Pulmonary Nodule: A Rare Case of Diffuse Large B Cell Lymphoma
Pulmonary Nodule: A Rare Case of Diffuse Large B Cell Lymphoma
Walid Hadid MD*1, Shaheen Islam MD, MPH2, Rabih I Bechara MD3
1. Assistant Professor of Medicine, Division of Pulmonary, Critical Care and Sleep Medicine. University of Kentucky.
2. Professor of Medicine, Division Chief, Division of Pulmonary, Critical Care and Sleep Medicine, Augusta University.
3. Professor of Medicine, Director; Interventional Pulmonology Atrium Wake Baptist. Wake Forest School of Medicine.
*Correspondence to: Walid Hadid MD, Assistant Professor, Interventional Pulmonary Section of Pulmonary, critical Care and Sleep, University of Kentucky.
Copyright
© 2023 Walid Hadid MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2023
Published: 30 September 2023
Pulmonary Nodule: A Rare Case of Diffuse Large B Cell Lymphoma
Primary pulmonary lymphoma is defined as clonal lymphoproliferative disorder infiltrates of one or both lungs, without extrapulmonary involvement at the time or up to 3 months after the diagnosis (1). It is 0.5-1% (2) of primary pulmonary malignancy. 70-80 % of that is mucosa associated lymphoid tissue lymphoma (MALT) (2). Thus, all other types of lymphoma are about 20-30%. Diffuse large B-Cell lymphoma (DLBCL) is one of uncommon primary lung lymphoma. It is rare for DLBCL to present as pulmonary nodule without lymph node involvement.
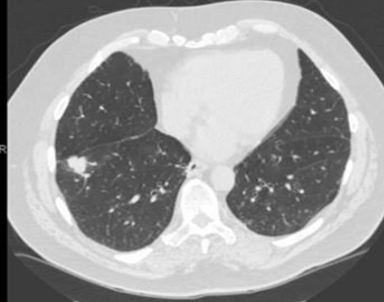
An 80-year-old man with past medical history of Hypertension and type-2 diabetes mellitus. He presented to his primary care physician for change of his urine color which he described as tea colored and he passed three very small stones. The primary care physician ordered a non-contrast CT abdomen with renal protocol to evaluate for renal calculus. The CT abdomen showed no renal calculus but it picked up a 23 mm right lower lobe pulmonary nodule (Figure1). The patient was referred to positron emission tomography scan (PET scan). The PET scan showed hypermetabolic activity in the right lower lobe nodule. the nodule had standardized uptake values (SUV) 10.7. This was highly suspicious for malignant etiology of the lung nodule. There was no other significant finding on the PET scan to suggest malignancy anywhere else but the lung nodule. There were no significant hypermetabolic activities of the mediastinal and hilar lymph node. The patient was referred to our interventional pulmonary clinic. The patient has chronic dry cough without hemoptysis. He denies any shortness of breath or dyspnea on exertion. He denies any history of smoking or significant history of occupational exposure. We discussed with the patient performing bronchoscopy and biopsy and he agreed on the procedure. A robotic bronchoscopy was performed and transbronchial lung needle aspiration TBNA with 21 gage needle and transbronchial lung biopsies with 2 mm forceps were obtained from the lung nodule. Endobronchial ultrasound with TBNA from mediastinal and hilar lymph nodes were obtained. All TBNS and biopsies were sent for cytology and pathology. Lung nodule pathology showed diffuse large B-Cell lymphoma (DLBCL). Lymph node TBNA showed normal lymphocytes. DLBCL was limited to the lung nodule only.
Primary lung lymphoma (PLL) it forma about 0.5% of all primary lung tumor (2). PLL is defined as clonal lymphoproliferative disorder infiltrates of one or both lungs, without extrapulmonary involvement at the time or up to 3 months after the diagnosis. The most common lymphoproliferative disorder of the lung is MALT lymphoma 70-80% (2). Less common is B-cell lymphoma such as DLBCL, lymphomatoid granulomatosis (LYG), plasmacytoma, and other types of small lymphocytic lymphoma in addition to T-cell origin lymphoma (2).
Primary pulmonary DLBCL is a rare disease which is more likely to present in immunocompromised and elderly patients (3). Up to 50% of primary pulmonary DLBCLs it may be presented at the same time with pulmonary marginal zone B cell lymphoma of mucosa associated lymphoid tissue (MALT)(3). Therefore, there is possibilities that MALT may progress to DLBCL (3). Almost 50% of Pulmonary MALT can be asymptomatic at the time of the diagnosis. There is no particular microorganism has been linked to the development of primary MALT lymphoma of the lungs. There is no guideline or randomized clinical trial on the treatment of Pulmonary DLBCL. Surgical option in localized disease has been used before (4). Radiation it can be used but in specific cases but it has no significant role (3). Chemotherapy with CHOP with or without Rituximab has shown survival benefits in nodal lymphoma (5,6) . The presentation of DLBCL as solitary pulmonary nodule as solo location is very rare. Establishing the diagnosis in this case is critical as treatment options are different from other types of lung cancer.
Part of this case was presented as poster in American Thoracic Society Conference( ATS 2022). San Francisco, USA.
Figure 1: Right lower lobe lung nodule.
References
1.Borie R, Wislez M, Antoine M, Cadranel J. Lymphoproliferative Disorders of the Lung. Respiration. 2017;94(2):157-175
2. Piña-Oviedo S, Weissferdt A, Kalhor N, Moran CA. Primary pulmonary lymphomas. Adv Anat Pathol. 2015;22(6):355–75.
3.Zhu Z, Wei Liu, Mamlouk O, O’Donnell JE et al. Primary Pulmonary Diffuse Large B Cell Non-Hodgkin’s Lymphoma: A Case Report and Literature Review. Am J Case Rep. 2017; 18: 286–290.
4.Vanden Eynden F, Fadel E, de Perrot M, et al. Role of surgery in the treatment of primary pulmonary B-cell lymphoma. Ann Thorac Surg. 2007;83(1):236–40
5.Aviles A, Nambo MJ, Huerta-Guzman J, et al. Rituximab in the treatment of diffuse large B-cell lymphoma primary of the lung. Hematology. 2013;18:81–84.
6.. Pfreundschuh M, Trümper L, Osterborg A, et al. CHOP-like chemotherapy plus rituximab versus CHOP like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: A randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7(5):379–91