Efficacy of Intravenous Immunoglobulins for the Treatment of Sepsis in Pediatric and Neonatal Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Efficacy of Intravenous Immunoglobulins for the Treatment of Sepsis in Pediatric and Neonatal Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Shruthi Punnapu *1 Suganya Nadarajan 2 Tusharkumar Sinhal 3
1,2,3. Specialist pediatrician, Mediclinic Parkview Hospital, Dubai, UAE.
*Correspondence to: Dr. Shruthi Punnapu, Specialist pediatrician, Mediclinic Parkview Hospital, Dubai, UAE.
Copyright
© 2023: Dr. Shruthi Punnapu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 December 2023
Published: 15 December 2023
Abstract
Background: Sepsis remains a global challenge, particularly in pediatric populations. Intravenous Immunoglobulins (IVIG) have emerged as a potential adjuvant therapy for pediatric sepsis, but skepticism persists regarding their efficacy. This study aims to systematically evaluate the clinical effectiveness of IVIG in pediatric sepsis.
Methods: A systematic review and meta-analysis were conducted following PRISMA- 2020 and Cochrane Handbook guidelines. Three biomedical databases were searched for relevant studies. The primary outcome was all-cause mortality in randomized controlled trials (RCTs). Risk of bias was assessed using the Cochrane risk of bias assessment tool (RoB-II). Statistical analysis utilized Review Manager 5.3, employing a random-effects DerSimonian-Laird model.
Results: The search identified 883 references, with 19 RCTs meeting inclusion criteria. The overall meta-analysis, involving 6165 participants, demonstrated a statistically significant decrease in all-cause mortality with IVIG compared to control (OR 0.57, 95% CI 0.43 to 0.75, p < 0.0001). Subgroup analyses revealed regional variations, with RCTs conducted in Asia showing a statistically significant decrease in mortality (OR 0.38, 95% CI 0.29 to 0.51, p < 0.00001). On the other hand, Europe (OR 0.69, 95% CI 0.34 to
1.40, p = 0.30) and North America (OR 0.84, 95% CI 0.69 to 1.01, p = 0.06) showed a non-statistically significant decrease in mortality. Sensitivity analysis confirmed consistent heterogeneity, suggesting broader variations among studies.
Conclusion: This meta-analysis provides evidence supporting the effectiveness of IVIG in reducing all-cause mortality in pediatric sepsis. However, significant heterogeneity and regional variations underscore the need for further research.
Keywords: Intravenous Immunoglobulins, IVIG, Sepsis, Septic shock, Neonates, Pediatrics.
Efficacy of Intravenous Immunoglobulins for the Treatment of Sepsis in Pediatric and Neonatal Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
1.Introduction
Sepsis, characterized by life-threatening organ dysfunction resulting from a dysregulated host response to infection, remains a global challenge with substantial mortality and morbidity rates [1]. Sepsis typically begins with an infection, which can be bacterial, viral, fungal, or parasitic [2]. Common sources include pneumonia, urinary tract infections, abdominal infections, and skin infections [3]. Bacteria are the most common underlying etiology, with gram-positive bacteria like Staphylococcus aureus and Streptococcus pneumoniae, and gram-negative bacteria like Escherichia coli being frequent causes [4].
The immune system's inflammatory response, intended to eliminate the infection, can have detrimental effects when it becomes excessive. This can lead to the release of pro-inflammatory cytokines, causing systemic inflammation. Sepsis can also disrupt the normal clotting mechanisms in the blood, leading to both excessive bleeding and abnormal clot formation [5]. This can contribute to organ dysfunction [2].
The standard approach, as advocated by the Surviving Sepsis Campaign, involves rapid eradication of septic foci, administration of anti-microbial agents, and maintaining hemodynamic stability [6]. However, sepsis is a complex syndrome involving various microorganisms, each with differing virulence and resistance profiles, affecting patients with diverse comorbidities and responses to infection [7].
In the realm of pediatrics, the challenges posed by sepsis are particularly poignant [8]. Children, with their developing immune systems and unique physiological responses, demand specialized attention within the context of sepsis management [9]. Pediatric sepsis not only manifests differently than in adults but also requires a nuanced approach considering the age-specific variations in clinical presentation, diagnostics, and therapeutic interventions [10].
Moreover, the distinctive microbial landscape in pediatric sepsis necessitates a tailored antimicrobial strategy [11]. The prescription of antibiotics should be mindful of age- specific pharmacokinetics and resistance patterns prevalent in pediatric populations [12]. The need for age-appropriate dosage adjustments and careful consideration of potential adverse effects is paramount in ensuring both the efficacy and safety of antimicrobial interventions.
Intravenous immunoglobulins (IVIG), with their pleiotropic effects on inflammatory and immune mechanisms, have emerged as potential adjuvant therapy for sepsis [13]. While historical skepticism surrounded their efficacy, recent trials suggest that IVIGs may be effective in septic patients [14]. The meta-analysis conducted in this study aims to evaluate the clinical effectiveness of IVIG in pediatric sepsis, providing valuable insights for clinicians in decision-making.
Focusing specifically on children with sepsis, severe sepsis, and septic shock, this study addresses the unique challenges posed by pediatric sepsis. It explores the potential benefits of IVIG, emphasizing the need for larger trials and systematic reviews to establish robust conclusions on its therapeutic potential in pediatric and neonatal populations. The overarching goal of this research is to contribute evidence-based insights into the efficacy of IVIG treatment for pediatric sepsis.
2. Materials and Methods
We followed the Preferred Reporting Items of Systematic Reviews and Meta-analysis (PRISMA-2020) during the preparation of this manuscript [15]. The methods and analyses were conducted in strict accordance with the guidelines of the Cochrane Handbook of Systematic Review and Meta-analysis [16].
2.1. Search Strategies
We searched 3 electronic biomedical databases (namely, PubMed, Scopus, and Web of science core collection) to find potentially relevant studies. We used specific keywords to identify potentially relevant studies that investigate efficacy of IVIG for sepsis in children and neonates on electronic databases. These keywords included: “Intravenous immunoglobulins”, “IVIG”, “sepsis”, “severe sepsis”, “septic shock”, “Children”, “Neonates” …etc.
2.2. Inclusion and Exclusion Criteria
We applied pre-specified inclusion and exclusion criteria to the retrieved articles. We defined the inclusion criteria using the PICOS model as follows:
Population: Neonatal and pediatric patients < 18 years old who received a diagnosis of sepsis, severe sepsis, or septic shock
Intervention: Intravenous immunoglobulins (IVIG) Comparator: Placebo or standard care Outcomes: All-cause mortality
Study design: Randomized controlled trials (RCTs)
We omitted research conducted in languages other than English, theses, conference abstracts, and studies with unreliable data that couldn't be extracted and analyzed.
2.3. Selection of Studies
The selection criteria were applied by 2 authors. The eligibility screening process comprised two steps: initially screening abstracts to determine eligibility, followed by retrieving and screening the full-text articles of eligible abstracts to assess their eligibility for inclusion in the meta-analysis.
2.4. Data Extraction
An online data extraction sheet was constructed. The data extraction includes the following domains: (1) study ID, (2) study year, (3) country, (4) study design, (5) population definition, (6) sample size (7) available data of outcome measures (odds ratio, 95% confidence interval), and (8) quality assessment domains.
2.5. Assessment of Risk of Bias
The Cochrane risk of bias assessment tool (RoB-II) is a recommended checklist for assessing the risk of bias in RCTs [17]. In this tool, each RCT is assessed for the possibility of the following risks: (1) selection bias, by assessing the methods of random sequence generation and the concealment of patient allocation; (2) performance bias, by assessing the blinding of participants and study personnel; (3) detection bias, by assessing the blinding methods of outcome assessment process; (4) attrition bias, by evaluating the magnitude and impact of incomplete outcome data and whether incomplete data were handled by appropriate statistical analysis techniques; (5) reporting bias, by assessing the selectivity of reporting study outcomes based on the prespecified methods in the clinical trial registration; and (6) any other source of bias that might have influenced the study data.
2.6. Statistical analysis
The primary outcome of our meta-analysis is the effect of IVIG on the mortality rates. This outcome is measured using the odds ratio (OR). An OR greater than one indicates an increased mortality and an OR less than 1 indicates a decreased mortality. We used Review Manager version 5.3 for windows (RevMan) to conduct the statistical analysis. RevMan was utilized to aggregate all effect sizes (ORs) and along with their 95% confidence interval. The final combined effect estimate was calculated using a random- effects meta-analysis model employing the DerSimonian-Laird method. This model, chosen over the fixed-effects model, accommodates both within-study and between- study variability. In case of significant heterogeneity, several methods are tried to resolve the heterogeneity in accordance with Cochrane handbook [16], including conducing sensitivity and subgroup analyses and using the random-effects model.
2.7. Publication Bias
To assess publication bias, we created a funnel plot using RevMan software, plotting the pooled effect estimate against its standard error (SE). The presence of publication bias was evaluated based on the symmetry degree of the generated figure.
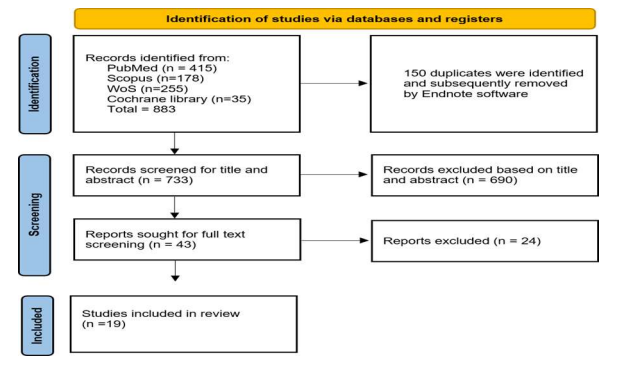
Figure 1: PRISMA flow diagram showing the study selection process.
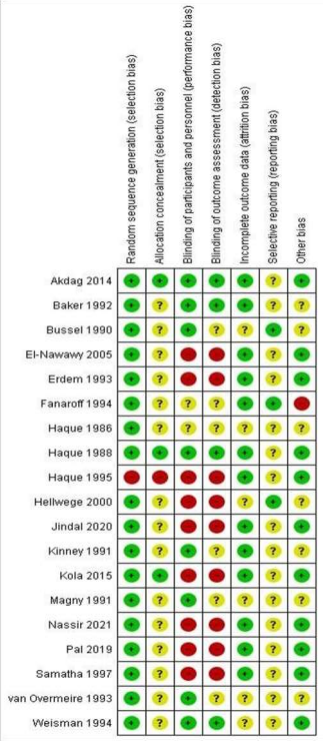
Figure 2: Risk of bias summary: authors' judgements about each risk of bias item for each included study.
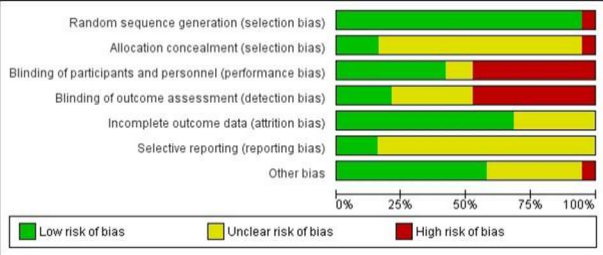
Figure 3: Risk of bias graph: authors' judgements about each risk of bias item presented as percentages across all included studies.
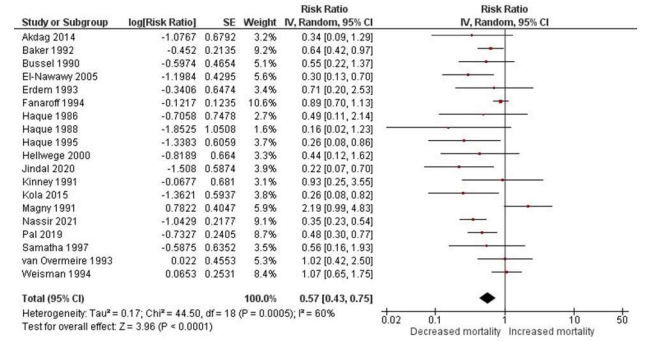
Figure 4: Forest plot for the effect of IVIGs on the all-cause mortality in children and neonates with sepsis.
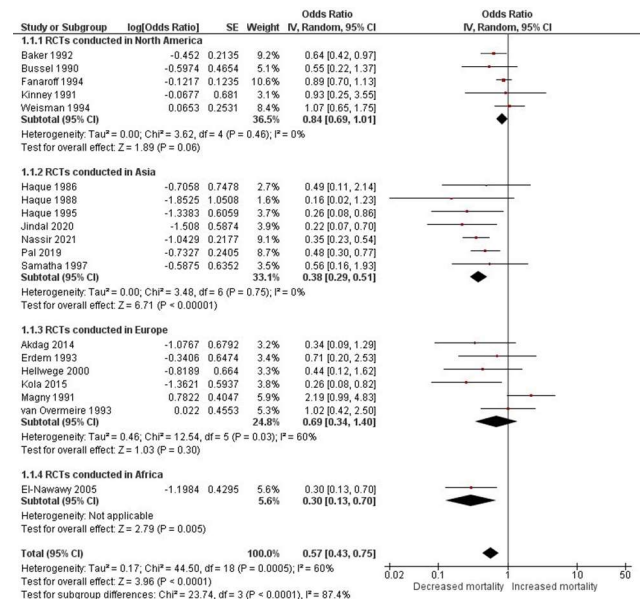
Figure 5: Forest plot for the subgroup analysis based on the geographical location.
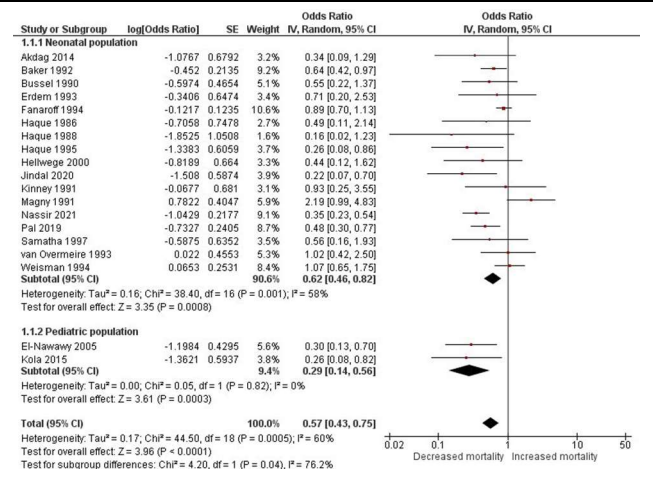
Figure 6: Forest plot for the subgroup analysis based on the study population.
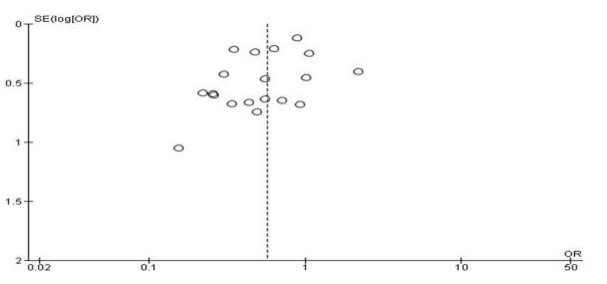
Figure 7: Funnel plot for assessment of publication bias
Table 1: Basic characteristics of the included studies.
3. Results
3.1. Search results
We identified 883 references through the computerized search, removed 150 duplicates, and screened the titles and abstracts of the remaining 733 records. We excluded 690 records after reviewing the titles and abstracts because they did not meet the prespecified inclusion criteria. The full texts of the remaining 43 studies were obtained and assessed again according to the eligibility criteria. This time, we excluded 24 studies. Finally, 19 studies fulfilled our inclusion criteria and were included in the meta-analyses (Figure 1).
3.2. Study characteristics
This present systematic review included 19 RCTs with 35 years as a span of publication time of the articles starting from 1986 and ending in 2021 (Table 1). 5 of the studies were conducted in the United States [18]–[22], 3 in the Saudi Arabia [23]–[25], 3 in India [26]–[28], 2 in Turkey [29], [30], and one in each of the following countries: Albania [31],
Belgium [32], Egypt [33], France [34], Germany [35], Iraq [36]. The total number of participants included in all studies was 6165. Among these studies, only 2 RCTs were conducted on pediatric populations [31], [33] while the rest (n= 17) were conducted on neonatal populations. After applying RoB-II to the 19 included studies, The results were obtained and presented graphically. Figure 2 shows authors' judgements about each risk of bias item for each included study and Figure 3 shows authors' judgements about each risk of bias item presented as percentages across all included studies.
3.3.Main meta-analysis results
Pooling the results from 19 RCTs showed that IVIGs are effective in decreasing all- cause mortality in children and neonates with sepsis with statistically significant results (OR 0.57, 95% CI .43 to 0.75, p < 0.0001). However, we detected significant heterogeneity in these results as evident by the Chi2 p value < 0.01 and I2 = 60%. The forest plot for the main meta-analysis is shown in Figure 4.
3.4.Sensitivity Analysis
We performed a sensitivity analysis across various scenarios by systematically excluding one study in each instance, repeating this procedure 19 times. This approach aims to examine whether a specific study significantly contributes to the observed high heterogeneity. Our findings revealed consistent heterogeneity across all scenarios, indicating that the variability cannot be solely attributed to any single study but rather arises from larger variations among the studies.
3.5. Subgroup Analysis
We conducted a subgroup analysis according to geographical location (Figure 5). RCTs conducted in North America (n = 5) showed a non-statistically significant decrease in mortality (OR 0.84, 95% CI 0.69 to 1.01, p = 0.06) with resolution of the heterogeneity (Chi2 p = 0.46, I2 = 0%). RCTs conducted in Asia (n =7 ) showed a statistically significant decrease in mortality (OR 0.38, 95% CI 0.29 to 0.51, p < 0.00001) with resolution of the heterogeneity (Chi2 p = 0.75, I2 = 0%). RCTs conducted in Europe (n = 6) showed a non-statistically significant decrease in mortality (OR 0.69, 95% CI 0.34 to 1.40, p = 0.30) with resolution of the heterogeneity (Chi2 p = 0.46, I2 = 0%). We also conducted subgroup analysis based on the study population whether pediatric or neonatal (Figure 6). RCTs that included neonates resulted in statistically significant decreased mortality due to IVIGs (OR 0.62, 95% CI 0.46 to 0.82, p < 0.0008) but with significant heterogeneity (Chi2 p = 0.001, I2 = 58%). Similarly, RCTs that included pediatric patients resulted in statistically significant results (OR 0.29, 95% CI 0.14 to 0.56, p = 0.0003) but with no significant heterogeneity (Chi2 p = 0.82, I2 = 0%).
3.6. Publication bias assessment
As shown in the funnel plot in Figure 7, the approximate symmetry of the plot indicates the absence of significant publication bias.
4.Discussion
The meta-analysis conducted in this study aimed to provide valuable insights into the clinical effectiveness of IVIG in pediatric sepsis. The comprehensive search strategy identified 19 RCTs spanning from 1986 to 2021, involving a total of 6165 participants. The main meta-analysis revealed a statistically significant decrease in all-cause mortality in children and neonates with sepsis who received IVIG compared to those receiving standard care or placebo (OR 0.57, 95% CI 0.43 to 0.75, p < 0.0001).
These results are consistent with the previous findings by Dinleyici et al. [37] who observed a clear mortality benefit based on their meta-analysis conducted on randomized as well as on prospective observational studies. However, contrary to the previous meta-analysis that mixed observational and interventional study designs, our evidence is based solely on RCTs which are considered the gold standard for establishing causation [38]. RCTs are crucial for minimizing confounding bias as they randomly assign participants to treatment groups, ensuring that potential confounding variables are equally distributed, thereby providing more robust evidence for causal relationships compared to observational studies.
Regrading other previously conducted systematic reviews on the effect of IVIG on sepsis, most of them were concerned with the adult populations. While they may not be directly related to our concern regarding the effect on neonatal and pediatric populations, discussion of their findings may reveal helpful insights. Cui et al. [39] conducted a systematic review and meta-analysis of 19 studies (15 RCTs, 4 observational studies) with a total of 1,530 adult patients. They conducted that use of IVIG significantly reduced mortality risk compared to control (RR 0.60, 95% CI 0.52– 0.69). However, no significant difference in ICU length of stay between IVIG and control groups [39].
Similarly, Yang et al. conducted a systematic review and meta-analysis 13 RCTs with a total of 1041 patients [40]. Compared to control treatment, IVIG reduced all-cause mortality in sepsis patients (OR = 0.61). However, there was some heterogeneity across studies. 6 of these RCTs reported on adverse events, which were generally minor allergic reactions related to IVIG administration [40].
The most recent of these systematic reviews was conducted in 2023 by Pan et al. [41] They included 31 RCTs examining IVIG as adjunctive therapy for sepsis. Overall, IVIG reduced mortality (RR 0.86), hospital stay (MD -4.46 days), and APACHE II scores (MD-1.65) in sepsis patients compared to control groups. Interestingly, in their subgroup analysis, they discovered that IgM-enriched IVIG significantly reduced mortality, while standard IVIG did not, which contradicts our results. This point highlights the need for well-planned RCTs for detection of the specific effects and adverse events of IgM- enriched IVIG on patients with sepsis, both children and adults.
The presence of significant heterogeneity in our overall analysis prompted further investigation. Sensitivity analysis, systematically excluding individual studies, consistently demonstrated heterogeneity, suggesting that the variability arises from larger variations among the studies rather than being attributed to a specific study. Despite efforts to explore potential sources of heterogeneity, the exact factors contributing to this variability remain unclear.
Subgroup analyses were performed to explore potential sources of heterogeneity and provide a nuanced understanding of IVIG efficacy in different populations. Geographical location-based subgroups revealed variations in outcomes, with Asia showing a statistically significant decrease in mortality (OR 0.38, 95% CI 0.29 to 0.51, p < 0.00001), while North America and Europe demonstrated non-statistically significant trends. Subgroup analysis based on the study population (neonatal vs. pediatric) demonstrated significant mortality reduction in both groups, with neonates showing significant heterogeneity.
The observed decrease in mortality associated with IVIG in pediatric sepsis is a noteworthy finding. However, the significant heterogeneity underscores the need for cautious interpretation. While the overall evidence suggests a positive effect, the varying results across subgroups warrant further investigation into factors influencing IVIG efficacy.
Considering the limited number of pediatric-specific trials, future research should prioritize large-scale RCTs focusing specifically on pediatric populations. The age- specific variations in immune response and pharmacokinetics emphasize the importance of tailored interventions in this vulnerable group. Additionally, the disparity in outcomes across geographical locations raises questions about potential regional differences in patient characteristics, healthcare practices, or IVIG administration protocols.
This meta-analysis has several limitations. The inherent heterogeneity among the included studies, along with variations in study design, populations, and IVIG protocols, introduces complexities in drawing definitive conclusions. The reliance on aggregated data and the potential for publication bias should also be acknowledged. Furthermore, the limited number of pediatric studies necessitates cautious extrapolation of findings to this specific population.
5.Conclusion
In conclusion, this meta-analysis provides evidence supporting the effectiveness of IVIG in reducing all-cause mortality in pediatric sepsis. However, the presence of significant heterogeneity and variations across subgroups highlight the need for further research to elucidate the factors influencing IVIG efficacy in different populations. Clinicians should consider the regional and age-specific nuances in pediatric sepsis management and, where appropriate, incorporate IVIG into their treatment strategies with a careful understanding of the current evidence and its limitations.
Acknowledgments: Nil
Ethical Guidelines: Ethical approval is not required as there is no direct involvement with human subjects.
Conflict of Interest: None to be declared.
References
[1]M. Bauer, H. Gerlach, T. Vogelmann, F. Preissing, J. Stiefel, and D. Adam, “Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis,” Crit. Care Lond. Engl., vol. 24, no. 1, p. 239, May 2020, doi: 10.1186/s13054-020- 02950-2.
[2]C. Caraballo and F. Jaimes, “Organ Dysfunction in Sepsis: An Ominous Trajectory From Infection To Death,” Yale J. Biol. Med., vol. 92, no. 4, pp. 629–640, Dec. 2019.
[3]M. A. Beutz and E. Abraham, “Community-acquired pneumonia and sepsis,” Clin. Chest Med., vol. 26, no. 1, pp. 19–28, Mar. 2005, doi: 10.1016/j.ccm.2004.10.015.
[4]S. P. Bergin, T. L. Holland, V. G. Fowler, and S. Y. C. Tong, “Bacteremia, Sepsis, and Infective Endocarditis Associated with Staphylococcus aureus,” Curr. Top. Microbiol. Immunol., vol. 409, pp. 263–296, 2017, doi: 10.1007/82_2015_5001.
[5]K. Moriyama and O. Nishida, “Targeting Cytokines, Pathogen-Associated Molecular Patterns, and Damage-Associated Molecular Patterns in Sepsis via Blood Purification,” Int. J. Mol. Sci., vol. 22, no. 16, p. 8882, Aug. 2021, doi: 10.3390/ijms22168882.
[6]L. Evans et al., “Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021,” Intensive Care Med., vol. 47, no. 11, pp. 1181–1247, Nov. 2021, doi: 10.1007/s00134-021-06506-y.
[7]M. Cecconi, L. Evans, M. Levy, and A. Rhodes, “Sepsis and septic shock,” Lancet Lond. Engl., vol. 392, no. 10141, pp. 75–87, Jul. 2018, doi: 10.1016/S0140- 6736(18)30696-2.
[8]B. M. Emr, A. M. Alcamo, J. A. Carcillo, R. K. Aneja, and K. P. Mollen, “Pediatric Sepsis Update: How Are Children Different?,” Surg. Infect., vol. 19, no. 2, pp. 176– 183, 2018, doi: 10.1089/sur.2017.316.
[9]S. L. Weiss et al., “Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children,” Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc., vol. 21, no. 2, pp. e52–e106, Feb. 2020, doi: 10.1097/PCC.0000000000002198.
[10]K. W. E. Hilarius, P. W. Skippen, and N. Kissoon, “Early Recognition and Emergency Treatment of Sepsis and Septic Shock in Children,” Pediatr. Emerg. Care, vol. 36, no. 2, pp. 101–106, Feb. 2020, doi: 10.1097/PEC.0000000000002043.
[11]K. Sands et al., “Characterization of antimicrobial-resistant Gram-negative bacteria that cause neonatal sepsis in seven low- and middle-income countries,” Nat. Microbiol., vol. 6, no. 4, pp. 512–523, Apr. 2021, doi: 10.1038/s41564-021-00870-7.
[12]L. B. Mau and V. Bain, “Antimicrobial Therapy in Pediatric Sepsis: What Is the Best Strategy?,” Front. Pediatr., vol. 10, p. 830276, 2022, doi: 10.3389/fped.2022.830276.
[13]M. Shankar-Hari, M. B. Madsen, and A. F. Turgeon, “Immunoglobulins and sepsis,” Intensive Care Med., vol. 44, no. 11, pp. 1923–1925, Nov. 2018, doi: 10.1007/s00134-018-5047-6.
[14]R. Domizi et al., “IgM-enriched immunoglobulins (Pentaglobin) may improve the microcirculation in sepsis: a pilot randomized trial,” Ann. Intensive Care, vol. 9, no. 1, p. 135, Dec. 2019, doi: 10.1186/s13613-019-0609-5.
[15]M. J. Page et al., “The PRISMA 2020 statement: an updated guideline for reporting systematic reviews,” Syst. Rev., vol. 10, no. 1, p. 89, Dec. 2021, doi: 10.1186/s13643-021-01626-4.
[16]J. P. Higgins and S. Green, Eds., Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series, 1st ed. Wiley, 2008. doi: 10.1002/9780470712184.
[17]J. P. T. Higgins et al., “The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials,” BMJ, vol. 343, p. d5928, Oct. 2011, doi: 10.1136/bmj.d5928.
[18]C. J. Baker, M. E. Melish, R. T. Hall, D. T. Casto, U. Vasan, and L. B. Givner, “Intravenous immune globulin for the prevention of nosocomial infection in low- birth-weight neonates. The Multicenter Group for the Study of Immune Globulin in Neonates,” N. Engl. J. Med., vol. 327, no. 4, pp. 213–219, Jul. 1992, doi: 10.1056/NEJM199207233270401.
[19]J. B. Bussel, “Intravenous gammaglobulin in the prophylaxis of late sepsis in very- low-birth-weight infants: preliminary results of a randomized, double-blind, placebo- controlled trial,” Rev. Infect. Dis., vol. 12 Suppl 4, pp. S457-461; discussion S461- 462, 1990, doi: 10.1093/clinids/12.supplement_4.s457.
[20]A. A. Fanaroff et al., “A controlled trial of intravenous immune globulin to reduce nosocomial infections in very-low-birth-weight infants. National Institute of Child Health and Human Development Neonatal Research Network,” N. Engl. J. Med., vol. 330, no. 16, pp. 1107–1113, Apr. 1994, doi: 10.1056/NEJM199404213301602.
[21]J. Kinney et al., “Efficacy and pharmacokinetics of intravenous immune globulin administration to high-risk neonates,” Am. J. Dis. Child. 1960, vol. 145, no. 11, pp. 1233–1238, Nov. 1991, doi: 10.1001/archpedi.1991.02160110025013.
[22]L. E. Weisman et al., “Intravenous immune globulin prophylaxis of late-onset sepsis in premature neonates,” J. Pediatr., vol. 125, no. 6 Pt 1, pp. 922–930, Dec. 1994, doi: 10.1016/s0022-3476(05)82011-6.
[23]K. N. Haque, M. H. Zaidi, S. K. Haque, H. Bahakim, M. el-Hazmi, and M. el- Swailam, “Intravenous immunoglobulin for prevention of sepsis in preterm and low birth weight infants,” Pediatr. Infect. Dis., vol. 5, no. 6, pp. 622–625, 1986, doi: 10.1097/00006454-198611000-00004.
[24]K. N. Haque, M. H. Zaidi, and H. Bahakim, “IgM-enriched intravenous immunoglobulin therapy in neonatal sepsis,” Am. J. Dis. Child. 1960, vol. 142, no. 12, pp. 1293–1296, Dec. 1988, doi: 10.1001/archpedi.1988.02150120047038.
[25]K. N. Haque, C. Remo, and H. Bahakim, “Comparison of two types of intravenous immunoglobulins in the treatment of neonatal sepsis,” Clin. Exp. Immunol., vol. 101, no. 2, pp. 328–333, Aug. 1995, doi: 10.1111/j.1365-2249.1995.tb08359.x.
[26]“Jindal SV, Gohil JR, Nikhileshwar A. Efficacy of IgM-rich immunoglobin for treating bacterial sepsis in very-low-birth-weight preterm neonates. Perinatology. (2020) 20(4):114–9.”
[27]“Pal S, Banerjee S, Roy B, Chattopadhyay A, Mazumder T, Bandyopadhyay S, et al. A study to see the efficacy of IGM enriched IVIG in reducing mortality in neonatal sepsis. Sch Bull. (2019) 5(7):370–3. doi: 10.21276/sb.2019.5.7.9.”
[28]“Samatha S, Jalalu MP, Hegde RK, Vishwanath D, Maiya PP. Role of IgM enriched intravenous immunoglobulin as an adjuvant to antibiotics in neonatal sepsis. Karnataka Pediatr J. (1997) 11(3):1–6.”
[29]A. Akdag, U. Dilmen, K. Haque, D. Dilli, O. Erdeve, and T. Goekmen, “Role of Pentoxifylline and/or IgM-Enriched Intravenous Immunoglobulin in the Management of Neonatal Sepsis,” Am. J. Perinatol., vol. 31, no. 10, pp. 905–912, Feb. 2014, doi: 10.1055/s-0033-1363771.
[30]G. Erdem, M. Yurdakök, G. Tekinalp, and F. Ersoy, “The use of IgM-enriched intravenous immunoglobulin for the treatment of neonatal sepsis in preterm infants,” Turk. J. Pediatr., vol. 35, no. 4, pp. 277–281, 1993.
[31]E. Kola, E. Çelaj, I. Bakalli, R. Lluka, G. Kuli-Lito, and S. Sallabanda, “Efficacy of an IgM preparation in the treatment of patients with sepsis: a double-blind randomized clinical trial in a pediatric intensive care unit,” South East. Eur. J. Public Health SEEJPH, 2014, doi: 10.4119/seejph-1770.
[32]B. van Overmeire, S. Bleyaert, P. J. van Reempts, and K. J. van Acker, “The use of intravenously administered immunoglobulins in the prevention of severe infection in very low birth weight neonates,” Biol. Neonate, vol. 64, no. 2–3, pp. 110–115, 1993, doi: 10.1159/000243980.
[33]A. El-Nawawy, H. El-Kinany, M. Hamdy El-Sayed, and N. Boshra, “Intravenous Polyclonal Immunoglobulin Administration to Sepsis Syndrome Patients: A Prospective Study in a Pediatric Intensive Care Unit,” J. Trop. Pediatr., vol. 51, no. 5, pp. 271–278, Oct. 2005, doi: 10.1093/tropej/fmi011.
[34]J. F. Magny et al., “Intravenous immunoglobulin therapy for prevention of infection in high-risk premature infants: report of a multicenter, double-blind study,”
Pediatrics, vol. 88, no. 3, pp. 437–443, Sep. 1991.
[35]“Hellwege HH, Seitz RC. Efficacy of Pentaglobin—an IgM enriched intravenous human immunoglobulin—in the treatment of neonatal sepsis. (2000). Biotest data on file.”
[36]K. F. Nassir, Y. I. Al-Saddi, H. M. Abbas, Q. A. Al Khames Aga, L. A. Al Khames Aga, and A. A. Oudah, “Pentaglobin (immunoglobulin M-enriched immunoglobulin) as adjuvant therapy for premature and very low-birth-weight neonates with sepsis,” Indian J. Pharmacol., vol. 53, no. 5, pp. 364–370, 2021, doi: 10.4103/ijp.ijp_881_20.
[37]E. C. Dinleyici et al., “Clinical efficacy of IgM-enriched immunoglobulin as adjunctive therapy in neonatal and pediatric sepsis: a systematic review and meta- analysis,” Front. Pediatr., vol. 11, p. 1239014, Aug. 2023, doi: 10.3389/fped.2023.1239014.
[38]J. Worrall, “Causality in medicine: getting back to the Hill top,” Prev. Med., vol. 53, no. 4–5, pp. 235–238, Oct. 2011, doi: 10.1016/j.ypmed.2011.08.009.
[39]J. Cui et al., “The clinical efficacy of intravenous IgM-enriched immunoglobulin (pentaglobin) in sepsis or septic shock: a meta-analysis with trial sequential analysis,” Ann. Intensive Care, vol. 9, no. 1, p. 27, Dec. 2019, doi: 10.1186/s13613- 019-0501-3.
[40]Y. Yang, X. Yu, F. Zhang, and Y. Xia, “Evaluation of the Effect of Intravenous Immunoglobulin Dosing on Mortality in Patients with Sepsis: A Network Meta-analysis,” Clin. Ther., vol. 41, no. 9, pp. 1823-1838.e4, Sep. 2019, doi: 10.1016/j.clinthera.2019.06.010.
[41]B. Pan, P. Sun, R. Pei, F. Lin, and H. Cao, “Efficacy of IVIG therapy for patients with sepsis: a systematic review and meta-analysis,” J. Transl. Med., vol. 21, no. 1, p. 765, Oct. 2023, doi: 10.1186/s12967-023-04592-8.