A Rare Presentation of Wilms Tumor in 2yr Old Child
A Rare Presentation of Wilms Tumor in 2yr Old Child
Dr Vishnu Vardhan Juture*1, Dr Gorla Vishnu Priyanka 2, Dr Shashidhar. V. Karpurmath 3
*Correspondence to: Dr Vishnu Vardhan Juture, Medical oncology department Vydehi institute medical sciences and research Centre, 82 EPIP Area, Whitefield, Bangalore, 560066, Karnataka.
Copyright
© 2023 Dr Vishnu Vardhan Juture. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 September 2023
Published: 30 September 2023
Abstract
Wilms’ tumor originates predominantly in the renal tissue; in rare cases, it can also arise from extra- renal sites accounting for 0.5-1% of cases of Wilms’ tumor seen.1 The establishment of the diagnosis of extrarenal Wilms tumor (EWT) with radiological features and clinical features is difficult unless histological findings are present. As there are less than 100 cases reported in the literature, we would like to report this extra-renal retroperitoneal Wilms tumor and discuss staging management and prognosis.
A Rare Presentation of Wilms Tumor in 2yr Old Child
Introduction
Wilms’ tumor (Nephroblastoma), the most common abdominal malignancy of childhood, occurs primarily as a malignant renal tumor. Extrarenal Wilms’ tumor is rare with occasional reports from the Indian subcontinent. There have been reports of it arising from other extra renal sites, in about 0.5– 1% of all cases.[1] The various locations of extra renal Wilms’ tumor include the retroperitoneum, uterus, skin, and thorax.[2] EWT is thought to arise from mesonephric remnants the clinical course of EWT often lacks specificity but as histological characteristics of Wilms tumor and EWT are similar, they both are staged in similar ways and treated in the same lines of management.[3, 4, 5]
Case Report
A 1 Year 8-month-old boy presented with Complaints of a painful progressively increasing mass per abdomen, frequent crying, fever, and reduced appetite since 1 month On examination revealed a healthy-looking boy With No pallor, No icterus, no peripheral lymphadenopathy With Blood pressure of 100/70 of mm of hg On P/A: mass measuring 10x 12cm in infra umbilical area, firm-hard in consistency does not move with respiration no hepatosplenomegaly considering his age and presentation we have thought Neuroblastoma, Wilms tumor, Rhabdomyosarcoma as differentials.
Hematological Parameters and serum biochemistry were within normal limits.
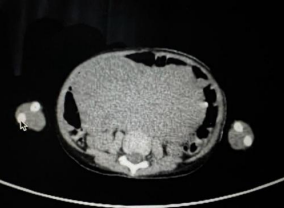
Figure 1, 2
On Imaging CECT abdomen suggestive of a Large soft tissue density heterogeneous mass lesion 127x8.3 x 11.1 in the central abdomen with lobulated margin and degeneration. No calcification is noted. As the origin of the mass and diagnosiscould not be made on imaging, a core needle biopsy was done from a mass lesion.
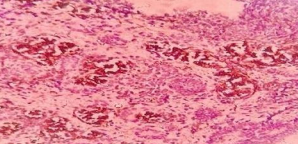
1) H&E 40X Reveals evidence of blastemal component <60%, immature tubular component, and cellular stroma.
Figure 3
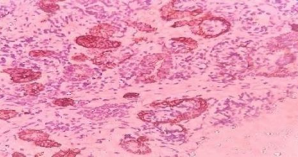
2) IHC Showed WT1- positive in the blastemal component and epithelial compnents from mesoblastic nephroma
Figure 4
3) PAN CK - positive in epithelial component
Figure 5
Vimentin - positive confirms mesenchymal origin.
Chromogranin, Synaptophysin, myogenic -negative, suggestive of ERWT.
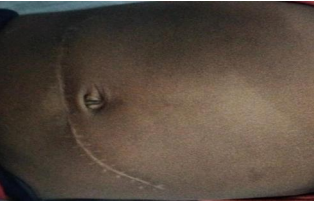
As per SIOP protocol patient was treated with Neoadjuvant chemotherapy followed by extraperitoneal surgical excision [6] of extrarenal Wilms tumor with Mesentery Node sampling done.
Figure 6
Histopathology suggestive of Nephroblastoma (Wilms tumor)-Mixed type, with 40% necrosis,Post-therapy histologic calcification: Intermediate risk (viable>33%, blastemal component <66%).no metastatic nodal deposits. TNM staging: p T2NO Mx (stage II).AV-2 PROTOCOL OF SIOP 2009 was started postoperatively based on the biopsy findings. The patient presently received 12th week of chemo and doing fine.
Discussion
As with intrarenal Wilms’ tumors in which most children present between 12 and 48 months with a mean age of diagnosis at 36 months, extrarenal Wilms’ tumors can similarly present within the same age group.[7] Our patient was a boy who presented at 2 years of age, which is the approximate mean age of diagnosis of most Wilms’ tumors.
Extrarenal Wilms tumors may be diagnosed in adults and neonates occasionally. But Extremes of Age groups have unfavorable prognosis.Extrarenal Wilms tumor’s exact embryonic origin is uncertain three theories are popularized. First theory[8] describes origin as ectopic mesonephric blastemal cells. The second theory[9] is the persistenceof primitive mesodermal tissue and the third theory[10] is the Connheims cell rest theory.
Apart from the classical presentation of painful abdominal swelling in this patient, he was otherwise ahealthy-looking baby.it is easy to confuse retroperitoneal extra-renal Wilms’ tumor with classical Wilms’ tumor based on clinical presentation alone because clinical features can be similar to both of them. However, extra renal Wilms’ tumor located in the inguinal canal, scrotum, and mediastinum children with abdominal mass should have immediate work-up for Wilms’ tumor. Regarding genetic associations unlike with standard Wilms’ tumor, only a few cases of extrarenal Wilms’ have been found to express the Wilms’ tumor suppressor gene WT1. [11] However in our case we have not done genetic testing. Another differential diagnosis considered was neuroblastoma, as it can also be seen inthe same age group as our patient. This condition often presents with pain from bony metastasis. [12] The possibility that other embryonal tumors, such as embryonal rhabdomyosarcoma, Burkett’s lymphoma, hepatoblastoma, and mixed Mullerian tumors can also occur in the retroperitoneum apartfrom retroperitoneal extra-renal Wilms’ should not be overlooked in the differential diagnosis of retroperitoneal tumors. staging of this patient directly goes to stage 2 due to its retroperitoneal presentation. Treatment strategies are similar for both renal Wilms tumor and extrarenal Wilms tumor but due to different locations and neighboring organs special scenarios are considered for surgery and adjoined therapies. The key step in the treatment of ERWT is surgical excision [6]
Most of the ERWTs will be having favorable histology but in about 11% of reported cases, local recurrence is observed. The recurrence rate is 15% in classical renal Wilms tumors in ERWTs 70% of cases are stage 2, 23% are stage 3 & 6% of cases are stage 4. In ERWT cases two- Year event-free survival [13] is 83% and the mortality rate was 5% compared to renal Wilms tumor.
Conclusion
Though there is difficulty in diagnosing Extrarenal Wilms tumor preoperatively, Extrarenal Wilms tumor should be considered when evaluating a patient with symptomatic abdominal swelling as diagnostic delay will cause a delay in appropriate treatment. Children presenting with abdominal mass one of the important differential diagnosis is extrarenalwilms tumour ,but staging treatment and prognosis are similar to wilms tumour.
Reference
1. Andrews PE, Kelalis PP, Haase GM. Extrarenal Wilms’ tumor: results of the National Wilms’ Tumor Study. J Pediatr Surg 1992;27:1181-84. https://ecommons.aku.edu/pakistan_fhs_mc_radiol/193
2. Shamberger RC, Grosfeld JL, Azmy AF. Renal tumours. In: Carachi R, Grosfeld JL, Azmy AF. The Surgery of Childhood Tumours. 2nd ed. Verlag Berlin Heidelberg: Springer; 2008. pp. 171-99. https://doi.org/10.1007/978-3-662-48590-3
3. Yunus M, Hashmi R, Hasan SH, Brohi HM. Extrarenal Wilms' Tumor. J Pak Med Assoc 2003;53: 436-9. https://ecommons.aku.edu/pakistan_fhs_mc_radiol/193
4. McAlpine J, Azodi M, O'Malley D, Kelly M, Golenewsky G, Martel M, et al . Extrarenal Wilms' tumor of the uterine corpus. Gynecol Oncol 2005;96:892-6.DOI: 10.5455/2349-3291.ijcp20150519
5. Hussain S, Nizami S, Tareen F. Neonatal extra-renal Wilm's tumour. J Pak Med Assoc 2004;54:37-8. http://www.njcponline.com on Monday, March 06, 2017, IP: 165.255.65.231]
6. Apozna?ski W, Sawicz-Birkowska K, Palczewski M, Szyde?ko T. Extrarenal nephroblastoma. Cent European J Urol. 2015;68(2):153–6.doi :10.5173/ceju.2015.571
7. Tagge EP, Thomas PB, Othersen HB Jr. In: Wilms’ tumour. In: Grosfield JL, O’ Neill jr JA, Fonkalsrud EW, Coran AG. editors. Peadiatric Surgery. 6th ed. Philadelphia: Mosby Elsevier; 2006. p. 465-86. http://www.njcponline.com on Monday, March 06, 2017, IP: 165.255.65.231]
8. Broecker BH, Caldamone AA, McWilliams NB, Maurer H, Salzberg A. Primary Extrarenal Wilms' tumor in children. J Pediatr Surg 1989;24:1283 .10.5455/2349-3291.ijcp20150519
9. Fernandes ET, Kumar M, Doughlas EC, Wilimas J, Parham DM, Rao BN. Extrarenal Wilms' tumor. J Pediatr Surg 1989;24:483-5. 10.5455/2349-3291.ijcp20150519
10. Andrews PE, Kelalis PP, Haase GM. Extrarenal Wilm's tumor: Results of National Wilms' Tumor Study. J Pediatr Surg 1992;27:1181-4.https://ecommons.aku.edu/pakistan_fhs_mc_radiol/193
11. Roberts DJ, Haber D, Sklar J, Crum CP. Extrarenal Wilms’ tumors. A study of their relationship with classical renal Wilms’ tumor using expression of WT1 as a molecular marker. Lad invest 1993;68:528-36. 10.3390/cancers15092563
12. Stiller CA, Parkin DM. Human cancer: international variations in the incidence of neuroblastoma. Int J Cancer 2006;52: 538-43. Int. J. Cancer: 142, 1977-1985 (2018) © 2017 UICC
13. Rojas Y, Slater BJ, Braverman RM, Eldin KW, Thompson PA, Wesson DE, et al. Extrarenal Wilms tumor: a case report and review of the literature. J Pediatr Surg. 2013 Jun;48(6):E33–5. DOI : 10.5455/2349-3291.icp20150519