Nasopharyngeal Swabs Gone Wrong: An Unexpected Complication of a Common Procedure
Nasopharyngeal Swabs Gone Wrong: An Unexpected Complication of a Common Procedure
Moyosoreoluwa M. Laditan MBBS 1,3* , Riya K. Kalra MBBS 1 , Laurene E. Reed MD 2 , Paras Khandhar MD 1
1.Department of Pediatrics Beaumont Hospital, Royal Oak, MI.
2.Department of Emergency Medicine Beaumont Hospital; Farmington Hills, MI.
3.Department of Internal Medicine Beaumont Hospital, Royal Oak, MI.
*Correspondence to:Dr. Moyosoreoluwa M Laditan, Beaumont Hospital, Royal Oak, MI. 3601 W 13 Mile Rd, Royal Oak, MI, 48073.
Copyright
© 2023: Dr. Moyosoreoluwa M Laditan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 September 2023
Published: 30 September 2023
Nasopharyngeal Swabs Gone Wrong: An Unexpected Complication of a Common Procedure
Introduction
During the COVID-19 pandemic, numerous swab samples have been taken for SARS-CoV-2 RT-PCR testing. About 8000 tests were done per day at the start of the pandemic. Despite adjacent vital structures, nasopharyngeal sampling is considered safe; however, adverse events can happen. We present a case of orbital cellulitis in a 4-year-old boy after multiple nasopharyngeal swab testing.
Case Report
A four-year-old, fully vaccinated male presented to the emergency room (ER) with four days of fever, a maximum temperature of 102°F, right eye pain, and swelling. Symptoms started after a recent acute viral upper respiratory illness. Due to worsening symptoms, his father gave him one dose of oral Amoxicillin and Clindamycin and then brought him to the ER. In the ER, right eye swelling was noted without painful or restricted eye movements. A complete eye evaluation by Ophthalmology was normal, including vision, pupils, accommodation, eye movements, tonometry, and fundus. Basic blood tests were unremarkable except for a high white blood cell count of 27.4 billion/L with neutrophilia and monocytosis, markedly elevated erythrocyte sedimentation rate (ESR) of 61 mm/hour and c-reactive protein (CRP) of 112.8 mg/L. He was diagnosed with periorbital cellulitis and started on intravenous Ampicillin-Sulbactam and Vancomycin in the ER before admission to the general pediatrics floor for further management. (Pictures 1-2).
He had traveled to Dubai 2 weeks before the onset of symptoms, before and after which he was swabbed on five separate occasions for COVID infection rule-out. There was no other pertinent medical or surgical history. Family history was negative for similar complaints, Methicillin resistant Staphylococcus aureus (MRSA) infections, and auto-immune diseases.
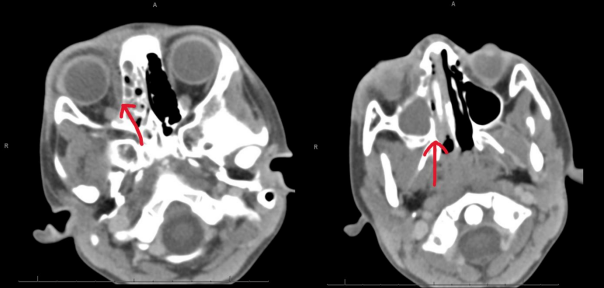
His eye swelling worsened throughout the first night of admission (Pictures 3-4). An orbital CT was obtained, which showed right orbital cellulitis with a subperiosteal abscess along the medial wall of the orbit, associated with vascular infection within the ethmoid air cells and the maxillary sinus (Pictures 5-6). Otorhinolaryngology (ENT) was consulted, who recommended endoscopic surgery in addition to starting Guaifenesin, Oxymetazoline, Fluticasone, and hypertonic saline nasal sprays. He was transferred into an intensive care step-down unit to monitor his ophthalmologic and neurologic status closely.
He underwent right total anterior and posterior ethmoidectomy, right maxillary antrostomy, and drainage of right subperiosteal abscess with endoscopic right orbital decompression the next day. Surgical culture returned positive for beta-lactamase positive Hemophilus Parainfluenza, Streptococcus Viridans group, coagulase-negative Staphylococcus species, and Streptococcus Intermedius. Infectious disease was consulted for antibiotic determination, who recommended continuing the same intravenous antibiotics until discharge and switching to Amoxicillin-Clavulanate after discharge for a 14-day course. In addition, he was also started on the nasal sprays (as above) twice a day until ENT follow-up. He was seen at the ophthalmology clinic three days after discharge, where his vision was normal, and swelling was significantly improved (Picture 7-8). He continued to follow up with ENT and ophthalmology outpatient, where he continued to improve.
Pictures 1 and 2
Pictures 3 and 4
Pictures 5 and 6
Pictures 7 and 8
Discussion
During the novel coronavirus infectious disease (COVID) pandemic of 2019, the nasopharyngeal (NP) swab became the centerpiece for detecting SARS-CoV2.1 About 8000 tests were done per day at the start of the pandemic2, and now there is clear upwards trend.
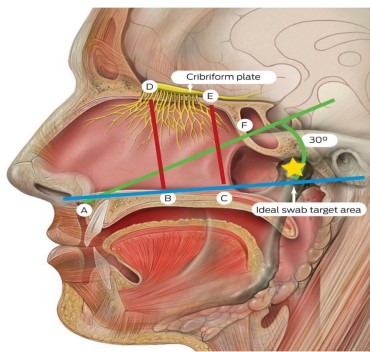
The trans-nasal approach to obtaining the respiratory tract secretions in the nasopharynx is the gold standard for COVID-19 testing; however, this examination can also be performed on the anterior nares and middle turbinate, but the sensitivity is significantly lower than that with NP swab.3 Nasopharyngeal sampling is considered safe, despite adjacent vital structures (orbit, skull base, rich vasculature, as in Picture 9); however, adverse events can happen.
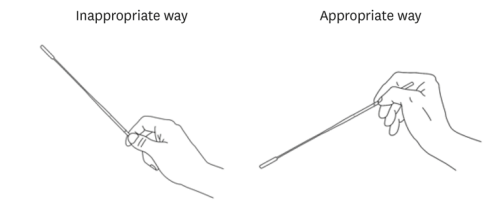
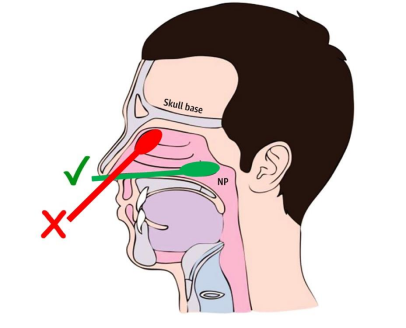
The procedure starts with correct head positioning by requesting the patient to gaze forward with the head on a horizontal plane parallel to the floor. It is ideal if the patient is comfortably seated with the back of their head against the headrest. Clinicians can predict the full depth of swab insertion by measuring the length between the nostril and the external ear canal. Hold the swab appropriately as in Picture 10 and insert it into the nostril 2-3 cm parallel to the nasal bridge until it reaches the anterior nasal spine, then raise the swab approximately 70° upwards at the same position and gently insert the swab along the nasal septum just above the nasal floor to the nasopharynx as in Picture 9 and 11. The swab should be kept on the nasopharynx for several seconds and gently pulled back while rotating it within fingers. In some studies, tilting the head slightly backward has been recommended at the beginning of the procedure for a more accessible nasal passage; however, a safe and effective approach is not significantly related to the head extension. Furthermore, head extension exposes the skull base to trauma if the clinician performs the procedure incorrectly.3,6
Picture 9
Picture 9:5 * A = anterior nasal spine; B = anterior nasal floor; C = posterior nasal floor; D = anterior cribriform plate; E = posterior cribriform plate; F = sphenoid ostium opening. The ideal swab target for the nasopharyngeal swab is indicated by the yellow star. Source: Lynch PJ, Jaffee CC. Head anatomy with olfactory nerve. https://commons.wikimedia.org/wiki/File:Head_olfactory_nerve.jpg (viewed January 2023). Creative Commons Attribution 2.5 (full terms at https://creativecommons.org/licenses/by/2.5/). Original image adapted by Sandeep Mistry.
{kind=link}
Picture 10:3 Clinicians should be cautious not to hold the swab inappropriately and are recommended to grip the swab appropriately. The inappropriate way of holding the swab causes difficulty entering the safety zone within 30° after passing the anterior nasal spine.
Picture 11:4 Picture showing correct way (?) and incorrect way (?) to collect a Nasopharyngeal (NP) sample to test for COVID-19
In an analysis of the MAUDE (Manufacturer and User Facility Device Experience) database and literature review by Hakimi et al. 8, the most common complication reported was a swab fracture resulting in a retained foreign body; it was followed by epistaxis, then headache. The most severe complication reported was cerebrospinal fluid (CSF) leak, of which one case led to meningitis. In another literature review by Clark et al. 9, epistaxis was reported as the most common complication, followed by a retained foreign body. In another study by Kim et al. 3, the retained foreign body was reported as the most common complication, followed by epistaxis, CSF leakage, and nasal septal/pharyngeal abscess. In a case report of a 35-year-old female by Fazekas et al. 10, preseptal cellulitis and infraorbital abscess were reported as a complication of nasopharyngeal swabs.
In our report, a 4-year-old male ultimately presented with orbital cellulitis and subperiosteal abscess after multiple nasopharyngeal swab testing leading to trauma to the intranasal structures potentiating bacterial pathogens to travel to the orbital area. Both preseptal and orbital cellulitis cause ocular pain and eyelid swelling, but only the latter causes swelling and inflammation of extraocular muscles and fatty tissues within the orbit, leading to painful extraocular movements, proptosis, and sometimes ophthalmoplegia with diplopia. A subperiosteal abscess can occur concurrently with orbital cellulitis, as in our case. The most common cause of orbital cellulitis has been reported as rhinosinusitis (86-98% of patients)11; however, infection and trauma of other adjacent structures can be additional causes.
Microbiology in preseptal and orbital cellulitis relates to the site of primary infection. Infections from the sinuses or the nasopharynx are usually caused by S. Pneumoniae, Moraxella Catarrhalis, and H. Influenzae. In contrast, infections due to local skin or skin structure infection (impetigo, cellulitis, or hordeolum) or dacryocystitis are usually caused by Staphylococcus aureus and Streptococcus pyogenes.14 In a study done in China, the most common bacterial pathogens found in children aged 2 to 6 years with preseptal or orbital cellulitis were M. catarrhalis (76.6 %), S. pneumoniae (26.6 %), S. aureus (21.8 %), H. parainfluenzae (12.7 %), and H. influenzae (2.3 %).12 Another study looking at nasal and skin pathogens of healthy individuals aged 2-40 years (classified from Tanner stage 1 to 5) in the Washington DC area showed a greater diversity of bacteria; however, Streptococcus, Moraxella, Haemophilus, and Neisseria dominated the microbiomes of Tanner stage 1 individuals.13 This is similar to our patient who grew a few beta-lactamase positive Hemophilus parainfluenza, few Streptococcus viridians group, rare coagulase-negative Staphylococcus group species, and rare Streptococcus intermedius. Physicians caring for the patient suspect that the source of his sinus infection, and the seeding of the infection deeper into the face, is attributable to a misplaced nasopharyngeal swab(s).
In orbital cellulitis, the infection can extend to the orbital apex, causing visual loss (3-11% of patients), and intracranially, causing epidural, subdural, or brain abscesses, meningitis, cavernous sinus or dural sinus thromboses. It rarely leads to death (reported in 1-2% of patients).11 A timely diagnosis and intervention can halt the disease process and help prevent and reverse the consequences. Furthermore, the risk of nasopharyngeal testing complications can be reduced by a basic understanding of the nasal anatomy and stopping the procedure in case of pain or increased resistance. The operator and patient should have proper expectations that although the test is uncomfortable, it should not cause intense pain.7
Conclusion
If not treated promptly, orbital cellulitis can cause significant morbidity (such as blindness) and mortality in the pediatric population. Even simple testing, like nasopharyngeal swabbing, can lead to this dangerous complication if done incorrectly and repeatedly over a short period. Given the extensive use of nasopharyngeal swabs, pediatric clinicians should be mindful of this rare complication in pediatric patients. They should educate technicians about the correct method of swabbing and weigh the risks and benefits when ordering repeated swabs.
Reference
1.Hanson KE, Caliendo AM, Arias CA, Hayden MK, Englund JA, Lee MJ, Loeb M, Patel R, El Alayli A, Altayar O, Patel P, Falck-Ytter Y, Lavergne V, Morgan RL, Murad MH, Sultan S, Bhimraj A, Mustafa RA. Infectious Diseases Society of America Guidelines on the Diagnosis of COVID-19: Molecular Diagnostic Testing. Infectious Diseases Society of America 2020; Version 2.0.0. Available at https://www.idsociety.org/practice-guideline/covid-19-guideline-diagnostics/
2.https://www.cnn.com/2020/03/19/health/us-coronavirus-case-updates-thursday/index.html
3.J Korean Med Sci. 2022 Mar 21;37(11):e88 https://doi.org/10.3346/jkms.2022.37.e88 eISSN 1598-6357·pISSN 1011-8934
5.https://www.mja.com.au/journal/2021/214/10/covid-19-swab-related-skull-base-injury
6.https://www.nejm.org/doi/10.1056/NEJMvcm2010260
7.https://jim.bmj.com/content/69/8/1399#xref-ref-15-1
8.https://journals.sagepub.com/doi/full/10.1177/19458924211046725#body-ref-bibr1-19458924211046725
9.http1s://jim.bmj.com/content/69/8/1399#xref-ref-15-1
10.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8137238/#R2
12.Pan H, Cui B, Huang Y, Yang J, Ba-Thein W. Nasal carriage of common bacterial pathogens among healthy kindergarten children in Chaoshan region, southern China: a cross-sectional study. BMC Pediatr. 2016 Sep 30;16(1):161. doi: 10.1186/s12887-016-0703-x. PMID: 27741941; PMCID: PMC5064895.
13.Oh J, Conlan S, Polley EC, Segre JA, Kong HH. Shifts in human skin and nares microbiota of healthy children and adults. Genome Med. 2012 Oct 10;4(10):77. doi: 10.1186/gm378. PMID: 23050952; PMCID: PMC3580446.
14. C Gappy MD, S Archer, et al. Preseptal Cellulitis. UpToDate. Sept 2022. Accessible at https://www.uptodate.com/contents/preseptal-cellulitis?search=orbital%20cellulitis&source=search_result&selectedTitle=2~31&usage_type=default&display_rank=2#H83430763