Critical Care Nurse’s Perceptions on Supportive Behaviors and Barriers Impeding the Provision of End-Of-Life Care in the Intensive Care Unit in Hafr- Al-Batin, Saudia Arabia
Critical Care Nurse’s Perceptions on Supportive Behaviors and Barriers Impeding the Provision of End-Of-Life Care in the Intensive Care Unit in Hafr- Al-Batin, Saudia Arabia
Naimah N. Al Salem1*, Nagwa Ibrahim Abbas Ghoneim2, Eidah khalaf Alrashdi3, Sharooq Dhaher Alenezi4
1. Nursing specialist in science of critical care nursing , Hafer-Albatin-Saudi Arabia.
2. Lecturer of Critical Care and Emergency Nursing, Faculty of Nursing, Tanta University, Egypt. Assist prof, Faculty of Nursing, UHB, SA. (0000-0001-6400-4121).
3. Nursing specialist in science of critical care nursing, Hafer-Albatin-Saudi Arabia.
4. Nursing specialist - Riyadh - Saudi Arabia
*Correspondence to: Naimah N. Al Salem, Nursing specialist in science of critical care nursing , Hafer-Albatin-Saudi Arabia.
Copyright
© 2025: Naimah N. Al Salem. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 Sep 2025
Published: 22 Sep 2025
ABSTRACT
Background: End-of-life care is an approach to a terminally ill patient that shifts the focus of care to symptom control, comfort, dignity, quality of life, and quality of dying. The aim of this study is to investigate the critical care nurse’s perceptions on supportive behaviors and barriers impeding the provision of end-of-life care in the intensive care unit.
Methodology: A descriptive cross-sectional study design and a convenience sampling technique of staff nurses who worked in Central Hospital and Maternity and Children's Hospital - Hafr Al Batin, SA. Two tools used in this study Tool 1: An electronic a questionnaire sheet it consists of sociodemographic characteristics and ICU nurses’ perceived barriers and supportive behaviors to end-of-life care. Tool 2 : Performance of end-of-life care.
Results: Concerning critical care nurses’ performance of plan and implementation in end-of-life care. It was found that 26% of respondent report that provide physical care including oral care and position change to dying patients not performed. Similarly, educate dying patients and their families on their symptoms and coping method, and Document assessments and nursing intervention about dying (or end of life) patient care. Also, 32% of them reported that refer to clergy or give spiritual care based on the spiritual needs of dying (or terminally ill) patients and their families not performed at all.
Conclusion: The findings of this study highlighted the top items perceived by critical care nurses as severe barriers to providing EOL care to die patients and their families. These barriers involve nurses’ heavy workload, poor ICU design, families who do not understand what life-saving measures really mean, lack of nursing education and training regarding family grieving and quality EOL care, and not knowing patients’ wishes regarding continuing with tests and treatments.
Key words: Critical care nurse’s, Perception, Supportive behaviors, Barriers, End-of-life care, Intensive care unit
Critical Care Nurse’s Perceptions on Supportive Behaviors and Barriers Impeding the Provision of End-Of-Life Care in the Intensive Care Unit in Hafr- Al-Batin, Saudia Arabia
Introduction
The ICU is currently the setting where the highest number of deaths occur in most hospitals. The global burden of ICU mortality has significant implications, leading to substantial losses in productivity and financial costs. In the United States alone, there are approximately four million annual ICU admissions, with an average death rate ranging from 8% to 19%. Developed continents like North America, Oceania, Asia, and Europe have lower ICU mortality rates, with rates of 9.3%, 10.3%, 13.7%, and 18.7%, respectively. On the other hand, in South America and the Middle East, the mortality rates are higher, at 21.7% and 26.2%, respectively. In comparison to other developed continents, Africa has a high ICU mortality rate. Studies conducted in Nigeria, Tanzania, and Kenya showed that the ICU mortality rates of 32.9%, 40.1%, and 53.6%, respectively (Ermiyas M et al 2024). In Saudi Arabia, study conducted by (Al Khalfan et al, 2021) they noted that the technological developments in patient care, mortality remains high with significant variances in rates due to differences in patient case, treatment plans, and organization of care. Typically, the global average of ICU mortality rates ranges from 8% to 20%.
End-of-life care is an approach to a terminally ill patient that shifts the focus of care to symptom control, comfort, dignity, quality of life, and quality of dying rather than treatments aimed at cure or prolongation of life. At this stage, the focus of care should shift from aggressive life-sustaining interventions to end-of-life care (EOLC). Therefore, critical care nurses must often switch the emphasis of their care from curative measures to EOLC (Jigeeshu V 2020). The provision of PC has shown many benefits including improved quality of life and reduced hospital admission and hospital stays. Due to its benefits, the provision of PC is encouraged to be integrated into a health system, including in the intensive care unit (ICU) (Christantie E et al 2022).
The ICU environment presents unique challenges in delivering end-of-life care due to the critical nature of patients' conditions and the high-intensity interventions typically provided. However, there are key principles and practices that guide end-of-life care in the ICU such as communication, symptom management, psychosocial support, respect for dignity and autonomy, family involvement, ethical considerations, and palliative care integration (Chen, M et al, 2019) (Tang et al., 2021). Studies have shown that end-of-life care can improve the quality of death, shorten the length of stay, and reduce the cost of hospitalization in ICU (Choi et al., 2019 & Khandelwal et al., 2017). Bereavement Support such as Effective communication is essential in end-of-life care. Clear, compassionate, and ongoing communication with patients, their families, and the healthcare team is crucial. It involves discussing prognosis, treatment options, goals of care, and addressing concerns and preferences. (Riegel, et al., 2021). Critical care nurses play a vital role in providing emotional and psychosocial support to patients and their families. (Chen, M et al, 2019).
After a patient's death, critical care nurses provide bereavement support to families. This involves offering condolences, facilitating memorial rituals or ceremonies, connecting families with grief support services, and providing resources for coping with loss.(Ozga, Wo?niak, & Gurowiec, 2020). Some of the common challenges as decision-making complexity as End-of-life decisions in the ICU can be complex due to the critical nature of patients' conditions and the presence of multiple treatment options. Balancing the desire to prolong life with the patient's wishes and quality of life considerations can create ethical dilemmas and decision-making challenges for both patients and their families (Majed A, et al., 2024).
Critical care nurses play a crucial role in providing care and support to critically ill patients and their families in high-stress environments. Supportive behaviors are essential in helping patients cope with their conditions, promoting their well-being, and assisting them in their recovery. (Yousef S, et al 2024). Critical care nurses focus on assess and monitor patients regularly, administer medications as prescribed, and implement non-pharmacological interventions to provide comfort (Beckstrand, et al., 2023). Several researchers (Hynes, Coventry, & Russell, 2021) (Effendy, Yodang, Amalia, & Rochmawati, 2022) (Palma, et al., 2022) (Almalki, Boyle, & O’Halloran, 2024) (Metaxa, 2021) they investigated the perceptions of critical care nurses regarding barriers and supportive behaviors to providing EOL care to dying patients and their families in different parts of the world, but research in this area in KSA is scarce. Hence, the current study was carried out to assess nurses’ perceptions of barriers and supportive behaviors in providing EOL care to dying patients and their families in ICUs of at Hafar Al-Batin Central Hospital and Maternity and Children's Hospital - Hafar Al Batin, Saudi Arabia. The aim of this study is to investigate the critical care nurse’s perceptions on supportive behaviors and barriers impeding the provision of end-of-life care in the intensive care unit.
Methodology
Study setting: The study conducted at Hafr Al-Batin Central Hospital and Maternity and Children's Hospital - Hafr Al Batin, Saudi Arabia.
Study design: A descriptive cross-sectional study design was utilized to conduct this study.
Target population:
A convenience sampling technique with random selection of staff nurses who worked in the previously selected settings with inclusion criteria of: (1) registered nurse, involved in direct patient care, (2) have experience in the ICU for at least one year. (3) Both males and females of all ages, and (4) prior experience in caring for dying patients (5) willing to participate in the study and (6) available at the time of data collection.
Tools of this study:
The two tools used in this study adapted from Beckstrand, Larsen, Macintosh, Rasmussen, Luthy, & Lyman, (2023). to elicit critical care nurses’ perceptions of barriers and supportive behaviors in providing End of Life Care (EOLC) to dying patients and their families.
Tool 1: An electronic a questionnaire sheet and it consists of two parts.
Part 1: it involved information about nurses’ socio-demographic characteristics such as age, gender, educational level, job title, type of the ICU where they worked, years of working experience in the ICU, and working hours, current position and number of dying patients cared for.
Part 2: a questionnaire on ICU nurses’ perceived barriers and supportive behaviors to end-of-life care.
Using the National Survey of Critical Care Nurses’ Perceptions of End-of-life-Care developed by Beckstrand, lamoreaux, Luthy, & Macintosh, (2017), will be used to identify barriers to and supportive behaviors for end-of-life care. It consists of 29 items focusing on barriers, and 24 items on supportive behaviors. The questionnaire uses a six-point Likert-type scale 0 to 5 to measure the intensity and frequency of barriers (0 = not an obstacle, 1 = extremely small, 2 = small obstacle, 3 = medium obstacle, 4 = large obstacle, 5 = extremely large). frequency scores (0 = never occurs, 1 = almost never occurs, 2 = sometimes occurs, 3 = fairly often occurs, 4 = very often occurs, 5 = always occurs). The supportive behavior’s part is scored in the same way as the barrier part. Using the mean item score to determine the intensity and frequency of each item, the perceived intensity of each item is the mean of intensity multiplied by the mean of frequency. The higher the item’s perceived intensity score, the more prominent the barrier or supportive behavior becomes. Each item’s intensity mean is multiplied by the item’s frequency mean to obtain a perceived intensity score for the barrier or a perceived supportive behavior score for the supportive behavior.
Tool 2 : Performance of end-of-life care:
An electronic self-questionnaire sheet regarding the performance of end-of-life care will be developed by the researcher after reviewing the literature (Jung, et al., 2023). These items were rated on a 4-point Likert scale, with “not performing at all” scoring 1 point, “not performing” scoring 2 points, “performing” scoring 3 points, and “always performing” scoring 4 points. A higher score signifies a higher level of performance in end-of-life care (Jung, et al., 2023).
Ethical considerations:
1. The researcher seeks the approval of the Ethics Committee of the High Institute of Public Health to conduct the research.
2. A written consent was taken from all study participants after explanation of the purpose and benefits of the research.
3. Anonymity and confidentiality assured and maintained.
4. There is no conflict of interest.
5. An agreement obtained from the selected hospital for data collection. Voluntary agreement of nurses who meet the inclusion criteria to fill in the questionnaires and be part of the study considered with written consent from participants.
Validity: The validity of the tool was tested by measuring its Content Validity Index (CVI) by 5 experts in the critical care nursing department field and it’s equaled by a statistician (95%). The tools will be tested for their face and content validity by five experts in the relevant field of the study and accordingly the necessary modification will be done.
Reliability: Reliability test was done using Cronbach's alpha test and it’s equaled (r) by a statistician (0.56).
A pilot study: A pilot study carried out for (10%) of the study subjects randomly selected to check and ensure the clarity and applicability of the tools in addition to calculate the duration required for filling in the questionnaires. Any necessary modification will be made and to identify obstacles and problems that may be encountered during data collection, participants in the pilot study is not included in the research.
Field of the work: Once official permission is obtained by using the proper channel of communication from the director of Hafr Al-Batin Central Hospital and Maternity and Children's Hospital – Hafr Al Batin, Saudi Arabia, the questionnaire sheet uploaded on Google drive in the form of hyper-Link and sent to the directors to distribute it to the nurses at the previously selected settings. Data collected and cleaned regularly in usual basis by checking the link format and allow for easy accessibility to every nurses at their spare time according to shift workload. This study carried out over a period according to a time plan. The time needed for each filling the questionnaire sheet ranged from 15-20 minutes according to the response of the participant nurses. Another data collection method done by participation through focus groups discussion which can held during nursing in-service education days, which nurses are routinely rostered to attend. Nurses who did not wish to participate in a focus group could use the time to complete their annual mandatory online training or independent private study. Data collection will begin in Augest to the end of October 2024.
Statistical analysis: Data coded, entered, and analyzed using Statistical Package for Social Science (SPSS) version 23 or higher. The collected data subjected to statistical analysis by the use of suitable techniques to achieve the objectives of the study.
Results
Table (1): Regarding to percentage distribution of the studied critical care nurses according to their socio-demographic characteristics, the current study revealed that the age group ranged from 26- 31 years represent 36% while, the mean 31.81. In addition, the female participant represents 64% about 27% of them had married. Concerning to education qualifications the half of participant 52% had bachelor’s degree and 40 diploma, doctoral respectively. Also, years of experience, more than half of participants ranged from 6-10 years represent 65%. Moreover, 41% of participants had bedside nurse while 30% had clinical nurse specialist and staff nurse respectively. Furthermore, more than half 56% of participants worked in combined ICU-CCU.
Table (1): Percentage distribution of the studied critical care nurses according to their socio-demographic characteristics (n=100)
|
Variable |
N |
% |
|
Age |
||
|
20-25 Years |
14 |
14.0 |
|
26-31 Years |
36 |
36.0 |
|
32-36 Years |
27 |
27.0 |
|
≥37 Years |
23 |
23.0 |
|
Mean ± SD |
31.81±6.18 |
|
|
Gender |
||
|
Male |
36 |
36.0 |
|
Female |
64 |
64.0 |
|
Marital Status |
||
|
Single |
21 |
21.0 |
|
Married |
72 |
72.0 |
|
Divorced |
3 |
3.0 |
|
Widowed |
4 |
4.0 |
|
Educational qualifications |
||
|
Diploma |
40 |
40.0 |
|
Bachelor |
52 |
52.0 |
|
Master |
8 |
8.0 |
|
Doctoral |
40 |
40.0 |
|
Years of experience |
||
|
1-5 yrs. |
13 |
13.0 |
|
6-10 yrs. |
65 |
65.0 |
|
11 – 15 yrs. |
22 |
22.0 |
|
Job title/Current position |
||
|
Direct care/bedside nurse
|
41 |
41.0 |
|
Staff/charge nurse
|
29 |
29.0 |
|
Clinical nurse specialist
|
30 |
30.0 |
|
Type of the critical care unit |
||
|
Combined ICU-CCU |
56 |
56.0 |
|
MICU |
26 |
26.0 |
|
SICU |
6 |
6.0 |
|
Shock/trauma unit. |
12 |
12.0 |
Figure (1): Previous training program in care of patients End of life in intensive care unit (n=100) The current results of the findings in this study regarding attendance on the previous training program in care of patients end of life in intensive care unit shown that most studied nurses do not present.
Table (2): Current results shows that critical care nurses’ perceived barriers to end-of-life care, such as family does not understand what ‘lifesaving measures’ really means, the nurse has to deal with angry family members, Intrafamily fighting about whether to continue or stop life support, not enough time to provide quality end-of-life care because the nurse is consumed with activities that are trying to save the patient's life, continuing rigorous care for a patient with a bad prognosis due to legal concerns from family, and the nurse was aware of the patient's bad prognosis before informing the family were among the highest frequency score and intensity score. 3.14, 3.39, 3.20, 3.11, 3.01, 3.31 respectively.
Table 2: Critical care nurses’ perceived barriers to end-of-life care
|
Barriers |
Frequency score |
Intensity score |
PSBS |
||||
|
Mean |
SD |
Rank |
Mean |
SD |
Rank |
|
|
|
3.14 |
1.39 |
6 |
3.05 |
1.23 |
8 |
9.58 |
|
2.28 |
1.36 |
24 |
3.39 |
1.07 |
7 |
7.73 |
|
2.95 |
1.38 |
13 |
2.98 |
1.21 |
11 |
8.79 |
|
2.98 |
1.21 |
12 |
2.98 |
1.21 |
12 |
8.88 |
|
3.19 |
1.34 |
5 |
2.94 |
1.17 |
14 |
9.38 |
|
2.93 |
1.37 |
14 |
3.33 |
1.19 |
3 |
9.76 |
|
3.39 |
1.07 |
1 |
3.33 |
1.41 |
1 |
11.29 |
|
3.20 |
0.80 |
4 |
3.20 |
0.80 |
6 |
10.24 |
|
3.11 |
0.80 |
7 |
3.11 |
0.80 |
2 |
9.67 |
|
2.88 |
1.36 |
15 |
3.05 |
0.96 |
9 |
8.78 |
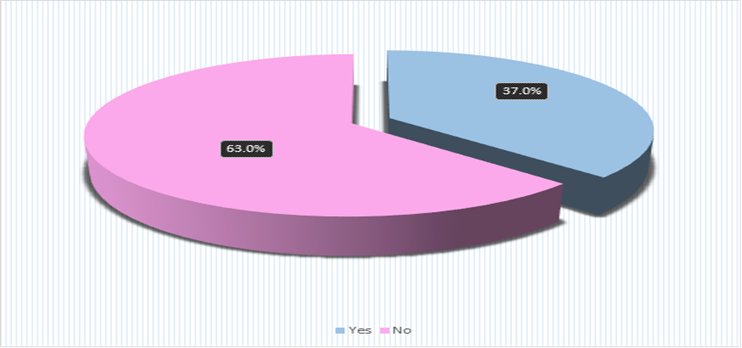
Figure 1
Figure 2
Figure 3
| |||||||