Critical Care Nurses' Compliance and Barriers toward Ventilator-Associated Pneumonia Prevention Guidelines
Critical Care Nurses' Compliance and Barriers toward Ventilator-Associated Pneumonia Prevention Guidelines
Eidah Alrashdi1*, Nagwa Ibrahim Abbas Ghoneim2, Naimah Naif Ayidh Al Salem3, Norah Al Mutairi4, Mesfer Alrashidi5
1. Nursing specialist in Maternity hospital
2. Lecturer of Critical Care and Emergency Nursing, Faculty of Nursing, Tanta University, Egypt.
Assist prof, Nursing Department, Applied Medical Sciences College, UHB, SA. (orcid.org/0000-0003-1385-4024)
4,5. General Nurse Specialist, Hafer Albatin, Saudi Arabia.
*Correspondence to: Eidah Alrashdi, SA.
Copyright
© 2025: Eidah Alrashdi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 Sep 2025
Published: 22 Sep 2025
ABSTRACT
Background Background: Ventilator-associated pneumonia (VAP) is a significant and preventable health condition affecting thousands of patients annually. This condition can lead to severe complications and is potentially fatal. Despite the availability of numerous evidence-based preventive measures performed by nurses to reduce its incidence, compliance remains a challenge. This study aimed to evaluate critical care nurses' compliance with and barriers to ventilator-associated pneumonia prevention guidelines.
Methods: A cross-sectional study was conducted in the intensive care unit of King Khaled Hospital, KSA. Convenience sampling was utilized proportionally according to the number of staff in each department, resulting in a sample of 62 ICU nurses. Data was collected using a self-reported questionnaire consisting of socio-demographic characteristics of ICU nurses, compliance with VAP prevention guidelines assessment, and barriers to compliance assessment. Statistical analysis was performed using descriptive and inferential statistics to determine the relationships between knowledge levels and socio-demographic variables. Ethical approval was obtained.
Results: The study revealed that most participants were young, predominantly female, and held a bachelor degree, with 59.7% aged between 20–30 years and 82.3% being female. Most were Saudi nationals (87.1%), and nearly 70% had 1–5 years of ICU experience. Approximately 64.5% of participants worked in ICUs with 10–15 beds, but 83.9% had not received prior training on ventilator-associated pneumonia (VAP) prevention guidelines. Knowledge gaps were significant, with only 46.8% of nurses demonstrating satisfactory knowledge levels. Correct responses to key VAP prevention elements, such as recommended bed positioning (16.1%) and antibiotic course duration (30.6%), were particularly low. Statistical analysis indicated significant relationships between knowledge levels and factors like age, education, experience, and training, but no significant relationship with gender or job title. Barriers to compliance included nursing staff shortages, inadequate education, lack of supplies, and insufficient time for evidence-based procedures, showing the need for targeted interventions to enhance training, institutional support, and resource availability.
Conclusion The majority of nurses demonstrated unsatisfactory knowledge regarding VAP prevention guidelines, with statistically significant associations between knowledge and certain socio-demographic characteristics. The study recommends implementing educational and training programs to improve nurses' knowledge and adherence to VAP prevention guidelines, ultimately aiming to reduce the incidence of VAP among ventilated patients in the Saudi healthcare system.
Keywords: Critical care nurses' compliance - barriers - ventilator-associated pneumonia - prevention guidelines.
Critical Care Nurses' Compliance and Barriers toward Ventilator-Associated Pneumonia Prevention Guidelines
Introduction
Ventilator-associated pneumonia (VAP) is a significant healthcare issue, impacting thousands of patients annually and resulting in increased morbidity, mortality, and healthcare costs. This preventable infection is associated with mechanical ventilation, a life-saving intervention frequently used in intensive care units (ICUs). VAP accounts for approximately one-third of nosocomial pneumonia cases in ICUs, with the Centers for Disease Control and Prevention (CDC) reporting that 32% of pneumonia cases in U.S. acute care hospitals in 2015 were linked to ventilator use. Its impact extends beyond patient outcomes, as it increases ventilator dependency, prolongs ICU stays, and raises healthcare expenses (Fernando et al., 2020; Papazian, Klompas, & Luyt, 2020).
VAP is defined as a pulmonary infection occurring in mechanically ventilated patients (MVPs) after at least 48 hours of endotracheal intubation. The prevalence of VAP is alarmingly high, ranging from 9% to 27%. Intubated patients are particularly vulnerable during the first five days of ventilation, when the risk of developing VAP is highest. Globally, the incidence of VAP varies, with developing countries experiencing the highest rates. In the United States, VAP incidence is reported to be between 1.1 and 7.4 episodes per 1,000 ventilator-days in adult ICUs. However, the International Nosocomial Infection Control Consortium (INICC) reported a significantly higher incidence rate of 14.7 episodes per 1,000 ventilator-days in 43 developing countries, including regions in Latin America, Asia, Africa, and Saudi Arabia (Mohamed et al., 2023).
Studies in Saudi Arabia showed the critical nature of VAP in ICUs. Research analyzing infection rates across 12 Ministry of Health hospitals revealed that VAP was the most common deviceassociated healthcare-associated infection (DA-HAI), accounting for 57.4% of such cases. Further analysis by the INICC in five Saudi cities between 2013 and 2015 reported an incidence rate of 7.5 episodes per 1,000 ventilator-days. These statistics illustrate the disparity in VAP incidence globally, which is influenced by differences in surveillance models, healthcare resources, and prevention practices (Gaid et al., 2018; Abdulla et al., 2023). The financial and clinical burden of VAP is profound; in Saudi Arabia, each episode of VAP is associated with an additional $40,000 in hospital costs, an average ICU stay extension of 17.5 days, and an excess mortality rate of 31.8% (Gaspar et al., 2023).
The complications of mechanical ventilation are multifaceted, with VAP being one of the most significant. The endotracheal tube (ETT) serves as a conduit for bacterial migration from the oral cavity to the lungs, reducing salivary flow, impairing mucus clearance, and inhibiting the cough reflex. These factors contribute to bacterial colonization and the development of VAP. This risk is heightened in patients requiring intubation for conditions such as airway protection, surgeries, or reduced consciousness (Weber, 2023). The consequences are severe; patients who develop VAP have a five to ten times higher risk of acquiring nosocomial infections and experience increased mortality rates, with death occurring in 33% of cases (Mumtaz et al., 2023).
Efforts to prevent VAP in critical care settings have led to the development of various strategies, including elevating the head of the bed, providing oral care, administering prophylactic antibiotics, and adhering to care bundles. These measures have been shown to decrease ventilator dependency and ICU stays. Notably, VAP bundles, which combine multiple evidence-based interventions, are particularly effective. The duration of mechanical ventilation remains the most significant risk factor, and reducing ventilator days is key to prevention (Coelho, Moniz, Guerreiro, & Póvoa, 2023; Safavi et al., 2023). Oral care, a cornerstone of VAP prevention, has been shown to significantly reduce respiratory tract infections when performed consistently and correctly. Research showed the importance of nurse education, technique, and compliance in the successful implementation of these measures (Alotaibi, 2023).
Despite the availability of clinical guidelines, adherence to VAP prevention strategies remains inconsistent. Barriers such as institutional differences, limited awareness, and variability in training contribute to this gap between ideal and current practice. In Saudi Arabia, the challenges of implementing these guidelines are further compounded by resource constraints and diverse healthcare settings. Addressing these issues is essential for improving nurse compliance and ensuring consistent application of evidence-based measures (Alotaibi, 2023; Wolfensberger et al., 2023). Nurses are at the forefront of VAP prevention, given their direct contact with patients and their responsibility for implementing the majority of interventions.
The global burden of VAP, coupled with its clinical and financial consequences, showed the importance of effective prevention strategies. In ICUs, where patients are most vulnerable, ensuring adherence to evidence-based guidelines is critical. This study aimed to evaluate the compliance of critical care nurses with VAP prevention measures and identify the barriers hindering adherence. By bridging the gap between knowledge and practice, healthcare institutions can significantly reduce the incidence of VAP, improve patient outcomes, and optimize healthcare resources. Empowering nurses through education, institutional support, and standardized guidelines is essential in combating this preventable yet impactful infection.
Methods
Study Design The research employed a cross-sectional study design, which allowed for the analysis of relationships among variables without establishing causality. This design is particularly useful for capturing data at a single point in time to assess critical care nurses’ compliance with ventilator-associated pneumonia (VAP) prevention guidelines and the barriers they encounter in implementing these measures (Setyawati, Lu, Liu, & Liang, 2020).
Study Setting This study was conducted in the intensive care unit (ICU) of King Khaled Hospital, located in Hafr Al-Batin, Saudi Arabia. King Khaled Hospital is a leading healthcare facility in the region, providing a wide array of medical services to the city and its surrounding areas. The hospital offers specialties such as emergency care, general medicine, surgery, pediatrics, obstetrics and gynecology, orthopedics, cardiology, and neurology. Equipped with state-of-the-art medical technology, the hospital is designed to deliver high-quality, patient-centered care.
Sampling The target population for the study comprised staff nurses working in the ICU of King Khaled Hospital who had at least one year of experience in bedside patient care. A convenience sampling method was utilized, proportionally representing staff from different departments. Inclusion criteria ensured a diverse sample, encompassing nurses of all qualifications, varying years of experience, different nationalities, and both genders. Participation was voluntary, with only those willing to partake in the study included in the sample.
Tools of Study A self-reported questionnaire was employed to collect data, divided into three distinct sections. The first section focused on the sociodemographic characteristics of ICU nurses, including age, gender, nationality, marital status, education level, position, years of ICU experience, the type of ICU, the number of beds, and prior education on ventilator management and VAP prevention. The second section assessed nurses’ compliance with VAP prevention guidelines through 11 multiple-choice questions covering knowledge of definitions, causes, guidelines, and complications. Responses were scored, with one point for each correct answer, yielding a total score of 11. Compliance was categorized as good (75–95%), average (60–74%), or poor (below 60%). The third section investigated barriers to guideline adherence, utilizing an 18-item Likert scale with responses ranging from strongly disagree to strongly agree. This section explored challenges related to knowledge gaps, workload, institutional factors, communication, and patient safety concerns.
Tool Validity and Reliability The validity of the questionnaire was assessed by five experts in the critical care nursing field, achieving a Content Validity Index (CVI) score of 97%. The reliability of the tool was measured using Cronbach's alpha, with a coefficient of 0.57. Adjustments and refinements were made based on feedback from the experts and results of a pilot study to enhance the clarity and applicability of the tools.
Pilot Study A pilot study was conducted with 10% of the target population to test the clarity and usability of the research tools. This phase also helped estimate the time required for data collection and identify potential challenges. Participants from the pilot study were excluded from the main research to ensure data integrity.
Compliance with VAP Prevention Guidelines The study revealed varying levels of compliance with VAP prevention practices among ICU nurses. High compliance rates were observed for practices such as head-of-bed elevation (70–100%) and oral care with chlorhexidine (60–100%). Moderate compliance was noted for daily sedation vacations and readiness-to-extubate assessments (60–88%). Lower compliance rates were recorded for interventions such as subglottic suctioning (30–75%), ventilator circuit changes only when necessary (40–80%), and the use of endotracheal tubes with subglottic suction ports (30–80%).
Barriers to VAP Prevention Guideline Adherence The study evaluated the presence and level of barriers affecting adherence to ventilator- The study identified and evaluated key barriers affecting adherence to ventilator-associated pneumonia (VAP) prevention guidelines, categorized into knowledge gaps, workload challenges, institutional factors, communication issues, and patient safety concerns. Knowledge deficits emerged as a primary barrier, with nurses lacking familiarity with current guidelines and uncertainty about certain interventions' effectiveness. Workload pressures, such as heavy patient assignments and high acuity levels in ICUs, further limited time for implementing preventive measures. Institutional shortcomings, including inadequate supplies like subglottic suction catheters and the absence of clear protocols, compounded the problem. Poor interdisciplinary collaboration and disagreements between nurses and physicians regarding certain practices also hindered adherence. Additionally, nurses expressed concerns that some measures, such as sedation holds, might compromise patient safety or comfort, creating reluctance to implement them. These findings showed the need for targeted strategies to address these barriers, including education, improved staffing, clearer institutional policies, and enhanced communication, to improve adherence and patient outcomes in ICU settings.
Statistical Analysis Data were coded, entered, and analyzed using the Statistical Package for Social Sciences (SPSS) version 23. Statistical techniques were applied to achieve the study’s objectives, with results presented in a structured format. Sociodemographic data were visualized through figures, while tables and charts were used to depict nurses’ knowledge of VAP prevention and barriers to compliance. This comprehensive approach provided insights into the factors influencing adherence to VAP prevention guidelines and showed areas for improvement in ICU nursing practices.
Ethical Considerations Ethical approval was obtained from the Ethics Committee of the High Institute of Public Health. Participants received comprehensive information about the study’s purpose, benefits, risks, and voluntary nature. Written consent was secured before participation, and nurses were informed of their right to withdraw at any time without consequences. The study ensured anonymity, confidentiality, and privacy throughout the research process, safeguarding the safety and rights of all participants. Following official approval from King Khaled Hospital’s administration, data collection was conducted over a designated period. The researcher personally explained the study’s objectives and procedures to participants and clarified how to complete the questionnaires. Data was gathered during morning shifts, with interviews conducted at times convenient for the nurses.
Results
Socio-Demographic Characteristics of Participants
The socio-demographic characteristics of the critical care nurses are detailed in Table 1. The age ranged from 20 to 45 years. The majority, 37 nurses (59.7%), were within the 20–30-year age group, followed by 23 nurses (37.1%) in the 30–40-year range. Only a small proportion of nurses (3.2%) were aged 36–45 years, and 3.6% were 40 years or older. Regarding gender, the overwhelming majority of participants were female (82.3%). In terms of education, 75.2% of the nurses held a bachelor's degree. Most participants (87.1%) were Saudi nationals, with 40.3% being single.
Concerning their professional roles, 82.3% held the position of staff nurse. A significant portion of the nurses (69.4%) had between 1–5 years of experience, and 72.6% worked in ICUs. Additionally, 64.5% worked in ICUs with 10–15 beds. These characteristics showed the varied yet predominantly young, educated, and female composition of the critical care nursing workforce at the studied hospital.
Table (1): Percentage distribution of the studied critical care nurses according to their sociodemographic data (n=62)
|
Participants characteristics |
N |
% |
|
Age |
|
|
|
20–30 Years |
37 |
59.7% |
|
30–40 Years |
23 |
37.1% |
|
≥40 Years |
2
|
3.2%
|
|
Gender |
|
|
|
Male |
11 |
17.7% |
|
Female |
51 |
82.3% |
|
Nationality |
|
|
|
Saudi |
54 |
87.1% |
|
Non-Saudi |
8 |
12.9% |
|
Religion |
|
|
|
Muslim |
59 |
95.2% |
|
Non-Muslim |
3 |
4.8% |
|
Marital Status |
|
|
|
Single |
25 |
40.3% |
|
Married |
35 |
56.5% |
|
Divorced/Widowed |
2 |
3.2% |
|
Job Title/Current Position |
|
|
|
Staff Nurse |
51 |
82.3% |
|
In-Charge Nurse |
10 |
16.1% |
|
Head Nurse |
1 |
1.6% |
|
Years of Experience |
|
|
|
1–5 Years |
43 |
69.4% |
|
6–10 Years |
10 |
16.1% |
|
>10 Years |
9 |
14.5% |
|
Type of Critical Care Unit |
|
|
|
ICU |
45 |
72.6% |
|
CCU |
6 |
9.7% |
|
PICU |
3 |
4.8% |
|
NICU |
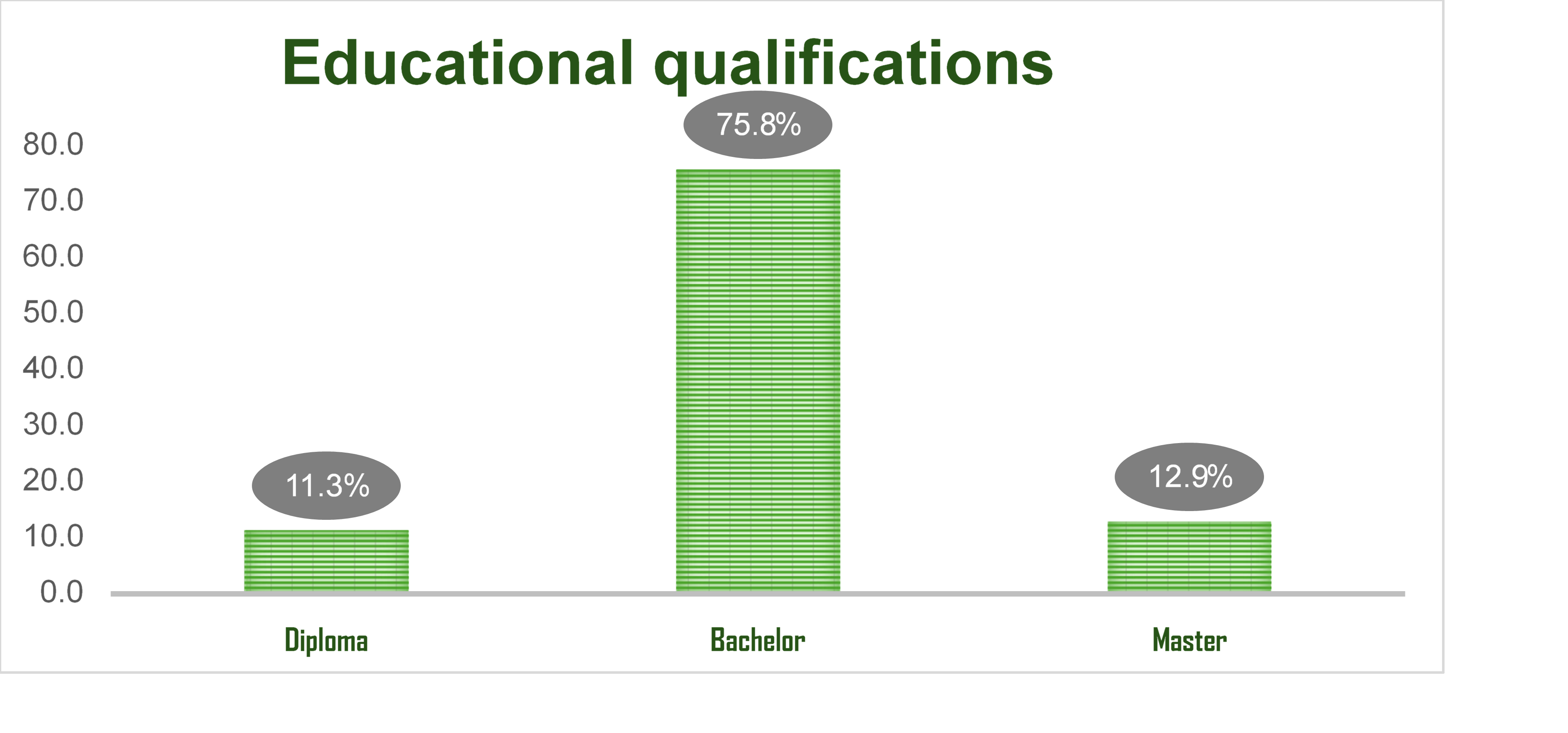
Figure 1
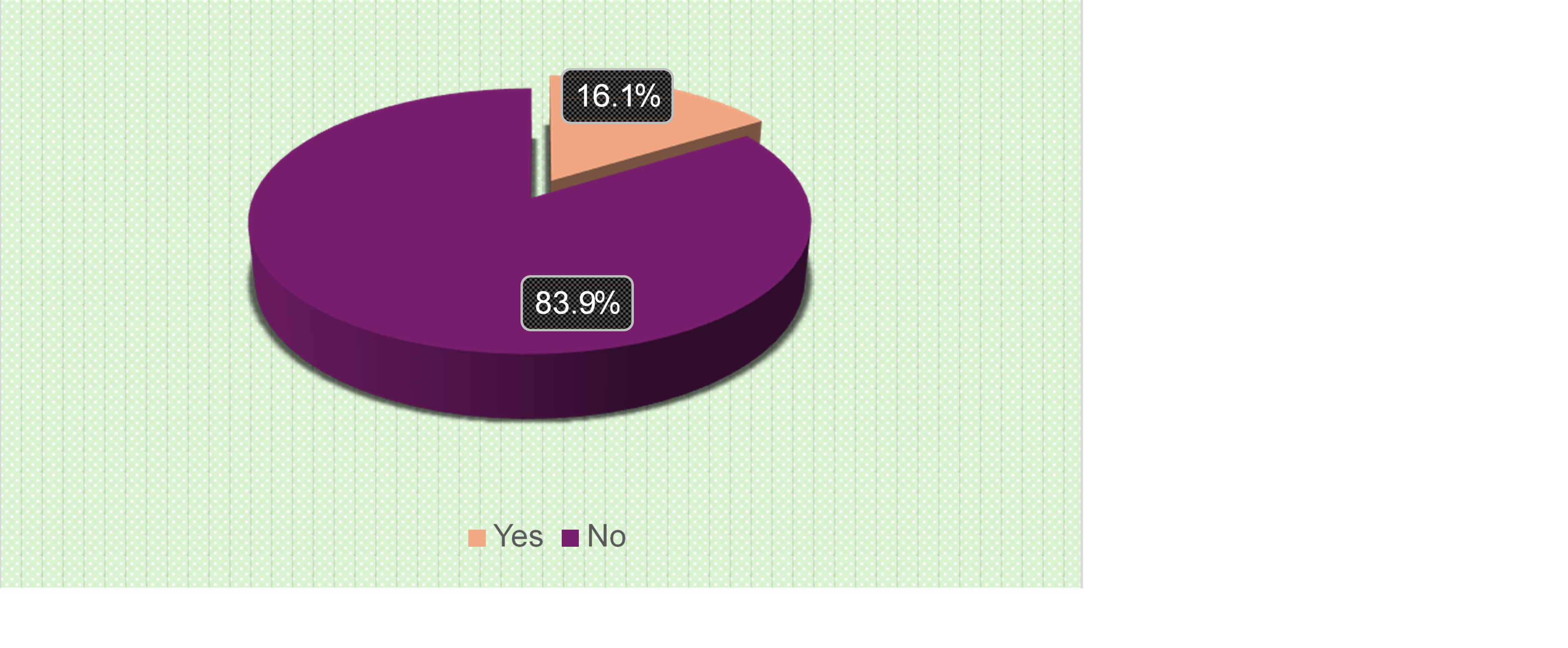
Figure 2
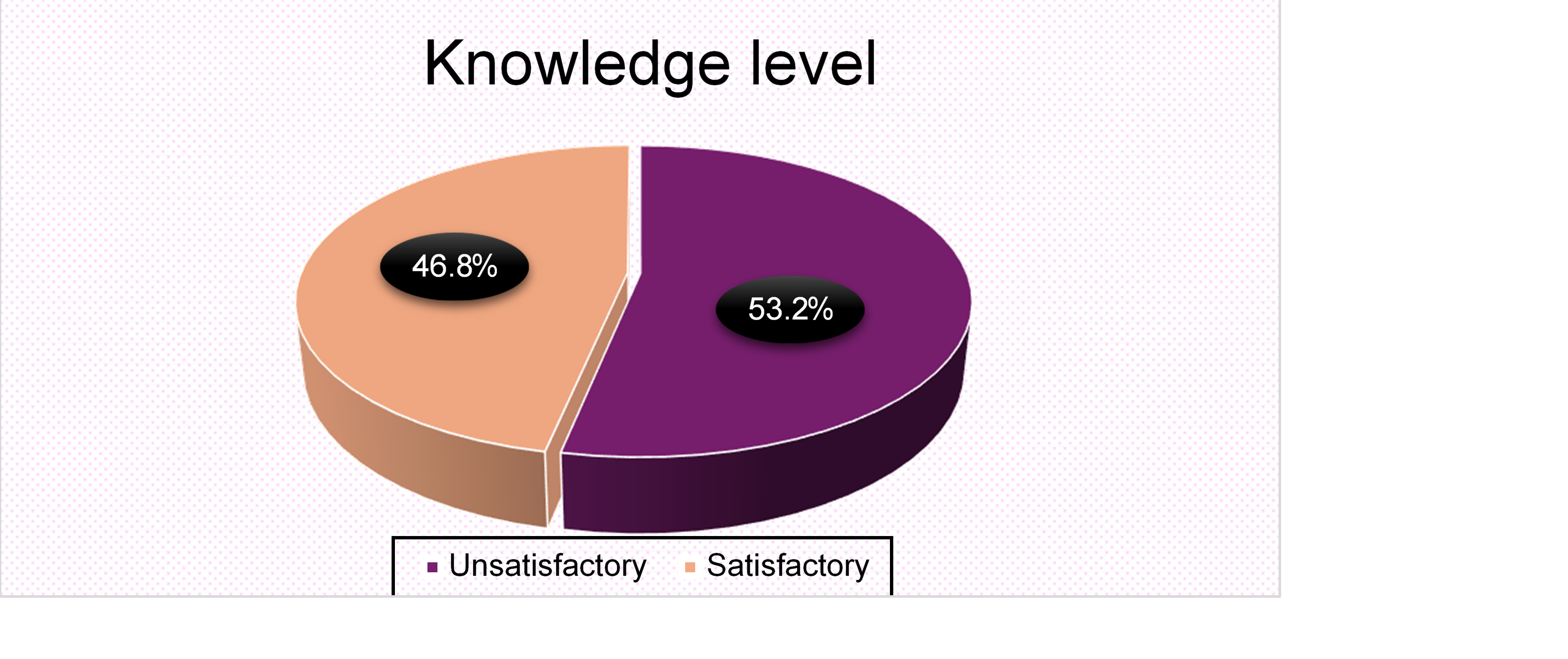
Figure 3
|