Evaluation of the Expression of Nanog in Invasive Breast Carcinoma at Tertiary Care Hospital
Evaluation of the Expression of Nanog in Invasive Breast Carcinoma at Tertiary Care Hospital
Dr.Hadiya Sibghatullah 1 , Dr.Hemkant Verma *2 , Dr.Riyasat Ahmed Memon1, Dr.Ikram Din Ujjan 1, Dr.Muhammad Rahil khan 1, Dr.Ghulam fatima 1, Dr Aditi 3
1. Department of Pathology
2. Department of Surgical Oncology
3. Department of Anaesthesia.
*Correspondence to: Dr Hemkant Verma, Consultant Surgical Oncology, IVY Hospital Mohali Punjab 140308.
Copyright
© 2023 Dr Hemkant Verma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 October 2023
Published: 28 October 2023
Abstract
Background
Breast cancer is the most prevalent cancer in women and the leading cause of cancer-related mortality in females, according to the majority of cases that are diagnosed. The histological type, grade, tumor size, lymph node status, estrogen and progesterone receptor status, and epidermal growth factor receptor 2 (HER-2/neu) status all affect the prognosis and progress of breast cancer. Because HER-2/neu is a proto-oncogene linked to a worse clinical result whereas HER-2/positive is directly linked to a good prognosis, it is treated with hormone therapy.
Objectives
This study was designed to determine Nanog expression in different types of malignant breast carcinomas. And to evaluate the immunohistochemical expression score of Nanog.
Material and Methods
It was a cross-sectional, descriptive study which was carried out in the department of pathology LUMHS Jamshoro between September 2020 and august 2022. Patients of histopathological diagnosed malignant breast neoplasms of which meet the inclusion criteria were taken into consideration. Sample size of study was 329 and a non-probability convenient sampling technique was used for sample selection. Histologic slides were inspected for confirmation of diagnosis. Immunohistochemistry of Nanog was applied and its expressions were interrupted. SPSS V.23 was used for data analysis The Chi-Square test was applied to associate the significance ((P ≤ 0.05).
Results
In this study involving 329 breast cancer patients, the expression of the stemness gene Nanog was investigated in relation to various clinicopathological factors. The findings revealed a significant association between Nanog expression and age, tumor size, lymph node involvement, estrogen receptor (ER) status, and progesterone receptor (PR) status (p < 0.05). Specifically, the 20-40 age group exhibited higher Nanog expression, along with smaller tumor sizes (<2cm) and absence of lymph node involvement. ER-positive and PR-positive cases also showed elevated Nanog expression.
However, no significant correlation was observed between Nanog expression and histological type of tumor, histological grade, HER2 status, molecular subtypes (Luminal A, Luminal B, Her-2neu, Triple negative), or lymphovascular invasion (p > 0.05). These results suggest that Nanog may serve as a potential biomarker for specific clinical characteristics in breast cancer patients, contributing to our understanding of disease progression and treatment implications.
Conclusion
This study revealed a significant prevalence of Nanog expression in breast cancer cases, indicating its common presence. The varying intensity and proportion of positive cells observed across different grades suggest that Nanog staining may offer insights into tumor aggressiveness. Although no significant correlations were found with specific variables, Nanog's potential as a diagnostic, prognostic, and predictive marker in breast cancer warrants further investigation.
Keywords: Nanog, Breast cancer ,Infiltrating ductal carcinoma, Immunohistochemical stain, TNBC, ER, PR, HER2.
Evaluation of the Expression of Nanog in Invasive Breast Carcinoma at Tertiary Care Hospital
Introduction
The most frequent cancer in women is breast cancer. There have been over 2.1 million new diagnoses recorded globally. representing roughly one in four cancer cases in women [1,2]. In Pakistan, it occurs more often than in Western and other Asian countries. According to recent research, the prevalence of breast cancer in women varied from 20 to 50%, with a total prevalence of 31% and an unusually high level of heterogeneity with a value of I 2 of 99.8% [3]. Higher prevalence of exogenous hormone intake, oral contraceptive use, hormone replacement therapy, nutrition (alcohol intake), anthropometry (greater weight, weight gain during adulthood, and body fat distribution), menstruation (early menarche, later menopause), reproduction (nulliparity, late age at first birth, and fewer children), physical inactivity, low socioeconomic status, and lack of awareness regarding the disease
The histologic type and grade, tumor size, lymph node status, estrogen receptor (ER), progesterone receptor (PR), and epidermal growth factor receptor 2 (HER-2/neu) status all affect the prognosis and treatment of breast cancer. While HER-2/neu is a proto-oncogene linked to a poorer clinical outcome and treated with trastuzumab, positive hormone-responsive malignancies are more likely to have a better prognosis and respond better to hormonal treatment. [21] The majority of patients still experience cancer recurrence and medication resistance despite ongoing advancements in therapeutic setup. Recent research indicates that the development, progression, metastasis, and recurrence of many kinds of tumors are all significantly influenced by cancer stem cells (C-SCs). A cell inside a tumor that has the ability to self-renew and develop into malignant cells is known as a C-SC. In order to overcome CSCs' resistance to chemo-radiation therapy in the future, it is imperative to create innovative therapeutic techniques [4,5, 6, 7, 8, 18].
The similarities between CSCs and embryonic stem cells (ESC) suggest a shared mechanism for the emergence of cancer [9, 10]. Early embryo self-renewal reactivation may be caused by a deregulated proliferation molecular pathway [11]. For the maintenance of ESC pluripotency, Nanog is a crucial multidomain homeobox transcription factor [13, 14]. The human Nanog gene, which can be found on chromosomal region 12p13.31, produces a 305-amino acid protein that is localized to the nucleus and has a conserved homeodomain motif. [15] It is well known that Nanog maintains pluripotent stem cells in their undifferentiated form. [16] The essential protein Nanog controls the production of this pluripotent marker by binding to the Rex-1 promoter. Rex-1 expression is decreased in ESCs when Nanog is knocked down, but it is increased when the protein is driven into expression. [17] Cancer stem cells' long-term self-renewal, multipotency, and quiescence are supported by Nanog.
It has been suggested that Nanog overexpression is connected to breast cancer patients' resistance to hormone or anticancer treatment. Transtuzumab also has an adverse association with the expression of ER/PR and Her2 receptors. Nanog has a function in carcinogenesis and influences tamoxifen resistance. [19]
Nanog-mediated reprogramming is hampered by Zmym2. Consistent outcomes across a variety of reprogramming systems, including epiSCs, fibroblasts, and brain stem cells, employing gain and loss of function experiments This supports findings from other research groups on RNAi in human cell reprogramming (22). Consequently, ZMYM2 may have a comparable function in the regulation of NANOG in humans [20].
Reprogramming can induce somatic cells to revert to a pluripotent state, enabling self-renewal and differentiation into adult organism germ layer cell types. NANOG's overexpression, triggered by factors such as retinoic acid or removal of leukemia inhibitory factor, inhibits embryonic stem cell development, causing rapid differentiation [24]. Its critical role in embryonic stem cells underscores its significance for self-regeneration [25]. In a majority of cases, NANOG is exclusively expressed in early embryonic and germline stem cells, contrasting with the predominant expression of OCT4 in pluripotent cells like epiblasts and germline stem cells [26,27]. Abundant NANOG and OCT4 expression has been noted in various cancers, including breast cancer [28], where their simultaneous suppression was found to reverse epithelial-mesenchymal transition (EMT) and impede lung adenocarcinoma cell dissemination [21]. NANOG's role in oncogenesis is evident through its involvement in the deregulation of factors like FoxJ1 and E-cadherin, influencing cell migration and invasion, as observed in ovarian cancer [29]. Investigations into NANOG's mechanism of action have unveiled its interactome and provided deeper insights into its function within the pluripotency family [30]
Material and Methods
This study was conducted over 2 years at the Department of Pathology, Liaquat University of Medical & Health Science Jamshoro, and LUMHS Diagnostic & Research Lab Hyderabad. It followed a cross-sectional descriptive design with a sample size of n=329 determined using open epi software calculator, considering a reference prevalence of 31% for Invasive Ductal Carcinoma in Pakistan, a 95% confidence interval, and a 5% margin of error. Purposive sampling, a non-probability conventional technique, was employed. Patients diagnosed with invasive ductal carcinoma after breast surgery were included, excluding those who underwent neoadjuvant treatment. Data collection involved obtaining demographic information with informed and written consent from patients or next of kin, aligning with the established inclusion criteria. Exclusion criteria ensured the integrity of the study's findings, excluding cases with certain biopsy specimen characteristics. Ethical approval was obtained from the review committee.
Procedure
The process of histopathological examination involved meticulous steps. Patient details, including name, age, and registration number, were cross-referenced with biopsy forms. Biopsy numbers and codes were matched with specimen containers. The forms were carefully reviewed to gather medical history, clinical, radiological, and intraoperative findings, along with the surgeon's provisional diagnosis.
Specimens, primarily total Breast Mastectomy cases, were grossly examined following established protocols. Size, shape, color, consistency, and integrity were noted. Upon cutting, sections were taken for cassettes, and the cut surface was described. Fixation involved 24 hours in formalin, with additional fixation for poorly fixed or fragile surfaces.
Tissue processing achieved uniform consistency for cutting via clearing, dehydrating, and embedding. An automated tissue processor was used for processing, followed by embedding in paraffin blocks. Subsequent sectioning using a manual microtome yielded thin paraffin sections, which were floated on water, dried, and placed on glass slides.
For morphological diagnosis, Hematoxylin and Eosin (H&E) staining was conducted. Steps included dewaxing, hydration, staining with Hematoxylin and Eosin, bluing, eosin staining, dehydration, and clearing. The process culminated in mounting with DPX, enabling comprehensive tissue evaluation.
Diagnosis
H&E stained slides were viewed under microscope starting from low magnification as 4x or 10x and to get an overview of the tissue sample and identify areas of interest. Then, move to higher magnification (e.g., 20x, 40x, or 100x) to assess cellular details as type of breast carcinoma as per WHO criteria. Histologic grading and staging were done for more accurate diagnosis and representative areas were marked for immunohistochemistry.
Immuno-Histochemistry
It is a specialized technique which selectively detect antigens present in tissue cells by manipulating the principle that antibodies directly bind to antigens in biological tissues. In this study Anti Nanog Antibody Rabbit monoclonal (EPR2027) has been used.
All of these cases were performed with a negative and positive control on the sample size of 329 cases with 5 cases per batch, these batches were formed for the stratification and simplification of the study. Positive control kit for Nanog was human Seminoma tissue labeling Nanog with purified ab109250 at 1/100. Our negative control was the tissue that the primary antibody did not shed. The nuclear staining was observed and scored. The controls guaranteed that the procedure of IHC is optimized and results are effective on the test tissue. The IHC procedure comprised several steps. Tissue positioning on DAKO IHC MICROSCOPIC slides, obtained through microtome cutting. A secondary antibody, Ab97051, was applied (1/200). Tissue underwent dewaxing, followed by antigen retrieval using a high pH Envision FLEX Target Retrieval Solution (pH 9.0). After cooling, slides were washed using DAKO ENVISON FLEX washing buffer pH7.6 (20x). Subsequently, peroxidase blocking with DAKO Envision FLEX solution, primary antibody application (Anti-Nanog antibody), and secondary antibody (Envision FLEX horseradish peroxidase) were carried out. Chromogen (DAB) application, counterstaining with hematoxylin, and mounting with DPX and a DAKO cover glass concluded the process.
The expression of Nanog was interpreted by nuclear staining in neoplastic cells. This is further scored for intensity and proportion. This interpretation was done by two pathologists at different times to ensure uniformity in results and to remove any bias.
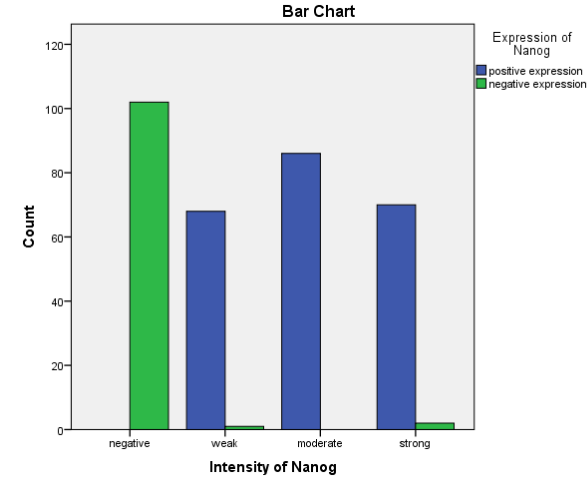
The Nanog expression status will be assessed using the Allred scoring method, which incorporates both the proportion of positive cells and staining intensity. Staining intensity will be categorized as follows: 0 for Negative, 1 for Weak, 2 for Moderate, and 3 for Strong. Meanwhile, the proportion of positive cells will be evaluated on a scale of 0 to 4, with 0 representing Negative staining, 1 indicating <25% Positivity in neoplastic cells, 2 reflecting >25-<50% Positivity, 3 denoting >50-<75% Positivity, and 4 representing >75% Positivity in neoplastic cells. This comprehensive approach will provide a nuanced understanding of the Nanog expression levels in each instance.
Total Score:
Finally, score of both intensity and proportion will be combined These two scores were multiplied to calculate the IRS, which ranged from 0–12 as follows: 0–3 as low expression or 4–12 as high expression. According to this method of assessment, staining scores ≤4 and ≥6 were regards as tumors with low and high expression, respectively.
Data Analysis
Statistical package for social sciences for windows (SPSS) V: 26.0 was used for data analysis. Qualitative tests were carried out to determine the frequency of Histological group and type, specimen type, specimen integrity, tumor grade, stage and positive or negative expressions of Nanog. They were expressed as number and percentage (No & %). The mean and standard deviation (X ± SD) of quantitative data (age) were used. The Chi square test was applied to determine the association of expression of Nanog with grade and stage. p value equals 0.05 was considered significant.
Results
Table 1 (Figure 2)
Figure 1
In this study we observed there is a statistically significant association between Nanog expression and patients in the age group 20 to 40 (p < 0.05).Nanog expression does not show a statistically significant association with patients in the age groups 41 to 60 and 61 to 80 (p > 0.05).Nanog expression is not statistically significantly associated with different histological types of tumors, including invasive ductal carcinoma, invasive lobular carcinoma, metaplastic carcinoma, and mucinous carcinoma (all p > 0.05).
Nanog expression does not exhibit a statistically significant association with various histological grades of tumors, including grade 1, grade 2, grade 3, and poorly differentiated carcinoma (all p > 0.05).
There is a statistically significant association between Nanog expression and tumor size less than 2cm (p < 0.05). Nanog expression does not show a statistically significant association with tumor sizes of 2 to 5 cm and greater than 5 cm (both p > 0.05).
Nanog expression is statistically significantly associated with lymph node involvement in stages pNX and pN0 (p < 0.05).No statistically significant association is observed between Nanog expression and lymph node involvement in stages pN1a, pN2a, and pN3a (all p > 0.05).
There is a statistically significant association between Nanog expression and positive ER status (p < 0.05).Nanog expression does not exhibit a statistically significant association with negative ER status (p > 0.05).There is a statistically significant association between Nanog expression and positive PR status (p < 0.05).Nanog expression does not show a statistically significant association with negative PR status (p > 0.05).Nanog expression is not statistically significantly associated with positive or negative Her2neu status (both p > 0.05).Nanog expression does not exhibit a statistically significant association with different molecular subtypes, including Luminal A, Luminal B, Her-2neu, and Triple Negative (all p > 0.05).Nanog expression does not show a statistically significant association with the presence or absence of lymphovascular invasion (both p > 0.05).
Discussion
The study calculated the mean age of breast cancer patients to be around 42.45 years, with a notable prevalence of cases in the 20-40 years age group (43.0%). This aligns with the findings of Al-Thoubaity et al. [31] who reported a higher prevalence of cases in individuals under 50 (59%). However, other studies like Rechsteiner et al. [32] indicated a higher mean age of diagnosis (61.3 years), while Han et al. [33] reported a mean age of 60.99 years. Couture et al. [34] observed a higher prevalence of cases in individuals over 50 (70.4%). study identified Luminal B subtype as the most prevalent (36.1%). This finding contradicts Couture et al. [34] where Luminal A was predominant (46.1%), while Han et al. [33] reported Luminal A as the most prevalent (70.7%). Al-Thoubaity et al. [31] did not specify subtype prevalence.
Invasive ductal carcinoma was the most common histological tumor type (95.5%), followed by lobular carcinoma (2.7%), metaplastic carcinoma (1.5%), and mucinous carcinoma (0.3%). Al-Thoubaity et al. [31] reported a slightly lower prevalence of invasive ductal carcinoma (85%) and higher prevalence of invasive lobular carcinoma (11.4%). Couture et al. [34] did not mention specific histological types. Histological grade 2 tumors were found to be more prevalent (49.4%), similar to Han et al. [33] with a prevalence of 42.2%. Al-Thoubaity et al. [31] reported grade 1 at 37.1%, grade 2 at 32.5%, and grade 3 at 29.4%. The discrepancy in grade distribution across studies suggests potential regional or demographic variations. The protein expression of NANOG was predominantly observed in the nucleus of breast cancer cells, with a lesser presence in the cytoplasm. Notably, NANOG expression was higher in tumor tissues compared to matched normal tissues. This elevated expression correlated strongly with advanced disease progression, lymph node metastases, lack of differentiation, and shorter overall survival times [35] This study showed the prevalent expression of Nanog in 224 cases of breast cancer while Nagata et al expressed only in a small percentage of breast cancer 29 cases. Our study and Nagata et al. [35], indicate a significant correlation between age categories and NANOG expression. our study and Nagata et al. [35], both show no significant correlation between NANOG expression and histological type of tumor. While our study finds a significant correlation between Size of Tumor and ER/PR Status, N stage and NANOG expression, and Nagata et al[35], does not provide specific information about this relationship. Emadian et al. [37] observing it in 55.8% of tumor samples, similar to our findings. Likewise, Finicelli et al. [39] reported Nanog expression in 44.5% of breast cancer patients. In contrast, Ezeh et al. [36] found no expression, and Nagata et al. [35] noted minimal expression (9.8%).
Our study and Emadian et al. [37], found significant correlation between age group "20 to 40" has a higher frequency of positive Nanog expression, tumors with a size less than 2cm (" <2cm"), Both sources indicate that cases with no lymph node involvement ("pNX, pN0") have a higher frequency of positive Nanog expression.
Our results display a distribution of Nanog expression across different molecular subtypes: Luminal A, Luminal B, Her-2neu, and Triple Negative. The Emadian et al[37],study does not directly show molecular subtype data for Nanog expression, making a direct comparison challenging. our results suggest no significant association between lymphovascular invasion and Nanog expression. while Emadian et al. [37], study also reports no significant difference in Nanog expression related to lymphovascular invasion.
Although Nanog expression was reported in 44.5% of breast cancer patients by Finicelli et al. [39], neither they nor Jin et al. [40] discovered an age-related trend. However, a strong correlation between Nanog expression and higher tumor grades (grade 2 and grade 3) was noted by our study and echoed by Emadian et al. [37], Finicelli et al. [39], and Wang et al. [38]. This suggests Nanogs potential linkage to aggressive disease states and tumor differentiation status.
Importantly, the consensus among all studies, including ours, underlines the significant potential of Nanog as a biomarker beyond traditional clinicopathological variables. Nanog's implications span disease aggressiveness, prognosis, and even potential therapeutic applications. The need for further research to validate Nanog's role and therapeutic potential is acknowledged by all, emphasizing the ongoing importance of understanding Nanog's impact on breast cancer [35,36,37,38,39,40].
Collectively, these findings contribute to the mounting evidence that Nanog holds significance as a biomarker for breast cancer aggressiveness, hormone resistance, and prognosis, extending beyond conventional clinical parameters. However, further research is imperative to establish its precise role and therapeutic utility in breast cancer [35,36,37,38,39,40].
Conclusion:
In this study, we delved into the expression of Nanog and its relationship with various clinicopathological parameters in patients with cancer. Our analysis aimed to decipher the significance of Nanog expression across different demographic and tumor-related factors.
Our findings revealed intriguing insights into the association between Nanog expression and several clinicopathological parameters. Notably, Nanog expression demonstrated a statistically significant correlation with certain parameters while maintaining its neutrality with others.
The age of the patient emerged as a discriminating factor, with a statistically significant link observed between Nanog expression and patients aged 20 to 40. However, this significance diminished for patients in the age groups of 41 to 60 and 61 to 80. This intriguing trend suggests that Nanog expression might have a more pronounced impact on younger patients, warranting further investigation.
Intriguingly, the size of the tumor also emerged as a significant factor. Nanog expression exhibited a substantial association with tumors smaller than 2cm, hinting at its potential role as an early indicator of tumor development. Conversely, Nanog expression did not display any significant ties with tumors ranging from 2 to 5 cm or larger than 5 cm.
Lymph node involvement, a crucial aspect of cancer progression, demonstrated a clear relationship with Nanog expression. A significant correlation was evident between Nanog and lymph node stages pNX and pN0, suggesting its possible involvement in tumor metastasis.
The status of estrogen receptors (ER) and progesterone receptors (PR) exhibited separate dynamics in relation to Nanog expression. Statistically significant associations were identified between Nanog expression and positive ER and PR statuses. This observation suggests that Nanog might be entwined with hormonal signaling pathways. Contrastingly, certain parameters such as histological type, histological grade, Her2neu status, molecular subtypes, and lymphovascular invasion did not exhibit any statistically significant correlation with Nanog expression. These findings prompt us to explore the intricate mechanisms behind these relationships and decipher the underlying molecular interactions. our study offers valuable insights into the intricate interplay between Nanog expression and clinicopathological parameters in cancer patients. This research underscores the potential of Nanog as a prognostic and diagnostic biomarker, especially in relation to patient age, tumor size, lymph node involvement, and hormone receptor status. However, the non-significant associations emphasize the need for comprehensive investigations to unravel the complex role of Nanog in cancer progression. This study forms a stepping stone for future research endeavors that delve deeper into Nanog's molecular intricacies and its promising implications for cancer management.
Strenghts Of Study
Large Sample Size: Inclusion of a substantial number of patients enhances statistical power and generalizability.
Robust Statistical Analysis: Utilization of appropriate tests like chi-square enhances reliability of findings.
Comprehensive Data Collection: Collection of diverse breast cancer-related factors provides a comprehensive examination.
Representative Tumor Characteristics: Inclusion of varied histological types, grades, and sizes improves external validity.
Multifactorial Assessment: Evaluation of Nanog expression across multiple factors contributes to a holistic understanding of its role in breast cancer.
Limitations Of Study
Despite assessing different clinicopathological features with the expression of Nanog, in this study, the prognosis of these patients could not be determined. Due to limited time duration, the follow up of all the patients with normal and aberrant Nanog expression could not be done. A longer follow-up period would allow for a more comprehensive assessment of outcomes, including recurrence rates, survival rates, and treatment responses.
Limited diversity as specific demographics or geographic regions, leading to limited diversity in the patient population. This can impact the external validity of the study results and limit their applicability to a more diverse population.
Future Recommendations
Conduct longitudinal studies to investigate Nanog expression's long-term impact on breast cancer outcomes, recurrence, and overall survival through follow-up assessments. Collaborate with multiple centers to expand sample size and enhance generalizability, assessing Nanog expression variations across diverse populations.
As well as conduct functional studies to uncover Nanog's molecular mechanisms impacting breast cancer progression, metastasis, and treatment response.
Study the link between Nanog expression and treatment response, examining potential resistance to therapies like hormonal treatment or targeted agents.
Lastly explore therapeutic strategies targeting Nanog, assessing effects of inhibition or silencing on tumor growth, metastasis, and treatment response in vitro and in vivo.
Reference:
1.Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R.L., Torre, L.A. and Jemal, A. (2018), Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J for Clin, 68: 394?424. doi: 10.3322/caac.21492.
2.Asif, Hafiz Muhammad, Sabira Sultana, Naveed Akhtar, Jalil Ur. Rehman, and Riaz Ur. Rehman. “Prevalence, Risk Factors and Disease Knowledge of Breast Cancer in Pakistan.” Asian Pacific Journal of Cancer Prevention 15, no. 11 (June 15, 2014): 4411–16. doi:10.7314/apjcp.2014.15.11.4411.
3.Idress, R., Fatima, S., Ghafar, J. A., Raheem, A., Ahmad, Z. (2018). Cancer prevalence in Pakistan: Meta-analysis of various published studies to determine variation in cancer figures resulting from marked population heterogeneity in different parts of the country. World Journal of Surgical Oncology, 16(1), 129-139.
4. Bao B, Ahmad A, Azmi AS, Ali S, Sarkar FH. Overview of cancer stem cells (CSCs) and mechanisms of their regulation:implications for cancer therapy. Current protocols in pharmacology. 2013;Unit 14.25(Chapter 14) .
5. Liu S, Wicha MS. Targeting breast cancer stem cells. Journal of clinical oncology. 2010;28(25):4006–4012.6. Clevers H. The cancer stem cell:premises, promises and challenges. Nature medicine. 2011;17(3):313–319.
7. Ratajczak MZ. Cancer stem cells-normal stem cells “Jedi” that went over to the “dark side” Folia histochemicacytobiologica. 2005;43(4):175–181.
8. Fábián A, Barok M, Vereb G, Szöllosi J. Die hard:are cancer stem cells the Bruce Willises of tumor biology? Cytometry A. 2009;75(1):67–74.
9. Dick JE. Stem cell concepts renew cancer research. Blood. 2008;112(13):4793–480.
10. Reya T, Morrison SJ, Clarke MF, Weissman IL. Stem cells, cancer, and cancer stem cells. Nature. 2001;414(6859):105–111.
11. Hart AH, Hartley L, Ibrahim M, Robb L. Identification, cloning and expression analysis of the pluripotency promoting Nanog genes in mouse and human. Developmental dynamics. 2004;230(1):187–98.
12. Guo ZK, Guo K, Luo H, Mu LM, Li Q, Chang YQ. The expression analysis of nanog in the developing rat myocardial tissues. Cellular Physiology and Biochemistry. 2015;35(3):866-74.
13. Liu A, Yu X, Liu S. Pluripotency transcription factors and cancer stem cells:small genes make a big difference. Chinese journal of cancer. 2013;32(9):483–487.
14. Guo Y, Liu S, Wang P, Zhao S, Wang F, Bing L, Zhang Y, Ling EA, Gao J, Hao A. Expression profile of embryonic stem cell-associated genes Oct4, Sox2 and Nanog in human gliomas. Histopathology. 2011;59(4):763–775.
15. Mitsui K, Tokuzawa Y, Itoh H, Segawa K, Murakami M, Takahashi K, Maruyama M, Maeda M, Yamanaka S. The homeoprotein Nanog is required for maintenance of pluripotency in mouse epiblast and ES cells. Cell. 2003;113(5):631–642.
16. Jeter CR, Yang T, Wang J, Chao HP, Tang DG. Concise review: NANOG in cancer stem cells and tumor development: an update and outstanding questions. Stem cells 2015; 33(8): 2381-2390.
17. Shi W, Wang H, Pan G, Geng Y, Guo Y, Pei D. Regulation of the pluripotency marker Rex-1 by Nanog and Sox2. Journal of biological chemistry 2006; 281(33): 23319-23325.
18. Islam F, Gopalan V, Smith RA and Lam AK: Translational potential of cancer stem cells: A review of the detection of cancer stem cells and their roles in cancer recurrence and cancer treatment. Exp Cell Res 335: 135-147, 2015.
19. Arif, K., Hussain, I., Rea, C., & El-Sheemy, M. (2015). The role of Nanog expression in tamoxifen-resistant breast cancer cells. OncoTargets and therapy, 8, 1327–1334. https://doi.org/10.2147/OTT.S67835.
20. Lawrence M, Theunissen TW, Lombard P et al. ZMYM2 inhibits NANOG-mediated reprogramming [version 1; peer review: 2 approved, 1 approved with reservations]. Wellcome Open Res 2019, 4:88 (https://doi.org/10.12688/wellcomeopenres.15250.1).
21. Safaee A, Zeighami B, Tabatabaee HR, MoghimiDehkordi B. Quality oflife and Related Factors in Breast Cancer Chemotherapy. Iranian Journal of Epidemiology. 2008;3(4):61–66.
22. “Global Cancer Observatory” International Agency for Research on Cancer, Lyon, France. [(accessed on 1 June 2020)]. Available online: https://gco.iarc.fr/
23. I. Ben-Porath, M.W. Thomson, V.J. Carey, R. Ge, G.W. Bell, A. Regev, R.A. Weinberg An embryonic stem cell-like gene expression signature in poorly differentiated aggressive human tumors Nat. Genet., 40 (2008), pp. 499-507.
24. Mitsui K, Tokuzawa Y, Itoh H, et al: The homeoprotein Nanog is required for maintenance of pluripotency in mouse epiblast and ES cells. Cell. 2003;113(5):631–642.
25. Nichols J, Zevnik B, Anastassiadis K, Niwa H, Klewe-Nebenius D, Chambers I et al. Formation of pluripotent stem cells in the mammalian embryo depends on the POU transcription factor Oct4. Cell 1998; 95: 379–391.
26. Pesce M, Gross MK, Scholer HR . In line with our ancestors: Oct-4 and the mammalian germ. Bioessays 1998; 20: 722–732.
27. Yeom YI, Fuhrmann G, Ovitt CE, Brehm A, Ohbo K, Gross M et al. Germline regulatory element of Oct-4 specific for the totipotent cycle of embryonal cells. Development 1996; 122: 881–894.
28. Almstrup K, Hoei-Hansen CE, Wirkner U, Blake J, Schwager C, Ansorge W et al. Embryonic stem cell-like features of testicular carcinoma in situ revealed by genome-wide gene expression profiling. Cancer Res 2004; 64: 4736–4743.
29. Siu MKY, Wong ESY, Kong DSH, Chan HY, Jiang L, Wong OGW et al. Stem cell transcription factor NANOG controls cell migration and invasion via dysregulation of E-cadherin and FoxJ1 and contributes to adverse clinical outcome in ovarian cancers. Oncogene 2013; 32: 3500–3509.
30. Wang J, Rao S, Chu J, et al. : A protein interaction network for pluripotency of embryonic stem cells. Nature. 2006;444(7117):364–368.
31.Al-Thoubaity, F. K. (2020). Molecular classification of breast cancer: A retrospective cohort study. Annals of medicine and surgery, 49, 44-48.
32. Rechsteiner, A., Dietrich, D., & Varga, Z. (2023). Prognostic relevance of mixed histological subtypes in invasive breast carcinoma: a retrospective analysis. Journal of Cancer Research and Clinical Oncology, 149(8), 4967-4978.
33. Han, Y., Wang, J., & Xu, B. (2020). Clinicopathological characteristics and prognosis of breast cancer with special histological types: a surveillance, epidemiology, and end results database analysis. The Breast, 54, 114-120.
34. Couture, H. D., Williams, L. A., Geradts, J., Nyante, S. J., Butler, E. N., Marron, J. S., ... & Niethammer, M. (2018). Image analysis with deep learning to predict breast cancer grade, ER status, histologic subtype, and intrinsic subtype. NPJ breast cancer, 4(1), 30.31..
35.Nagata T, Shimada Y, Sekine S, Moriyama M, Hashimoto I, Matsui K, et al. KLF4 and NANOG are prognostic biomarkers for triple-negative breast cancer. Breast Cancer 2016;24:326–35. https://doi.org/10.1007/s12282-016-0708-1.
36. Ezeh UI, Turek PJ, Reijo RA, Clark AT. Human embryonic stem cell genesOCT4, NANOG, STELLAR, andGDF3 are expressed in both seminoma and breast carcinoma. Cancer 2005;104:2255–65. https://doi.org/10.1002/cncr.21432.
37. Emadian Saravi O, Naghshvar F, Torabizadeh Z, Sheidaei S. Immunohistochemical Expression of Nanog and Its Relation with Clinicopathologic Characteristics in Breast Ductal Carcinoma. Iranian Biomedical Journal 2019;23:184–9. https://doi.org/10.29252/ibj.23.3.184.
38. Wang D, Lu P, Zhang H, Luo M, Zhang X, Wei X, et al. Oct-4 and Nanog promote the epithelial-mesenchymal transition of breast cancer stem cells and are associated with poor prognosis in breast cancer patients. Oncotarget 2014;5:10803–15. https://doi.org/10.18632/oncotarget.2506.
39. Finicelli M, Benedetti G, Squillaro T, Pistilli B, Marcellusi A, Mariani P, Santinelli A, Latini L, Galderisi U, Giordano A. Expression of stemness genes in primary breast cancer tissues: the role of SOX2 as a prognostic marker for detection of early recurrence. Oncotarget 2014; 5(20): 9678-9688.
40. Wang B, Jin Y, Zhang X, Sun M, Zhang Y, Zhang G. Clinical implications of the coexpression of SRC1 and NANOG in HER-2-overexpressing breast cancers. OncoTargets and Therapy 2016;Volume 9:5483–8. https://doi.org/10.2147/ott.s102386.