Endoscopic Management of Bile Leaks After Cholecystectomy Is There a Treatment of Choice?
Endoscopic Management of Bile Leaks After Cholecystectomy
Is There a Treatment of Choice?
Ivano Biviano1, Sinan Sadalla*1, Pietro Maria Barazzoni1, Zhaohan Wang2, Alessia D'Ignazio3,
Alessia Santini1, Elena Gianni1 and Raffaele Macchiarelli1
1.Gastroenterology and Operative Endoscopy Unit; Azienda Ospedaliero-Universitaria Senese
“Le Scotte” Policlinico, 53100 Siena, Italy
2.Department of Gastroenterology and Hepatology, Jiangxi Provincial People’s Hospital, Nanchang University, Nanchang, China.
3.Department of General Surgery and Surgical Oncology, University of Siena, Italy.
*Correspondence to: Ivano Biviano, viale Mario Bracci, 11 - 53100 Siena, Italy.
Copyright
© 2023 Ivano Biviano. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 November 2023
Published: 13 December 2023
Abstract
Background. Iatrogenic bile duct injuries (BDI) are common post-cholecystectomy complications. Endoscopic retrograde cholangiopancreatography (ERCP) is the first-line treatment, but it is not clear what is the best endotherapy option.
The aim of this study was: to evaluate the efficacy of endoscopic treatment for biliary leaks (BLs) after cholecystectomy; to investigate the predictive factors to guide treatment; to evaluate the best option between plastic (PS) or fully covered self-expandable metallic stents (FCSEMS).
Methods. We retrospectively analyzed data of all patients with BLs after cholecystectomy who underwent ERCP between 2011 and 2022. The severity of the leak was classified according to Amsterdam Criteria. Endoscopic treatment consisted of endoscopic sphincterotomy alone (ES) or sphincterotomy and stenting (EST). The resolution of the leak was evaluated by the biliary drainage cessation. We performed a multivariate analysis to investigate predictive factors for successful endoscopic treatment.
Results. Thirty-eight patients (13F, 66±18 years) underwent ERCP for BL. Fifteen (5F, 75±12y) were treated with EST, while 23 (8F, 61±19y) with ES, 9 (3F) of which required additional ERCP for failure. Comparing the two groups, a statistical difference was demonstrated for the presence of stenosis (p 0.015) and high-grade leak (p 0.05) in Fisher's test. Multivariate analysis revealed no predictors between the two groups (OR 1.35; 0<95%CI<2). In the EST group 14 (4F) were treated with PSs and 8 (3F) with FCSEM with a mean time of maintenance of 54±31 and 44±31 respectively (p=0,525).
Conclusions. ES alone or EST are both effective in BLs post-cholecystectomy. No predictive factors to guide endotherapy were identified; however, biliary stenting should be primarily considered in high grade leaks and in the stricture of the biliary ducts. There was no advantage in placing FCSEMS rather than PS.
Keywords: Bile Duct Leaks, endoscopic retrograde cholangiopancreatography, cholecystectomy, sphincterotomy, biliary stenting
Endoscopic Management of Bile Leaks After Cholecystectomy Is There a Treatment of Choice?
Introduction
Postoperative bile leakage is a well-known complication after cholecystectomy regardless of if it is done through open rather than laparoscopy surgery. The incidence of bile duct injuries (BDI) after video laparoscopic cholecystectomy has been estimated to be between 0,9% and 3%(1–3).
A biliary leak can be defined as loss of bile from any site in the biliary tree resulting in an increased bilirubin concentration in the abdominal cavity or abdominal drains. Several classification systems have been developed to describe iatrogenic biliary injuries including Bismuth(4), Strasberg(5), Stewart and Way(6), McMahon(7), and Hanover (8) classifications. The most common is the Amsterdam criteria(9). Anyway, for the purpose of this study, we will divide between high-grade leaks, those that show rapid extravasation of contrast from the biliary tree on initial injection, and low- grade leaks, that require complete or near complete intrahepatic filling before there is contrast medium extravasation.
The most common site of leak is the cystic duct stump, followed by aberrant biliary ducts (duct of Luschka)(9).
The first line treatment in both groups of patients is the endoscopic management with ERCP, (10) with the aim to direct bile to the duodenum while minimizing loss through the leak and to decrease the pressure in the biliary ducts. This can be achieved via transpapillary stent placement(11–13), sphincterotomy(14), or a combination of both. Even though there is no consensus on the best treatment(10,15,16), the efficacy of ERCP in diagnosing and treating BDIs is established. However, it is not possible at this time to take advantage of proven predictive rules which could help the endoscopist to decide between sphincterotomy or stent placement. Therefore, the aim of our study was to evaluate the efficacy of endoscopic treatment for biliary leaks (BLs) after videolaparoscopic cholecystectomy. The secondary point was to study predictive factors to guide the endoscopist between the different endotherapy options.
Moreover, we tried to evaluate a difference in terms of time of stent maintenance between plastic or fully covered self-expandable metallic stents (FCSEMS).
Materials and Methods
We retrospectively analysed the data of all patients referred to Siena Hospital’s Endoscopy Department for bile duct leaks after laparoscopic cholecystectomy for symptomatic cholelithiasis, who underwent ERCP during the period between January 2010 and December 2022. Data were collected in a database and a total of 41 patients were identified, most of whom came from Siena’s Surgery Unit. Exclusion criteria were BDI due to different cause than cholecystectomy and impossibility to retrace follow-up at our hospital. All the bile leaks were confirmed by means of ERCP by experienced endoscopists. The leak was classified by reviewing the endoscopic images according to the Amsterdam Criteria(9) and its severity was distinguished into high- grade and low-grade leak based on fluoroscopic findings (Fig.1). A high-grade leak was defined as the visualization of a leakage of contrast medium through the breach before total opacification of the intrahepatic biliary tree; a low-grade leak was defined as the visualization of contrast spreading through the breach right after full opacification of the biliary tree, according to the latest guidelines(17). The endoscopic therapeutic options were sphincterotomy alone (ES) or sphincterotomy and stenting (EST). In case of unsuccess of ES alone, we proceeded with an additional endoscopic procedure to insert a stent. Resolution or persistence of the leak were respectively evaluated as a reduction or persistence of bile loss from the surgical drainage. Two different types of stents were used: polyethylene prosthesis either straight or double pigtail (7 or 10 Fr and lengths between 4 and 12 cm), or FCSEMS (8-10 mm in diameter and 60-80 mm in length). We collected data about age, gender, Amsterdam classification (we also distinguished between leaks from duct of Luschka and from cystic duct within Amsterdam class A), leak’s grade, type of therapeutic option carried out, type of stent inserted, timing of stent maintenance, success or unsuccess of the procedure, occurrence of fistulas or stenosis and presence of stones in common bile duct (CBD).
Statistical analysis
Statistical analyses were performed using SPSS statistical software. Descriptive continuous variables are expressed as mean (m) and standard deviation (SD). Fischer’s exact test and Mann-Whitney U test was used to compare continuous variables and Chi square for dichotomous variables, considering the value of p ≤ 0.05 as the limit for statistical significance. We also performed a multivariate analysis (logistic regression) and the results were evaluated with a 95% confidence interval.
Results
The study population consisted of 41 patients with diagnosis of post-cholecystectomy biliary leak who underwent ERCP procedure at our Department between January 2010 and December 2019. Three patients were excluded due to impossibility to obtain adequate follow-up. Therefore, we analyzed data of 38 patients (13 females [F]).
No significant differences between the two genders were found. The median age for patients was 66±18y (range 22-87). All data and patients’ characteristics according to groups are reported on Table 1.
Patients were divided into two groups: subjects who received endoscopic sphincterotomy alone [ES Group; n.23] and those who received sphincterotomy and stenting [EST Group; n.15]. Median age for ES Group (8F; 33%) was 61±19y and 75±12y for EST Group (5F; 33%).
In ES Group, 12 patients (52%) had a leak from the cystic duct, 3 (13%) from duct of Luschka and 8 (35%) from CBD; consequently, it comes out that 15 people (65%) had Amsterdam class A leak while 8 patients had class B leak. Of the EST Group, 7 patients (47%) had a leak from cystic duct and 2 (13%) from duct of Luschka resulting in 9 subjects (60%) with Amsterdam class A leak; 6 patients had a leak from CBD meaning a class B leak.
Ten subjects (43%) in ES Group had a low-grade leak while 13 had a high-grade one; eleven patients (73%) in EST Group had a high-grade leak and 4 of them had a low- grade one.
In both groups, 4 people had stones in CBD and 2 had fistulas at the time of the procedure. Three people (13%) who received sphincterotomy alone and 5 (33%) in EST Group had stenosis of the biliary tract. No statistically differences were found between the two groups except from age.
Among the 38 patients enrolled, thirty-seven (97,4%) benefit from ERCP treatment. One failure was met because of patient’s death during follow-up. Nine subjects who received sphincterotomy alone needed a second ERCP to insert an endoprosthesis due to leak persistence.
These patients were therefore relocated into two new categories: those whose ES was a success [ES Group; n.14] and those who had a stent insertion [EST Group; n. 23] including ES failures. Data are reported in Table 2. Median age for ES Group (5F; 36%) was 66±17 years. 9 subjects (64%) had leak from cystic duct and 1 (7%) from duct of Luschka [10 patients (71%) Amsterdam class A leaks] while 4 (29%) had a leak from CBD [Amsterdam class B leak]. In EST Group there were 9 (39%) leaks from cystic duct and 4 (17%) leaks from duct of Luschka [meaning 13 patients (57%) with Amsterdam class A leaks] and 10 patients with leak from CBD [Amsterdam class B leaks]; median age for the group (7F; 30%) was 65±12 years.
ES Group was composed of 8 subjects (57%) with low-grade leak and 6 with high- grade one while EST Group consisted of 17 patients (74%) with high-grade and 6 with a low-grade one. Both Groups presented stones in CBD (3 and 5, respectively). EST Group gathered all population’s fistulas and stenosis, three and seven, respectively. In this latter Group, two patients had post procedural acute pancreatitis.
A statistically significant difference emerged about presence of stenosis comparing the two Groups (p=0,015) at Fisher’s exact Test. It also emerged a borderline significant difference (p=0,05) about presence of high-grade leak between the two Groups. However, the logistic regression did not show predictive factors may influence failure of sphincterotomy alone. Therefore, we studied the time of maintenance of 22 subjects (Table 2). No statistically relevant differences were found between the two groups at Mann-Whitney U Test.
Table 1 - Comparison between endoscopic sphincterotomy alone (ES Group) and endoscopic sphincterotomy with stent placement (EST Group) for biliary leaks post cholecystectomy
Table 2 - Comparison between success of endoscopic sphincterotomy alone (ES Group) and endoscopic sphincterotomy with stent placement including unsuccess of ES (EST Group).
Discussion
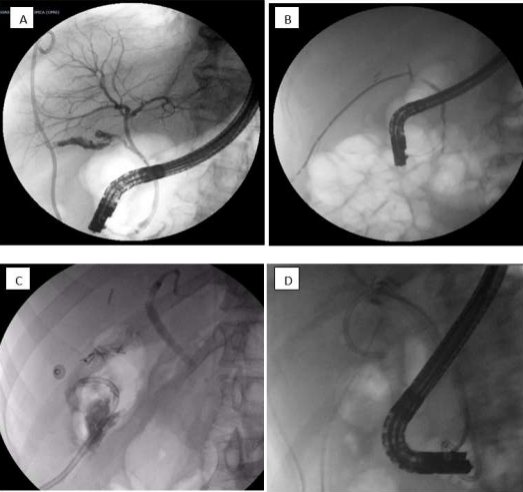
In this study we evaluate the management of post cholecystectomy biliary leaks in our centre. Among biliary injuries, bile duct leaks are the most common ones(18), being a challenge for healthcare professionals in terms of early diagnose, prompt treatment and minimal discomfort for the patient. The cause of bile leaks in our study was laparoscopic cholecystectomy and the most common site of leak was the cystic stump, as frequently reported in literature(19). Figure 1 demonstrate bile leaks and stent placement.
Figure 01 A: Low grade bile leak identified only after intrahepatic opacification; B: High grade bile leak observed before intrahepatic opacification; C: Bile leak in a patient with a cystic stump; D: Placement of plastic biliary stent
Efficacy of endoscopic treatment
In case of biliary leak, the percutaneous drainage of abdominal collections and surgery could represent a therapeutic option but, in the last decade, the endoscopic approach has become the first choice, both for diagnostic and treatment purposes(20,21). The goal is to direct biliary flow to the duodenum, minimize flow through the bile leak, and decrease pressure gradients in the biliary system, which allow the biliary ductal leak to heal on its own. This can be achieved via transpapillary stent placement(12), sphincterotomy(14), or a combination of both.
Evaluating the global efficacy of all endoscopic approach, we observed a success rate up to 97% (37 of 38 patients); resolution occurred in 14 subjects (37%) that underwent sphincterotomy and in 23 subjects (60%) who received stent placement, taking account of those who had a stent insertion after failure of sphincterotomy. Only one case of unsuccess of endoscopic treatment was observed because the patient died during the follow-up for causes not related to the procedure.
Potential predictive factors
A search of the literature showed a broad number of studies comparing endoscopic sphincterotomy alone and biliary stenting, but there is no agreement on the best approach, and no prediction rule is available to help endoscopists choosing the best treatment option(22,23). We compared age, sex, Amsterdam class, grade of leak, presence of stenosis, fistulas, and CBD stones in 38 patients. People were firstly divided into an ES group for those who primarily received an endoscopic sphincterotomy and an EST group for those who received a stent insertion, but no significant differences were met. Then we compared the same patients redistributed in an ES group composed of people who had a success of ES and an EST group composed of people who received a stent insertion in the first place and those who had failure of ES procedure and subsequent stenting of the biliary tract. The comparison brought out a significant statistical difference for presence of stenosis and for grade of leak. The latter was a borderline association, probably due to limited sample.
Assuming that interactions between “biliary stenosis” and “grade-of-leak" could influence the changeover from success to unsuccess of ES, a multivariate analysis did not show any significant interaction between the two factors, maybe due to the small number of patients under analysis. Sphincterotomy alone nowadays is reserved to cases where there are obstructing stones or when a large sphincterotomy is needed, in all other cases the combination therapy or stent monotherapy is associated with a lower rate of unsuccess as compared with sphincterotomy as monotherapy(24). Moreover sphincterotomy has been shown to have a higher complication rate in case of nondilated bile ducts as occurs in case of bile leak without retained bile duct stones. Complications include pancreatitis, haemorrhage, perforation, sepsis, and cholangitis and papillary stenosis(25).
Many authors (26) describe the superiority of stenting over sphincterotomy in terms of safety and efficacy. However, it is necessary to consider that sphincterotomy alone usually requires a single step procedure and that the overall expenses are only for use of one duodenoscope and one sphincterotome. Moreover, bile leaks above the liver bifurcation are not usually treated with the placement of stent because the drainage from the other side of the liver can be blocked. Putting the various aspects on the balance, it is interesting to identify the prediction rule to direct the patient towards the best option for his condition.
Interesting is the algorithm proposed by Sandha et al.(27), which suggests ES alone as first therapeutic approach for low-grade leaks, in opposition to direct stenting of the biliary tract as first choice for high-grade leaks. This proposal, combined with many other studies available, should warn us about over usage of stents in unnecessary situations. In their recent study Rainio et al.(26) state that ES is an efficient and cost- effective procedure to treat Amsterdam class A leaks, comparable to EST also for high- grade bile leak, with a success rate of 87%. Aksoz et al.(22)in their study with 31 patients say that ES is an optimal therapeutic option for low-grade leaks and Llach et al.(14) argued that ES alone should be considered a highly effective treatment to solve post-cholecystectomy biliary leaks as long as no stenosis exist.
The interaction between “biliary stenosis” and “grade-of-leak" factors in their impact on success or unsuccess of ES has been analyzed in the present study. We implemented a multivariate analysis considering as dependent variables “ES group” and “Unsuccess of ES (28)” and as independent variables “stenosis” and “grade of leak” but not relevant results emerged due to the small number of patients under analysis.
Differences in outcome between PSs and FCSEMSs
Stent insertion includes two different possibilities: use of a plastic stent (PS) or a self- expandable metal stent (SEMS). The choice is often led by guidelines but it is also quite common to find in the literature endoscopists who decide the treatment basing on their own experience, as it happens usually in many medical fields and also in this study. So far it is difficult to find any conclusion about the best type of stent to use and the time of maintenance.
We showed any significant difference in terms of duration of stent maintenance between plastic and metal stents, and these data are in accordance with other papers on the issue.
Limitation
In the past decade biodegradable stents appeared in clinical practice as an alternative to traditional plastic and metal stents. These devices are prominently made of polydioxanone and comes in various shapes (29-30).
The main advantage of biodegradable stents is that they allow to avoid further endoscopy exams after the first deployment. In this regard, the main scenarios for the use of biodegradable stents are the management of post-cholecystectomy leak, treatment of benign biliary strictures, prevention of post-ERCP pancreatitis, and in ampullectomy procedures (31).
The first use of an endoscopic biodegradable stent was reported in 2015 for the treatment of a post-cholecystectomy leak from the cystic duct (32).
In recent years, new shapes and type of biodegradable stents emerged. A single centre study focused on helicoidal-shaped biodegradable stents and showed that technical stent deployment was excellent. Furthermore, it demonstrated that the time of biodegradation was reliable(29).
To better understanding the management of biliary leaks, Siiki et al. compared the use of biodegradable stents with plastic stents. Their study demonstrated that biodegradable stents were highly successful and safe as the plastic stents, with the advantage of no further endoscopic procedures. Moreover, biodegradable stents showed a lower drain output compared with plastic ones (33).
Even if biodegradable stents should be a first choice in the setting of biliary leaks, these devices were not available in our setting. Therefore, in our study we focused on plastic and metal biliary stents only.
Conclusions
Endoscopic treatment with ERCP is a safe and effective therapeutic option for benign iatrogenic lesions of the biliary tract after cholecystectomy. It should be considered as first therapeutic option in treatment of bile duct injuries for its high success rate.
It has not been possible to identify any predictive factor which could help the endoscopist to choose the best therapeutic option. However, the presence of a high- grade leak and a stenosis of the biliary tract should primarily direct towards a stent insertion rather than ES alone, while the presence of a low-grade leak without evidence of any other connected pathology to the biliary tract could address the choice towards ES alone.
Reference
32. Siiki, A., Sand, J., & Laukkarinen, J. (2018). A systematic review of biodegradable biliary stents: promising biocompatibility without stent removal. European Journal of Gastroenterology & Hepatology, 30(8), 813–818. https://doi.org/10.1097/MEG.0000000000001167
33. Siiki, A., Vaalavuo, Y., Antila, A., Ukkonen, M., Rinta-Kiikka, I., Sand, J., & Laukkarinen, J. (2018). Biodegradable biliary stents preferable to plastic stent therapy in post- cholecystectomy bile leak and avoid second endoscopy. Scandinavian Journal of Gastroenterology, 53(10–11), 1376–1380. https://doi.org/10.1080/00365521.2018.1518480.