COVID-19 Pandemic Affected on Global Tuberculosis Epidemic
COVID-19 Pandemic Affected on Global Tuberculosis Epidemic
Attapon Cheepsattayakorn1,3*, Ruangrong Cheepsattayakorn2, Porntep Siriwanarangsun3
1. 10th Zonal Tuberculosis and Chest Disease Center, Chiang Mai, Thailand.
2. Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
3. Faculty of Medicine, Western University, Pathumtani Province, Thailand.
Correspondence to: Attapon Cheepsattayakorn, 10th Zonal Tuberculosis and Chest Disease Center, 143 Sridornchai Road Changklan Muang Chiang Mai 50100 Thailand Tel : 66 53 140767 ; 66 53 276364 ; Fax : 66 53 140773 ; 66 53 273590 ; Email : Attapon1958@gmail.com
Copyright
© 2023 Attapon Cheepsattayakorn. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 November 2023
Published: 16 November 2023
COVID-19 Pandemic Affected on Global Tuberculosis Epidemic
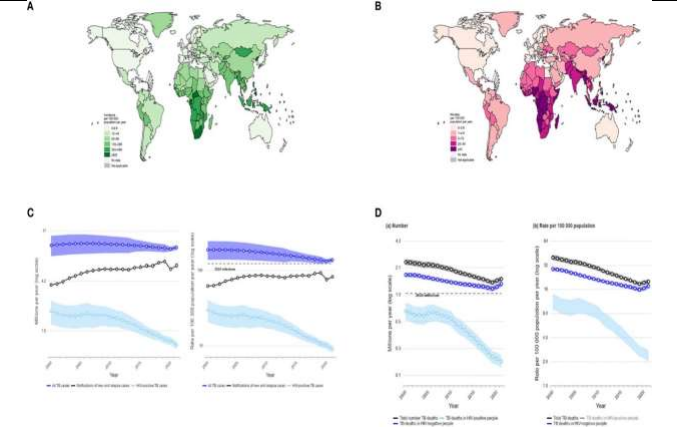
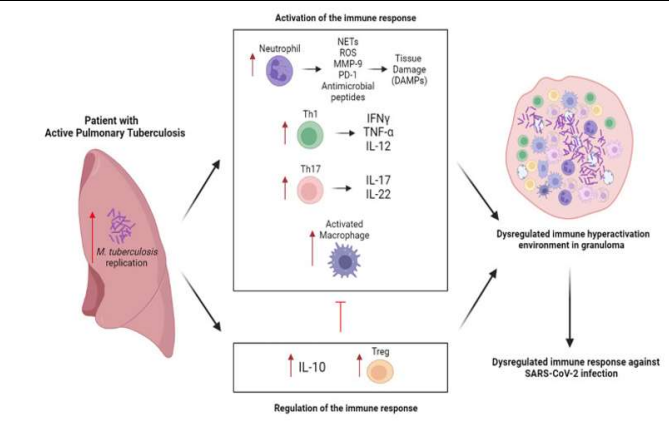
Between 2005 and 2019, globally, annual tuberculosis (TB, caused by Mycobacterium tuberculosis (M tuberculosis or M tb)) death (around 50 % of cases) decreased regularly and appeared 1.4 million of death in 2019 [1], whereas TB deaths were back to 1.5 million and 1.6 million in 2020 and 2021, respectively [1]. In 2020, global TB notification rate substantially dropped approximately 18 %, compared with 2019’s rate [1], whereas a partial recovery was noted in 2021 [1]. Characteristically, the disease affects the lungs with predominantly among adult men [1]. Geographically, the TB incidence and mortality is high in African and Asian countries (Figure 1A, 1B) [1]. In addition to the impact of global COVID-19 pandemic on global TB incidences and deaths, immunological responses in humans is also affected by COVID-19 and TB coinfection (Figure 2) [2]. Affection of immune responses in COVID-19 and TB (latent tuberculosis infection (LTBI)) coinfection was indicated in a previous systematic review of 4-cross-sectional studies that COVID-19- or SARS-CoV-2-antigen responsiveness, CD4-T-cells-specific-against SARS-CoV-2 or COVID-19, and lymphocyte counts reduced among patients with COVID-19 and active TB (Figure 2) [2]. Several recommendations focus on the following : 1) maintaining minimal TB surveillance, TB infection prevention and control, and TB health services, 2) leveraging laboratory capacity mechanisms of TB contact tracing, 3) incorporating digital health technologies, 4) considering routine-immunization- and latent-TB-infection-screening-catching-up-activities, 5) considering simultaneous testing for COVID-19 and TB, and 6) securing BCG-vaccine stocks and its supply chain [3].
In conclusion, Immune responses in TB and COVID-19 coinfection is depended on both innate and adaptive immunity and is complex. The current evidence demonstrates that LTBI patients demonstrate positive immunomodulation against COVID-19. Active-TB patients might have lower lymphocyte function and a lower SARS-CoV-2-specific or COVID-19-specific responses. Further urgent longitudinal studies are needed to fill several knowledge gaps. Lessons learnt from the COVID-19 pandemic can assist in the creation of the future national TB control program.
Figure 1 : Demonstrating A : Estimated TB incidence rates (2021). B : Estimated TB mortality rates in HIV-negative people (2021). C : Global trends in the estimated number of incident TB cases (left) and the incidence rate (right) (2000–2021) (shaded areas represent uncertainty intervals. The horizontal dashed line shows the 2020 milestone of the End TB Strategy). D : Global trends in the estimated number of deaths caused by TB (left) and the mortality rate (right) (2000–2021) (shaded areas represent uncertainty intervals. The horizontal dashed line shows the 2020 milestone of the End TB Strategy) [1].
Figure 2 : Demonstrating the immune response in COVID-19 and active tuberculosis. The Th1 response potentiates macrophage activity and the Th17 response favors the recruitment and activation of neutrophils with release of harmful products to the host tissue, further exacerbating the inflammatory process. To appease these responses, an elevated production of IL-10 and differentiation of Treg occurs, however, this generates a low immunologic potential. This response caused by M. tuberculosis generates an unfavorable immune microenvironment for the response against SARS-CoV-2 [2].
References
1.Falzon D, Zignol M, Bastard M, Floyd K, Kasaeva T. The impact of the COVID-19 pandemic on the global tuberculosis epidemic. Frontiers in Immunology 2023.
DOI : 10.3389/fimmu.2023.1234785
2.Flores-Lovon K, Ortiz-Saavedra B, Cueva-Chican?a LA, Aperrrigue-Lira S, Montes-Madariaga ES, Soriano-Moreno DR, et al. Immune responses in COVID-19 and tuberculosis coinfection : a scoping review. Frontiers in Immunology 2022.
DOI : 10.3389/fimmu.2022.992743
3.Jeong Y, Min J. Impact of COVID-19 pandemic on tuberculosis preventive services and their post-pandemic recovery strategies : a rapid review of literature. J Korean Med Sci 2023 Feb 6; 38 (5) : e43. DOI : https://doi.org/10.3346/jkms.2023.38.e43