Management of Adenomyosis: A Single Centre Retrospective Study of Hysterectomy and LNG-IUS treated patients
Management of Adenomyosis: A Single Centre Retrospective Study of Hysterectomy and LNG-IUS treated patients
Kiran Mehndiratta1*, Shailesh Perdalkar2, Shubha Shankari3, Shubha Dadhich4, Rohit Ravindra Dusane5, Mary Boban6
1,3,4,6 - Department of Obstetrics and Gynaecology, NMC Specialty Hospital, Abu Dhabi, United Arab Emirates.
2,5- Clinical Research Department, NMC Healthcare, Abu Dhabi, United Arab Emirates.
*Correspondence to: Kiran Mehndiratta, Consultant Obstetrics and Gynaecology, NMC Specialty Hospital, Abu Dhabi, United Arab Emirates.
Copyright
© 2025 Kiran Mehndiratta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 June 2025
Published: 07 July 2025
Management of Adenomyosis: A Single Centre Retrospective Study of Hysterectomy and LNG-IUS treated patients
Introduction
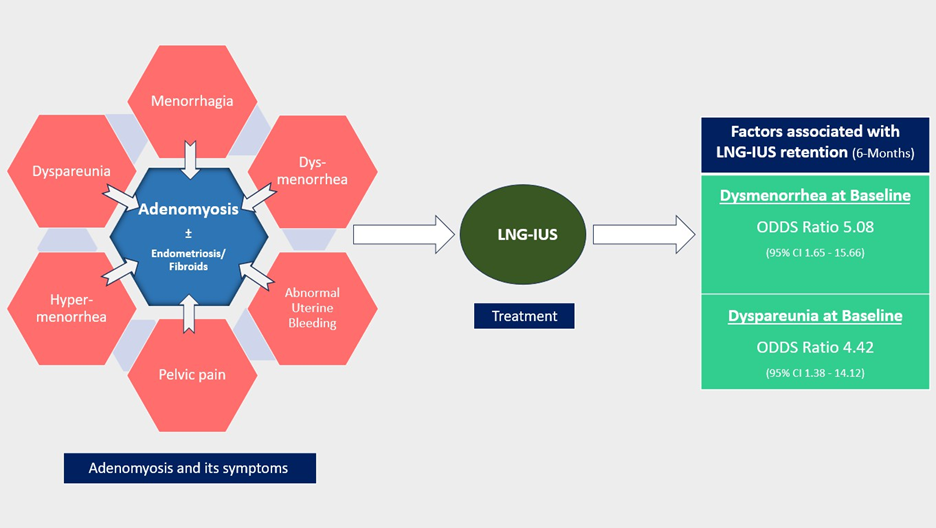
Adenomyosis (AD) is a common benign gynaecologic condition in which the uterus is enlarged due to myometrial invasion of endometrial glands and stroma. AD can be asymptomatic or may induce menorrhagia, dysmenorrhea, abnormal uterine bleeding, pelvic pain, hypermenorrhoea, dyspareunia, subfertility or infertility and eventually affecting the quality of life of the women[1–3]. The pathophysiology of AD is not clearly understood, but several theories have been proposed over the years [4–6]. Age, parity, and previous history of uterine surgery increase the risk of developing AD [Schrager S et al 2022]. The diagnosis of AD is challenging due to the overlapping symptoms with other gynaecological conditions such as endometriosis, uterine fibroids and leiomyomas.
Earlier AD could only be diagnosed by histopathological examinations in patients undergoing hysterectomy, thus the diagnosis was restricted to patients who did not wish to preserve their fertility. However, the advancement in imaging techniques such as transvaginal ultrasound (US) and Magnetic Resonance Imaging (MRI), have increased the scope of AD diagnosis in younger women as well [7]. The quest for a reliable biomarker for the diagnosis of AD is ongoing and currently, there are no clinically reliable biomarkers available for the same. However, studies investigating the use of CA 125[8], Cytokines [9], miRNA [10], proteomics and metabolomics [11, 12] for the diagnosis or differential diagnosis of AD have gradually increased. In future, AD diagnosis may be benefited from the integration of biomarkers along with imaging techniques.
Hysterectomy is the conventional treatment for symptomatic patients [13] as at present, there are no international guidelines on the clinical and surgical management of AD. Although hysterectomy is an effective treatment option for AD in providing long-term relief from symptoms and preventing recurrence, it often conflicts with patients' desire to preserve their fertility [14]. It is further compounded by surgical complications, short-term morbidities, and mortality [15]. Minimally invasive techniques like uterine artery embolization, laparoscopic myometrial resection/ electrocoagulation, endo-myometrial ablation, MRI-guided focused US (MRgFUS), high intensity focused ultrasound (HIFU), etc. are also used for symptomatic management of AD. Considering the lack of high-quality data, more evidence on these treatment options is warranted [16, 17].
The pharmacological management of AD includes NSAIDS for pain relief, hormonal therapies such as gonadotropin-releasing hormone analogues (GnRH-a), oral contraceptives, high-dose progestins, and hormone receptor modulators. According to the National Institute for Health and Care Excellence guidelines, the first-line treatment for AD should be an intrauterine hormone-releasing device [16, 18]. Levonorgestrel-releasing intrauterine system (LN-IUS) is a surgically implanted medical device that releases levonorgestrel locally into the uterus to treat the symptoms of AD temporarily [3]. LNG-IUS has been successfully used to treat AD to reduce blood loss and pain during menstruation by reducing the thickness of the myometrial junctional zone and total uterine volume. Low side effects, low serum hormonal levels, high local concentration around the site of implantation etc., are some of the advantages of LNG- IUS when compared to other oral treatments [19]. LNG-IUS offers a viable option for women who wish to preserve their fertility while managing AD [20]. Recently, there has been an increase in the number of studies that explore the benefits of LNG-IUS in AD either as a monotherapy or in combination with conservative surgeries/minimally invasive treatments/ other medical therapies. However, the studies investigating the duration and factors associated with the retention of the LING-IUS device are limited.
In this study, we intend to evaluate the characteristics of AD patients managed with either hysterectomy or LNG-IUS and explore the factors associated with the retention of LNG-IUS. Additionally, we studied the effect of LNG-IUS on pain levels in AD patients.
Materials and Methods
Study design:
A retrospective study was conducted at the Obstetrics and Gynaecology Department of NMC Specialty Hospital, Abu Dhabi. Patients aged 18 and above with confirmed diagnosis of AD between January 2020 and December 2022 were included in the study. AD with or without endometriosis and or fibroids, treated by hysterectomy or LNG-IUS were included and AD patients treated by other treatment modalities were excluded. The demographic and clinical characteristics of the patients were collected from medical records.
The diagnosis of AD was done based on symptoms of menorrhagia, menometrorrhagia, dysmenorrhea, dyspareunia, chronic pelvic pain, genitourinary or irritable bowel symptoms, supplemented with transvaginal US. Additionally, few patients had confirmed AD diagnosis by MRI.
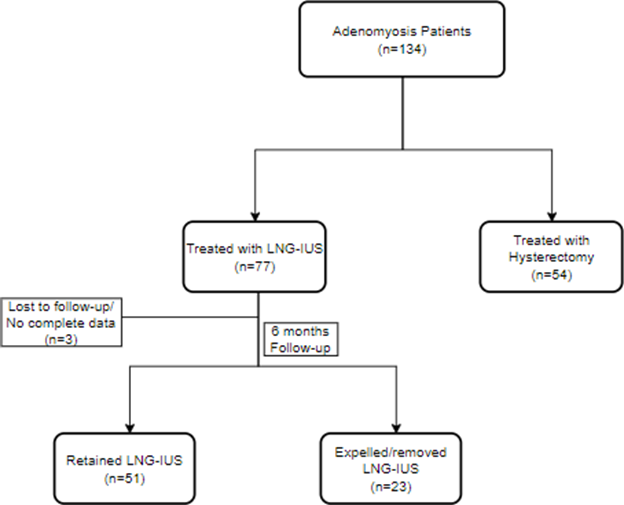
The patients enrolled in the study were divided into two groups based on their treatment options. Group I - AD patients treated with Hysterectomy and Group II – AD patients treated or managed with LNG-IUS. Group II was further categorized based on the status of Intrauterine Device (IUD); LNG-IUS at 6 months post insertion into Group II a- LNG-IUS retained and Group II b- LNG-IUS expelled (Figure 1). For Group I, only the baseline data was collected and for Group II Baseline, 1-month (1M), 3-month (3M) and 6-month (6M) follow-up data post-insertion of LNG IUS were collected.
Statistical analysis:
Write about the analysis. Variables with P-values below 0.05 in the univariate analysis were further examined in the multivariate analysis. All statistical analyses were performed using SPSS, version xxxx. p-values less than 0.05 were considered statistically significant.
Ethics approval:
This study was approved by the NMC Regional Research Ethics Committee (NMC/RREC/AUH/2023/0013).
Tables:
Table 1: Characteristics of patients in Group I and Group II
|
Variable |
LNG IUS |
Hysterectomy |
p value |
|
|
Age |
43.11 ± 5.45 |
45.49 ± 4.47 |
< 0.05 |
|
|
BMI |
28.14 ± 4.76 |
28.17 ± 5.08 |
0.8153 |
|
|
Parity |
0 |
0 |
5.00 (8.77) |
< 0.05 |
|
1 |
14.00 (18.92) |
14.00 (24.56) |
||
|
2 |
37.00 (50.00) |
28.00 (49.12) |
||
|
>=3 |
23.00 (31.08) |
10.00 (17.54) |
||
|
Coexisting Uterine disease (Endometriosis and or Fibroids) |
NO |
19.00 (25.68) |
6.00 (10.53) |
< 0.05 |
|
YES |
55.00 (74.32) |
51.00 (89.47) |
||
|
History of C-section SX |
NO |
31.00 (41.89) |
44.00 (77.19) |
< 0.05 |
|
YES |
43.00 (58.11) |
13.00 (22.81) |
||
|
History of D&C |
NO |
54.00 (72.97) |
45.00 (78.95) |
0.430 |
|
YES |
20.00 (27.03) |
12.00 (21.05) |
||
|
NRS pain score |
2 |
19.00 (25.68) |
15.00 (26.32) |
< 0.05 |
|
4 |
50.00 (67.57) |
30.00 (52.63) |
||
|
6 |
5.00 (6.76) |
12.00 (21.05) |
||
|
Haemoglobin |
≤8 |
11.00 (14.86) |
18.00 (31.58) |
0.072 |
|
8-10 |
19.00 (25.68) |
11.00 (19.30) |
||
|
>10 |
44.00 (59.46) |
28.00 (49.12) |
||
|
PBAC |
≤80 |
9.00 (12.16) |
7.00 (12.28) |
0.180 |
|
80-120 |
46.00 (62.16) |
27.00 (47.37) |
||
|
>120 |
19.00 (25.68) |
23.00 (40.35) |
||
|
Menorrhagia |
NO |
7.00 (9.46) |
10.00 (17.54) |
0.172 |
|
YES |
67.00 (90.54) |
47.00 (82.46) |
||
|
Irregular Bleeding |
NO |
3.00 (4.05) |
10.00 (17.54) |
< 0.05 |
|
YES |
71.00 (95.95) |
47.00 (82.46) |
||
|
Dysmenorrhea |
NO |
26.00 (35.10) |
18.00 (31.58) |
0.669 |
|
YES |
48.00 (64.86) |
39.00 (68.42) |
||
|
Dyspareunia |
NO |
37.00 (50.00) |
29.00 (50.88) |
0.921 |
|
YES |
37.00 (50.00) |
28.00 (49.12) |
||
Table 2: Baseline characteristic of the Group II patients
|
Variable |
Outcome |
||||||||
|
Yes |
No |
P value |
|||||||
|
BMI |
28.32 ± 4.31 |
27.77 ± 5.69 |
0.726 |
||||||
|
Age |
42.45 ± 5.70 |
44.57 ± 4.65 |
0.110 |
||||||
|
Parity |
1 |
12.00 (0.24) |
2.00 (0.09) |
0.268 |
|
||||
|
2 |
23.00 (0.45) |
14.00 (0.61) |
|
||||||
|
>=3 |
16.00 (0.31) |
| |||||||