Acute Compartment Syndrome of the Forearm after Minor Trauma in a Patient with Antiphospholipid Syndrome on Anticoagulant Therapy
Acute Compartment Syndrome of the Forearm after Minor Trauma in a Patient with Antiphospholipid Syndrome on Anticoagulant Therapy
Mr Ahmed Elkohail 1, Mr Georgios A. Loumpardias 2, Mr Paulius Birgeris 3, Mr Diab *4, Miss Larisa Radu 5, Dr Ahmed Khalifa 6
*Correspondence to: Mr Diab.
Copyright
© 2023 Mr Diab. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 August 2023
Published: 01 November 2023
Abstract
Compartment syndrome of the forearm is a rare event that can be subsequent to trauma or other pathological and physical conditions. At the forearm the thin and elastic fascia may allow accumulation of blood more than in other districts, especially in patients undergoing anticoagulant therapy. We describe a rare case of an acute compartment syndrome of the forearm after minor trauma to Elbow without fracture or dislocation in a patient with LMWH SC injection therapy for Antiphospholipid Syndrome. Prompt diagnosis and surgical decompression helped to avoid the occurrence of complications with a satisfying recovery of forearm function.
Acute Compartment Syndrome of the Forearm after Minor Trauma in a Patient with Antiphospholipid Syndrome on Anticoagulant Therapy
Introduction
Compartment syndrome is a condition in which increased tissue pressure within a limited space compromises the circulation and function of the contents of that space. This happens when pressure is elevated over a certain level for some time sufficient to reduce capillary perfusion. The inadequate tissue perfusion then leads to inadequate tissue oxygenation to the nerves as well as muscles within the affected compartment.
Compartment syndrome was first described in 1881 by Richard von Volkmann, a German surgeon, who first described the Volkmann contracture in a publication called 'Non-infective ischaemic conditions of various fascial compartments in the extremities.' He believed at the time that the contracture was not due to nerve damage but rather to ischemia. The anatomy of the forearm is very complex. The ulna and the radius represent the bony structure. There are 3 compartments of muscles.
The three compartments are:
- The anterior compartment contains the hand and wrist flexors.
- The posterior compartment contains 9 muscles responsible for extension of the wrist and digits and supination of the forearm. It is separated from the anterior compartment by the interosseous membrane between the radius and ulna.
- The lateral compartment
The nerves that supply the forearm are the radial nerve, the median nerve, and the ulnar nerve, with their sensory and motor branches.
The vascular supply is provided by the radial artery and the ulnar artery and their anastomotic vessels.
Compartment syndrome of the forearm is primarily a clinical diagnosis. Patients often present within a few hours of the inciting event, sometimes even within 48 hours. They present with a swollen, tense, tender forearm with overlying skin that is often pink. Pain that is out of proportion to the injury is the pathognomonic sign, especially on passive stretching of the fingers. Pain is usually not relieved by rest, analgesia, or anti-inflammatory medication. Pain can, however, disappear in late stages or presentations or chronic compartment syndrome. A few patients who present a few hours after the onset of compartment syndrome present with haemorrhagic blisters in addition to the above mentioned.
Sensory deficits or paraesthesia are usually signs of nerve ischemia in the affected compartment and can be present. Paralysis is often a late sign.
Radial and ulnar pulses are usually intact, given the systolic arterial pressure (around 120 mmHg) usually exceeds the pressure within the involved compartment. The absence of pulses is usually a late finding, and amputations are considered when there is a significant amount of ischaemic tissue death.
Epidemiology
Compartment syndrome in the forearm is most commonly seen after trauma associated with fractures, crush injuries, head injuries, and burns. The National Trauma Data Bank (U.S.A.) reveals 1.22% of forearm fractures and 3.79% of tibial fracture patients underwent fasciotomy for compartment syndrome. Young patients with a mean age of 32 years in males and a mean of 44 years in females are likely to be affected, while the overall incidence of acute compartment syndromes is 3.1 per 100000 population per year in the western world. Incidence is increased in men compared to women with a ratio of 10 to 1.
Case Report
A 39-year-old right hand dominant woman with PMHx : Antiphospholipid Syndrome (2015 ) on Eonxaparin 100 mg OD , Compartment Syndrome Bilateral Lower Limbs (2015 –2016 ) , DVT Right Lower Limb (2016 ), Complex Region Pain , presented to the ED complaining of 1 week worsening Left forearm pain and swelling . Reported 1-week history of left elbow contusion after a fall at Home from stairs. At that time Radiographs of Left Elbow / Forearm /Hand performed at walking centre. No fracture /dislocation detected and Patient sent home with analgesia.
Laboratory values revealed increased levels of CRP: 10 (0-4 mg/L ) , CK: 3370 (25-150 U/L) , decreased levels of Hb: 87 (118-148 g/dL ) and normal range of APTT: 1.0 sec and INR of 1.0.
Radiographs did not show fractures or dislocations again.
Due to limitation of ROM and increasing pain of Left upper arm during movements despite Analgesia Patient admitted for monitor and in order to exclude muscular hematoma; urgent MRI requested and performed.
MRI Forearm Lt (non-contrast) report:
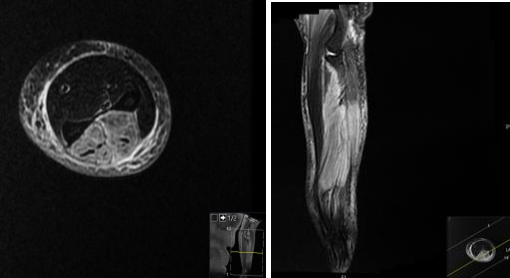
The muscles within the posterior compartment of the forearm, including the extensor muscles, are diffusely enlarged and demonstrate increased signal intensity on T2-weighted sequences with anterior bowing of the deep fascia. No obvious internal collections to suggest abscess formation.
Note is also made of extensive subcutaneous oedema. The oedema extends from the wrist to the elbow, involving the soft tissues and the muscles of the forearm. There is no evidence of any underlying bony or joint abnormalities.
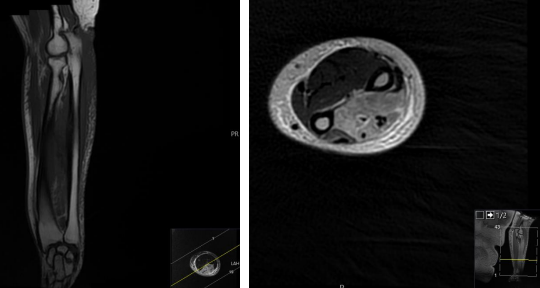
The flexor muscles within the anterior compartment of the forearm are within normal limits with no evidence of injury or oedema.
The tendons and ligaments are intact, with no evidence of tearing or avulsion.
Photo 1 : Axial STIR Left Forearm Photo 2 : Cor STIR Left Forearm
Photo 3: Cor T1 Left Forearm Photo 4: Axial T2 PR Left Forearm
Conclusion of MRI:
Diffuse thickening an oedema change involving the muscles of the posterior compartment and the subcutaneous oedema. Given the patient's history of antiphospholipid syndrome and recent trauma followed by severe pain, the MRI findings could be in keeping with suspected compartment syndrome, this needs urgent surgical review.
So, after MRI and worsening clinical presentation: Left forearm increased Swelling at dorsal side and sever pain with passive extension of fingers and wrist, urgent surgical treatment was planned with fasciotomy.
Operation:
Urgent left forearm fasciotomy performed via Thompsons approach to the forearm. Fascia opened and muscles appeared strained and compressed with pale pink colour. No bleeding, No necrotic muscle detected. Traced incision back to tendons and wound Covered with Gelonet, Blue gauze, wool and crepe.
Post-operative Plan:
Elevation, NVS close monitor, 48-72 hours 2nd look +/- closure, continue antibiotics and analgesia
After 48 hours second look of wound performed: Forearm wound looked healthy, no signs of soft tissue necrosis, muscles viable. Washout pulse lavage 3.0 litres normal saline. Skin closed with interrupted 2-0 Ethilon sutures without tension.
Two weeks after surgery wound looked healthy and sutures removed and dressing applied.
Four weeks after surgery had full recovery of elbow flexion and wrist and finger motion without Pain. Sensibility was normal with two-point discrimination test value less than 5 mm.
Discussion
ACS is an orthopaedic emergency that can occur in any fascial compartment within the body. Therefore, it is important to identify all risk factors that can be associated with ACS; early diagnosis and treatment are vital in preventing unfavourable outcomes such as permanent muscular and neurovascular damage, limb amputation, and death
Patients undergoing anticoagulant therapy raise their susceptibility to haemorrhage and are more exposed to development of an acute compartment syndrome.
To our knowledge, there are no published case studies of recurrent ACS of both upper and lower limbs in a patient with antiphospholipid syndrome.
The beauty of this case report is that this Patient with Hx of Antiphospholipid Syndrome and Recurrent episodes of CS in both Lower Limbs developed also Unicompartmental CS in Left Upper Limb after Minor Trauma which make this case unique .
Further research is needed to determine the incidence of ACS and it’s relation to antiphospholipid syndrome.
Conclusion
In patients with antiphospholipid syndrome /LMWH therapy, the risk of development of compartment syndrome should be always considered and prolonged clinical observation should be indicated in order to detect initial clinical symptoms. Early treatment with fasciotomy may prevent major complications and residual deficits.
Reference
1. Paolo Titolo,* Patrizia Milani, Bernardino Panero, Davide Ciclamini, Giulia Colzani, and Stefano Artiaco. 2014 Jan 6. doi: 10.1155/2014/980940. Acute Compartment Syndrome of the Arm after Minor Trauma in a Patient with Optimal Range of Oral Anticoagulant Therapy. [PubMed] [CrossRef] [Google Scholar]
2. T. Chandraprakasam and R. Ashok Kumar. Acute compartment syndrome of forearm and hand. 2011 May-Aug; 44(2): 212–218. doi: 10.4103/0970-0358.85342. [PubMed] [CrossRef] [Google Scholar]
3. Mazur M., Jabaly N., Ebraheim N. Acute compartment syndrome in patients on long-term anticoagulation therapy. Journal of Trauma and Critical Care . 2018;3(1):1–5. [Google Scholar]
4. Mubarak S. J., Owen C. A., Hargens A. R., Garetto L. P., Akeson W. H. Acute compartment syndromes. The Journal of Bone and Joint Surgery. American Volume . 1978;60(8):1091–1095. doi: 10.2106/00004623-197860080-00012. [PubMed] [CrossRef] [Google Scholar]
5. Matthew Mazur N. J., Ebraheim N. Acute compartment syndrome in patients on long-term anticoagulation therapy. Journal of Trauma and Critical Care . 2019;3(1) doi: 10.35841/2591-7358.3.1.1-5. [CrossRef] [Google Scholar]
6. McQueen M. M., Gaston P., Court-Brown C. M. Acute compartment syndrome. Journal of Bone and Joint Surgery. British Volume (London) . 2000;82(2):200–203. doi: 10.1302/0301-620X.82B2.9799. [PubMed] [CrossRef] [Google Scholar]
7. James A. Nemunaitis, corresponding author 1 Jason P. Den Haese, Jr., 2 Mark S. Buseck, 3 Shawn W. Storm, 1 Joshua A. Tuck, 1 and Anthony J. Ferretti 1.A Case of Recurrent Compartment Syndrome with Concomitant Use of Eliquis. 2022 Mar 7. doi: 10.1155/2022/1863538. [PubMed] [CrossRef] [Google Scholar]
8. Netter Atlas of Human Anatomy: A Systems Approach, 8th Edition
9. Miller's Review of Orthopaedics, 8th Edition
10. Williams Hematology, 10th Edition
11. Musculoskeletal MRI, 3rd Edition /Authors : Nancy M. Major & Mark W. Anderson
12. OrthoBullets.com.