Clinicopathological Study of Gastrointestinal Endoscopic Biopsies in a Tertiary Care Center
Clinicopathological Study of Gastrointestinal Endoscopic Biopsies in a Tertiary Care Center
Pangeni P. Neera1*, Pradhan A2, Upadhyaya P2, Paudyal P2, Pokhrel S2, Kafle S3, Mudbhari B4
1: Neera P. Pangeni : Senior consultant pathologist, Kanti children hospital, Kathmandu, Nepal
2: Anju Pradhan: Professor, B.P. Koirala institute of health sciences, Dharan, Nepal
Paricha Upadhaya: Professor, B.P. Koirala institute of health sciences, Dharan, Nepal
Punam Paudyal: Additional Professor, B.P. Koirala institute of health sciences, Dharan, Nepal
Sairil Pokhrel: Associate Professor, B.P. Koirala institute of health sciences, Dharan, Nepal
3. Shankar Kafle: Assistant professor, Tribhuvan university teaching Hospital, Maharajgunj, Kathmandu, Nepal
4. Bandana Mudbhari: Consultant pathologist, Nisarga hospital and research center, Dhangadi, Nepal
*Correspondence to: Neera P Pangeni, Kanti children hospital, Maharajgunj, Kathmandu, Nepal.
Copyright
© 2025 Neera P Pangeni. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 April 2025
Published: 05 May 2025
Abstract:
Introduction:
Gastrointestinal (GI) mucosal lesions represent a significant health burden. Histopathological study of biopsy specimens is used to confirm endoscopic diagnosis in suspected malignancy or to rule out the endoscopically benign appearing lesions, and, to monitor the course, determine the extent of a disease, responses to therapy and for the early detection of complications.
This study aimed to determine the spectrum of GI mucosal lesions in endoscopic biopsies and correlate endoscopic diagnoses with histopathological findings in Eastern Nepal.
Methods:
A cross-sectional study was conducted at a tertiary care center (B.P. Koirala institute of health sciences, Dharan, Nepal) over a period of 12 months. Endoscopic biopsy samples were received in the pathology department and histopathological examinations were performed. Results were recorded and data analysis included descriptive statistics and diagnostic measurements.
Results:
A total of 45 endoscopic biopsies were analyzed (33 upper GI, 12 lower GI). The mean age of patients was 54.16 years. The most common site for upper GI biopsies was the stomach (37.7%), and for lower GI, it was the colon and rectum (11.11% each). Pain abdomen (86.67%) was the predominant clinical symptom. Histopathological diagnoses varied, with adenocarcinoma being common in both stomach and rectum. The correlation between endoscopic and histopathological diagnoses was evaluated.
Conclusion:
Adenocarcinoma was the most common malignancy in GIT except oesophagus in which squamous cell carcinoma was more common. Esophagitis, gastritis and inflammatory bowel disease were the most common types of non-neoplastic lesion in GIT. This study will be helpful to address the need for a definitive diagnosing tool based on which rapid presumptive diagnosis can be made in suspected cases and adequate treatment can be started accordingly.
Keywords: Benign, diagnosis, endoscopy, histopathology, malignant.
Clinicopathological Study of Gastrointestinal Endoscopic Biopsies in a Tertiary Care Center
Introduction
Gastrointestinal tract disorders are one of the most encountered problems in clinical practice with a high degree of morbidity and mortality.
Gastrointestinal tract can be sited for a wide variety of infections, inflammatory disorders, vascular disorders, mechanical conditions, toxic and physical reactions, including radiation injury and neoplasm. (1)
In the Gastrointestinal tract, the upper gastrointestinal tract consists of the buccal cavity, pharynx, esophagus, stomach and duodenum and the lower gastrointestinal tract includes part of the duodenum below the suspensory muscle and whole of the large intestine. (2)
Mucosal lesions are defined as different degrees of inflammation, erosion, pre-neoplastic and neoplastic lesions of the upper and lower gastrointestinal mucosa originating from the superficial layers/epithelial layer confined to the mucosae or in cases of ulcer and malignancy, penetrating up to the muscularis mucosae. (3)
Incidence of GIT mucosal lesions:
Worldwide gastric adenocarcinoma is the second most common cancer and carcinoma oesophagus is the sixth leading cause of death. (4) In Nepal, gastric carcinoma is the second most common among males. (5) Squamous cell carcinoma of oesophagus is usually seen in the middle third. Squamous cell carcinomas of the oesophagus emerge mainly through a sequence of chronic esophagitis, progressive dysplasia, carcinoma in situ, and finally invasive carcinoma. More than 90% of oesophageal cancers are squamous cell carcinoma or adenocarcinoma, while other types like melanoma, lymphoma, stromal tumours and neuroendocrine tumors are rarely seen. Oesophageal carcinoma shows a wide range of global variation in its incidence and this geographical distribution of cancer can be of great value for generations of epidemiological data. To facilitate diagnosis of different lesions, endoscopy and histology are complementary. (6).
Duodenal biopsies are now commonly performed as a part of Upper GI endoscopic procedure. Common indication for duodenal biopsy includes peptic ulcer disease, symptoms of malabsorption, neoplasia and infectious enteritis. Another common condition affecting duodenum is Celiac disease which is an enteropathy in certain predisposed individuals who have an inappropriate destructive inflammatory reaction against various proline rich proteins including gliadin in wheat, secalin in rye and horde in barley. This reaction may initially begin in proximal duodenum and may later involve entire stomach, small intestine and large intestine. The biopsies should be performed in patients with symptoms and laboratory abnormalities suggestive of
malabsorption and/or nutrient deficiency with the anti-celiac antibodies. Since the clinical presentation of celiac disease is often subtle, it is important that the threshold for biopsy be relatively low. (7)
The concept of a spectrum of histological appearances in chronic inflammatory bowel disease is useful and is convenient for practical assessment. This is particularly true in the early histological appearance of Crohn’s disease when the definitive criteria may not be present. From the point of view of histological assessment, particularly of mucosal biopsies, which are small, the histopathologist is faced with an apparent range of inflammatory changes falling within a continuous spectrum. The accurate histological diagnosis of chronic inflammatory bowel disease is dependent upon either multiple endoscopic biopsies or assessment of a surgically resected specimen. The key reasons for performing biopsies in patients with suspected active ulcerative colitis are to help confirm the diagnosis and to determine the extent of the disease. Knowledge of the latter is important for determining the best management strategy. (8)
In lower Gastrointestinal tract, endoscopy is more often done in patients who suffer from constipation and rectal bleeding although it is important in any kind of early detection of pathologic conditions of the colon. (9) In rare instances, where the gastrointestinal mucosa appears visually normal with endoscopy, the use of biopsy may still be beneficial in determining microscopic disease. In the lower GIT, obtaining biopsies from an endoscopically normal terminal ileum during colonoscopy adds little additional information. However, colonic biopsies of an endoscopically normal colon yield important information on aetiology in patients presenting with chronic diarrhoea. (10)
Most of the lesions are often subtle and cannot be identified during standard White light Endoscopy although the best chances of cure are associated with the early diagnosis. (11) Endoscopic appearances may be valuable in diagnosis but more accurate and detailed information results from histological examination of mucosal biopsy specimens. (12)
In most countries, gastrointestinal diseases are a large burden on the health-care services with GI pathology being a major workload of surgical pathology. There is a wide range of diseases that can affect the lower GIT, ranging from inflammatory to neoplastic lesion. (13) For diagnosis of abnormal mucosa is seen during endoscopy, specimens should be taken of both diseased and adjacent normal appearing mucosa and should be separately labelled to allow staging of the extent and severity of the disease. (14) The advent of fibre optic endoscopy in recent years has enormously extended the diagnostic possibilities in gastroenterology, assessment in certain situations, perhaps especially for small colorectal polyps. (15)
Gastroenterologists rely on the results of the biopsy for correct diagnosis. Therefore, histopathology is an essential complement to endoscopic examination. Hence, the present study aims to determine the spectrum of gastrointestinal lesions by endoscopic biopsy, make definite histopathological diagnosis of various neoplastic and non-neoplastic upper GI tract lesions and associate the endoscopic findings with histomorphology diagnosis.
Materials and Methods
Study Design and Setting:
A cross-sectional, hospital-based study was conducted at B. P. Koirala Institute of Health Sciences (BPKIHS), a tertiary care center in Eastern Nepal.
Inclusion and exclusion criteria: The study included all patients visiting BPKIHS who underwent endoscopy and had biopsy samples taken from gastrointestinal lesions. Patients who refused consent or had open excision biopsies were excluded. A total of 45 cases were included in the study. Patient data, including age, gender, clinical history, endoscopic diagnosis, and lesion site, were recorded.
Histopathological Examination:
Endoscopic biopsy specimens were preserved in 10% formaldehyde, processed, and stained with hematoxylin and eosin (H&E). Special stains were used when necessary. Special stains used were Periodic acid Schiff (PAS) stain to highlight micro-organism, carbohydrate/mucin, Alcian blue for carbohydrate, Combined Alcian blue – PAS technique and Mucicarmine Stain for mucin, Ziehl-Neelsen stain for tubercle bacilli, Gram stain for Gram positive and Gram-negative Bacteria, Giemsa stain to highlight micro-organism (example: Helicobacter pylori). Gastric biopsies were evaluated for mucosa type, surface epithelium, gastric pits, glands, metaplasia, H. pylori status, inflammation, dysplasia, and neoplasia.
Statistical Analysis:
Data was analyzed using SPSS 25. Descriptive statistics included percentages, proportions, ratios, and means. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for diagnostic measurements.
Results
Site Distribution of Biopsies:
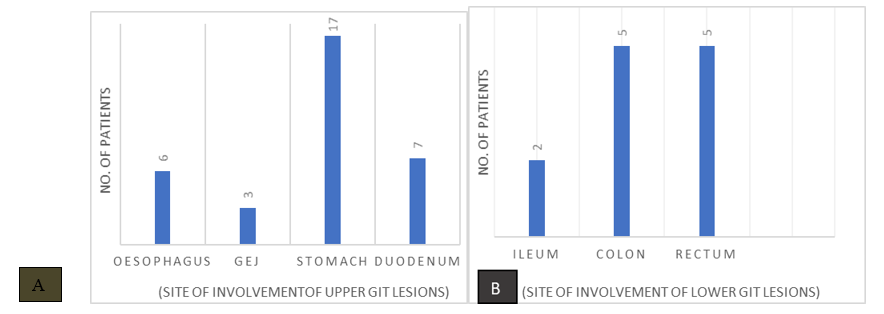
Of the 45 endoscopic biopsies, 33 were from the upper GI tract and 12 from the lower GI tract. In the upper GI tract, the most common site was the stomach (37.7%), followed by the duodenum (15.5%) and esophagus (13.33%). In the lower GI tract, the colon and rectum were the most common sites (11.11% each). (Fig. 1)
Figure 1: Sitewise distribution of: (A) upper GIT lesions (B) lower GIT lesions
Patient Demographics:
The age ranged from 26 to 85 years, with a mean age of 54.16 years. Most patients were female (57.8%). The most common occupation was housewife (37.8%). The predominant clinical symptom was abdominal pain (86.67%).
Clinical symptoms:
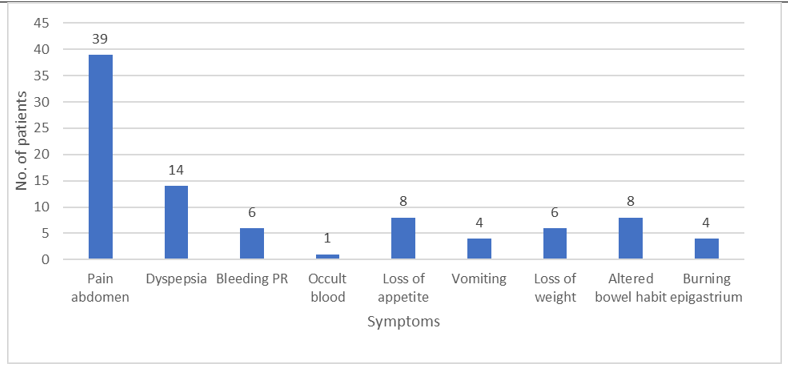
The predominant clinical symptom among the cases who underwent endoscopic biopsies was pain in abdomen (86.67 %) followed by dyspepsia (31.11%), loss of appetite (17.77%), altered bowel habit (17.77%), loss of weight (13.33%), vomiting (8.88%) and burning epigastrium (8.88%). (Fig.2).
In lower Gastrointestinal tract lesions, the most commonly presenting symptom was bleeding per rectum (13.33%) and occult blood positivity was found in 1 case i.e., 2.22%.
Figure 2: Presenting symptoms of the patients.
Endoscopic and Histopathological Findings:
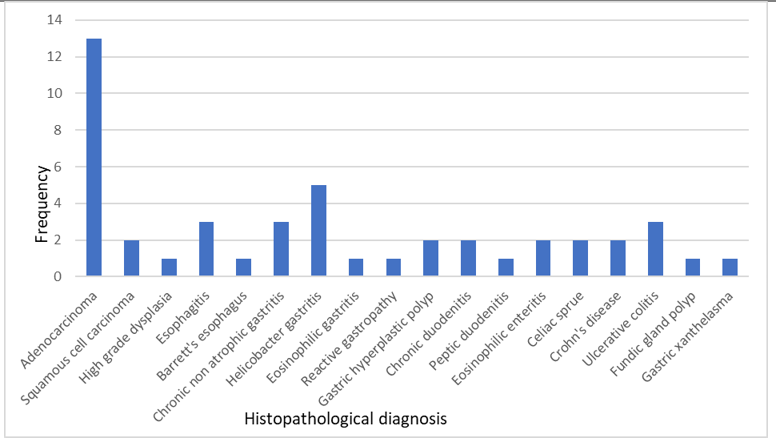
In the upper GI tract, endoscopic findings included suspected malignancy in the esophagus (3 cases), adenocarcinoma in the gastro-oesophageal junction (GEJ) (2 cases), and H. pylori gastritis in the stomach (4 cases). Histopathological diagnoses in the upper GI tract included esophagitis, squamous cell carcinoma, adenocarcinoma, Helicobacter gastritis, and chronic duodenitis. (Fig.3)
Similarly, in the lower GI tract, histopathological diagnoses included adenocarcinoma, Crohn's disease, and ulcerative colitis. (Fig.3)
Figure 3: Histopathological spectrum of GIT mucosal lesions
Association of Endoscopic and Histopathologic Diagnosis:
The association between endoscopic diagnosis and histopathologic diagnosis is tabulated in Table 1. Out of 45 endoscopic mucosal biopsies of GIT, three (3) cases were diagnosed as adenocarcinoma in both endoscopy as well as in histopathology. However, fifteen (15) cases were diagnosed as adenocarcinoma only in histopathology. The malignant cases that were not shown on endoscopy were diagnosed as adenocarcinoma in histopathology alone. Thus, sensitivity for endoscopic diagnosis for adenocarcinoma is 20%, specificity 100%, PPV 100%, NPV 71.43% and accuracy 73.33% which in comparison to histopathological diagnosis is lower.
Patients suspected of malignancy on endoscopy were diagnosed with variable benign and malignant conditions in histopathology. Thirteen (13) cases were suspected of malignancy on endoscopy. Seven (7) out of 13 cases suspected of malignancy in endoscopy were diagnosed as adenocarcinoma, two cases as squamous cell carcinoma, one esophagitis, two chronic non-atrophic gastritis and one chronic duodenitis on histopathological examination. The sensitivity for the endoscopically diagnosed ‘suspicious of malignancy’ was 31.82%, specificity 73.91%, positive predictive value 53.85% and negative predictive value 53.12%. The accuracy of endoscopic diagnosis in this case was only 53.33%. Here, the sensitivity of the endoscopy is very low as compared to histopathology and thus, we conclude that the histopathological examination is always necessary for the definite diagnosis of GIT mucosal lesions.
For benign lesions in upper GIT, Helicobacter gastritis was the commonest on histopathological diagnosis and on comparing the endoscopic diagnosis with the histopathology, specificity of endoscopic diagnosis was 90.00%, while sensitivity was 0.00%, PPV 0.00%, NPV 87.80% and accuracy of 80.00%. This might be because of the microscopic examination of organisms like H. pylori with the special stains which is impossible on endoscopic examination alone.
Similarly, for pangastritis on endoscopy, the specificity of diagnosing chronic non-atrophic gastritis was found to be 97.62 % and accuracy of 91.1% which is quite less compared to the histopathologic diagnosis. One case was diagnosed as erosive gastritis endoscopically but was diagnosed as adenocarcinoma in histopathology. Erosive gastritis when diagnosed on endoscopy, sensitivity was 25%, specificity 100%, PPV 100%, NPV 57.14 % and accuracy of 62.50 %. The sensitivity is found to be very low compared to the gold standard histopathological examination.
Cases diagnosed as eosinophilic gastritis on endoscopy were diagnosed as eosinophilic gastritis on histopathologic examination. The specificity was 97.73%, sensitivity 0.00%, PPV 0.00%, NPV 97.73% and accuracy 95.56%. But these values were found to be very low compared to the histopathologic examination. This might address the lower number of sample size and limited duration of the study leading to the poor association of these methods of diagnosis.
Table 1:Association of Endoscopic and Histopathologic Diagnosis:
|
S.N. |
Diagnosis |
Endoscopic (%) |
Histo-pathology (%) |
Diagnostic test for Endoscopic versus Histopathologic (Histo=gold standard) |
||||
|
Sensitivity (%) |
Specificity (%) |
Positive predictive value |
Negative predictive value |
Accuracy |
||||
|
1. |
Adenocarcinoma |
3 (6.66) |
15(33.33) |
20.00 |
100.00 |
100.00 |
71.43 |
73.33 |
|
2. |
Suspicious of malignancy |
13(28.88) |
22(48.8) |
31.82 |
73.91 |
53.85 |
53.12 |
53.33 |
|
3. |
Dyspepsia under evaluation |
1(2.2%) |
3(6.66) |
0.00 |
97.62 |
0.00 |
93.18 |
91.11 |
|
4. |
Helicobacter gastritis |
| ||||||