Comparative Study of the Effect of Intravenous Lignocaine and Intravenous Dexmedetomidine for Attenuation of Haemodynamic Response to Laryngoscopy and Endotracheal Intubation
Comparative Study of the Effect of Intravenous Lignocaine and Intravenous Dexmedetomidine for Attenuation of Haemodynamic Response to Laryngoscopy and Endotracheal Intubation
Dr. Twinkle Jayesh Gupta 1*, Dr. Dimple K. Pandya2
1.3rd Year Resident, Department of Anaesthesia, NHL MMC, Gujarat University, Gujarat, Ahmedabad, India
2.Assistant professor, Department of Anaesthesia, NHL MMC Gujarat University, Gujarat, India.
*Correspondence to: Dr. Twinkle Jayesh Gupta, 3rd Year Resident, Department of Anaesthesia, NHL MMC, Gujarat University, Gujarat, Ahmedabad, India
Copyright
© 2024: Dr. Twinkle Jayesh Gupta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 August 2024
Published: 29 August 2024
Abstract
In most patients undergoing general anaesthesia, laryngoscopy and endotracheal intubation are required that can cause a large haemodynamic stress response, caused by sympathetic adreno-medullary response due to cortisol, norepinephrine, and epinephrine production. These can lead to tachycardia, hypertension, occasional dysrhythmias, angina, myocardial infarction or stroke. Considering the clinical significance of these changes stress attenuation is needed to blunt these responses. This is done by a variety of medications like lidocaine, deep inhalation anaesthetic, ganglion blocking drugs, calcium channel blockers, vasodilators, opioids, and adrenergic blockers.
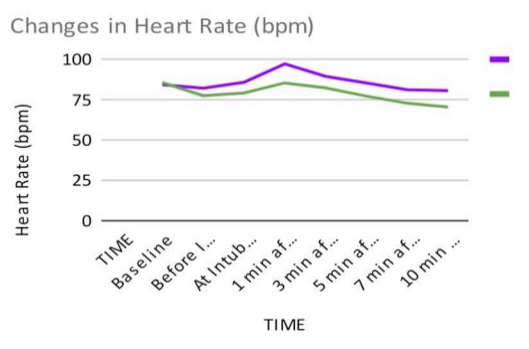
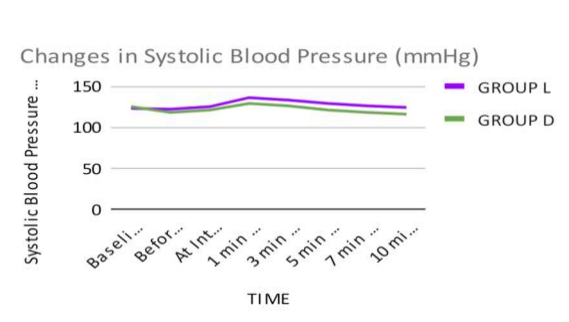
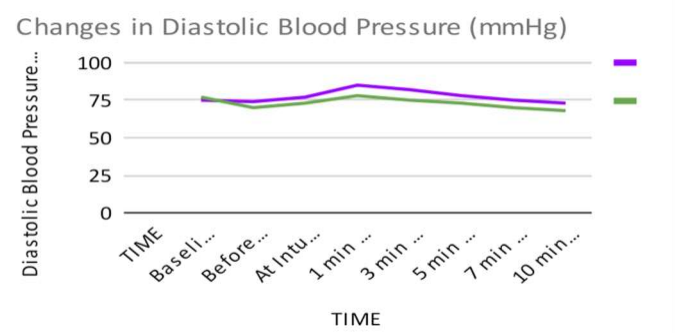
An observational study was carried out to compare the efficacy of intravenous Lignocaine and intravenous Dexmedetomidine in attenuation of haemodynamic response to laryngoscopy and endotracheal intubation. 50 patients aged 18-60 years of either sex belonging to ASA grade I or II were selected for the study and divided in two groups of 25 patients each. Group L: received Injection Lignocaine Hydrochloride 1.5 mg/Kg IV ( diluted to 10 ml with normal saline) 3 minutes before intubation ; Group D: received Injection Dexmedetomidine 1 mcg/kg IV infusion (diluted to 10 ml with normal saline) over 10 minutes before intubation. Changes in Heart rate, Systolic Blood Pressure, Diastolic Blood Pressure ,Mean Arterial Pressure, and Spo2 were recorded.
Keywords: Haemodynamic response, lignocaine, dexmedetomidine, laryngoscopy, endotracheal intubation.
Comparative Study of the Effect of Intravenous Lignocaine and Intravenous Dexmedetomidine for Attenuation of Haemodynamic Response to Laryngoscopy and Endotracheal Intubation
Introduction
Direct laryngoscopy and endotracheal intubation are almost always associated with haemodynamic changes due to reflex sympathetic discharge caused due to epipharyngeal and laryngo-pharyngeal stimulation. This increased sympathoadrenal activity may result in hypertension, tachycardia and arrhythmias.[1] The response is transient and occurs 30 seconds after intubation and lasts for less than 10 minutes. Hypertension and tachycardia may predispose an individual to development of pulmonary edema, myocardial insufficiency and raised intracranial pressure especially in patients with ischaemic heart disease, cerebrovascular disease, hypertension, old age, and diabetes mellitus.
There are various techniques and drugsused to reduce this pressor response to laryngoscopy and endotracheal intubation. They are:
Deeper plane of anaesthesia with Intravenous and Inhalational agents.
Topical anaesthetics- Topical Lignocaine gel 2%, Lignocaine aerosol 10%
IV Drugs:-
- Lignocaine 2% ;
- Vasodilators - Sodium Nitroprusside, Nitroglycerine ;
- Calcium channel blockers- Nifedipine, Verapamil, Diltiazem ;
- Beta blockers- Metoprolol, Esmolol, Labetalol ;
- Opioids- Fentanyl, Remifentanyl ;
- Alpha 2 adrenergic blockers- clonidine, dexmedetomidine ;
- ACE inhibitors- Ramipril, Enalapril ; ? Magnesium Sulfate , etc.
The present study was undertaken to compare the efficacy of intravenous Lignocaine (1.5 mg/kg) and intravenous Dexmedetomidine (1 mcg/kg) in attenuating haemodynamic response to laryngoscopy and endotracheal intubation.
Materials and Methods
This prospective comparative observational study was conducted on 50 patients who satisfied the inclusion criteria and were scheduled for elective surgery under general anaesthesia.Written informed consent was obtained from all the patients.
INCLUSION CRITERIA:
1. Patients with ASA physical status I and II.
2. Irrespective of sex , aged between 18-60 years.
EXCLUSION CRITERIA:
1. Patient refusal.
2. Patients known to have drug allergies.
3. Patients on treatment with beta blocker or calcium channel blocker drugs.
4. Patients with anticipated difficult airway , or those who required more than one intubation attempts or attempts lasting longer than 15 seconds .
5. Patients with Hypertension, Cardiac, Renal , Cerebral or Hepatic diseases.
6. Patients with asthma or reactive airway diseases.
7. Pregnant and lactating females.
Study protocol:
Preoperative assessment:
- Detailed history was taken, physical and systemic examination of all patients was done a day prior to operation. Airway assessment was done using Mallampati classification.
-Laboratory investigations like CBC, RFT, LFT, Blood Sugar, Serum Electrolytes, X-ray chest and ECG were reviewed.
-The nature of study and procedure was explained to the patient.
- Written informed consent was taken from the patient.
Preoperative preparation :
-All patients were kept Nil By Mouth at least for 6 hours before surgery.
- Anaesthesia machines , equipment and monitors were checked and emergency drugs were kept ready.
-Pulse oximeter , non invasive blood pressure monitor and ECG were attached and baseline readings were taken.
-After establishing intravenous access, an infusion Ringer lactate was started.
-All patients were premedicated with Inj. Glycopyrrolate (0.004mg/kg) iv ,Inj. ondansetron (0.08 mg/kg) iv and Inj. Fentanyl (1 mcg/kg) iv as premedication.
Method of Study
All patients were randomly divided into two groups of twenty-five patients each.
Group L: received Injection Lignocaine Hydrochloride 1.5 mg/Kg IV ( diluted to 10 ml with normal saline) 3 minutes before intubation
Group D: received Injection Dexmedetomidine 1 mcg/kg IV infusion (diluted to 10 ml with normal saline) over 10 minutes before intubation.
-All patients were preoxygenated with 100% oxygen for 3 minutes.
-Respective study drugs were injected as mentioned above.
-All patients were induced with Inj. Thiopentone Sodium 2.5 % (5 mg/kg) IV followed by Inj. Succinylcholine (2 mg/kg) IV to facilitate laryngoscopy and intubation.
-All patients were intubated with appropriate sized oral , portex, cuffed endotracheal tube within 15 seconds of Laryngoscopy
- Anaesthesia was maintained with O2 (50%) + N2O (50%), Sevoflurane and Inj. Vecuronium Bromide ( 0.08 mg/kg IV loading dose + 0.02 mg/kg IV in intermittent doses).
- Vitals to be monitored were Heart Rate, Systolic Blood Pressure, Diastolic Blood Pressure and SPO2.
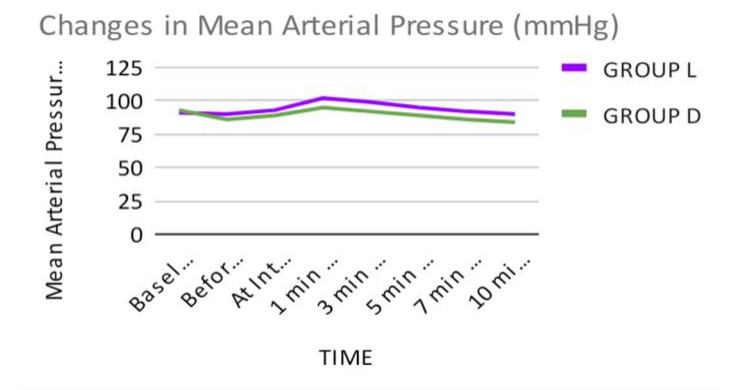
-Mean Arterial Pressure and Rate Pressure Product were calculated using following formulas:
Mean Arterial Pressure = 1/3 Systolic Blood Pressure ( mmHg) + 2/3 Diastolic Blood Pressure (mm Hg)
All the parameters were recorded at following stages:
Baseline
Before induction
At intubation
At 1 min, 3 min, 5 min, 7 min, 10 min after Intubation.
-At the end of surgery, residual neuromuscular blockade was reversed with Inj. Glycopyrrolate 0.008 mg/kg IV and Inj. Neostigmine 0.05 mg/kg IV.
- Extubation was carried out when the patient had adequately recovered from the effect of neuromuscular blockade with regular breathing pattern, good muscle tone/power, haemodynamic stability and was able to respond to verbal commands.
- We looked for adverse effects like allergic reactions, pruritus, bradycardia, hypotension and bronchospasm in both groups.Method of statistical analysis
- The results were expressed as Mean and Standard deviation. All recorded data was entered using Microsoft Excel software and analysed using Online software.
- Statistical analysis was done by using descriptive and inferential statistics using Chi-square test and students unpaired t test to find out the significance of various study parameters among the two groups.
P >0.05 : Not significant(NS)
P <0.05 : Significant(S)
P<0.001: Highly Significant (HS)
Observation
TABLE 1 : DEMOGRAPHIC DATA
|
Demographic data |
|
|||
|
Patient Data |
GROUP L |
GROUP D |
P value Inference |
|
|
Number Of Patients |
25 |
25 |
- |
|
|
Age( years) |
35.4 ± 7.64 |
36.8 ± 7.12 |
0.5059 NS |
|
|
Male:Female |
13:12 |
11:14 |
- - |
|
|
Weight (kgs) |
52.6 ± 5.58 |
54.8 ± 6.24 |
0.1951 NS |
|
|
ASA Grade |
I |
11 |
12 |
- - |
|
II |
14 |
13 |
||
Table-1 Compares the demographic characteristics of all the patients which were clinically comparable among both the groups ( p > 0.05) .