ST Elevation Durind Stresstest-a Stressfull Time for the Clinician.
ST Elevation Durind Stresstest-a Stressfull Time for the Clinician.
Shaju Padman Panattil*1, Priya Muralidharan2, Anandu Rajendran3, Durga Prasad4, Prashanth Panduranga5.
*Correspondence to: Dr. Shaju Padman Panattil, NMC Speciality Hospital.
P O Box 613, PC 133, Al Ghoubra, Muscat, Sultanate of Oman.
Copyright
© 2023 Shaju Padman Panattil. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 December 2023
Published: 30 December 2023
Abstract
Transient ST elevation during stress test can be associated with severe coronary artery disease. Here we report a patient with severe coronary artery disease who presented with significant reversible ST elevation during treadmill testing.
ST Elevation Durind Stresstest-a Stressfull Time for the Clinician.
Introduction
Transient ST elevation can occur stress testing. Most of the patients have severe coronary artery disease. However exercise induced ST elevation has also been reported secondary to coronary spasm. Coronary slow flow -also called Cardiac syndrome Y have been reported in patient with exercise induced ST elevation. Here we present a patient without any cardiac risk factors,who developed reversible ST elevation on stress test.
Case Report
A 42 year old male with no cardiac risk factors presented with exertional angina class 2 since 3 weeks.
His ECG and cardiac enzymes were normal.
His echocardiogram was also normal.
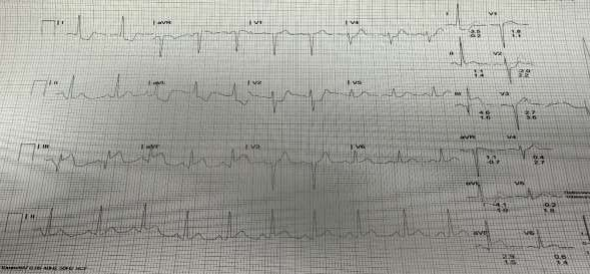
However his Treadmill Test was strongly positive for inducible ischaemia.
He developed ST elevation in lead 3,avf,along with ST depression 1,AVL,V3-V5.
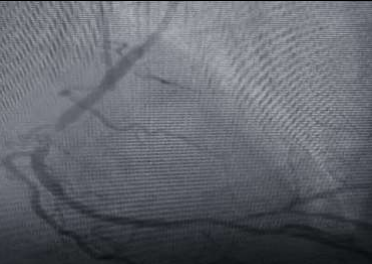
Coronary angiogram was performed.
Right coronary artery had mid 95% stenosis followed by RPL with osteoproximal 80% stenosis.RPL was a short vessel.
He underwent PTCA to RCA with DES (3 /16 mm) with good results.
He was asymptomatic on followup.
Figure 1
Figure 2: ST elevation TMT report
Discussion
The incidence of acute ST elevation during treadmill test is 0.78% in those without prior history of myocardial infarction. This is often associated with critical coronary obstruction. ST elevation during stress test has also been reported secondary to acute severe rise in pulmonary pressure and RV dilatation. ST elevation in AVR can be associated with left main stenosis. Without pathological q waves exercise induced ST elevation indicates significant proximal coronary stenosis or epicardial coronary spasm. When pathological q waves are present exercise induced ST elevation is usually indicative of LV aneurysm.
Conclusion
Exercise induced ST elevation is an important finding during stress test which can signify significant coronary artery disease.
Reference
1.Arteriographic correlation in 38 patients Am J Cardiol 1980.45(4);762-8.
2.Speechia et al Significance of exercise induced ST elevation in patients without myocardial infarction.Circulation 1981;63;46-53.
3.Celik T, Iyisoy A, Kursaklioglu H, Yuksel C, Turhan H, Isik E. ST elevation during treadmill exercise test in a young patient with slow coronary flow: a case report and review of literature. Int J Cardiol. 2006 Sep 20;112(2):e1-4.
4.Murphy JC, Scott PJ, Shannon HJ, Glover B, Dougan J, Walsh SJ, Adgey AA. ST elevation on the exercise ECG in patients presenting with chest pain and no prior history of myocardial infarction. Heart. 2009;95:1792 7.
5.Chahine RA, Raizner AE, Ishimori T. The clinical significance of exercise-induced ST-segment elevation. Circulation. 1976;54:209 13.
6.Nguyen TH, Clavijo LC, Naqvi TZ. Acute ST segment elevation during exercise stress echocardiography due to severe pulmonary hypertension. Cardiovasc Ultrasound. 2011 Jun 6;9:18. doi: 10.1186/1476-7120-9-18.
7 .Ghaffori S et al- Predictive value of exercise stress test induced ST segment changes in lead V1 and AVR in determining angiographic coronary involvement. Ann.Non invasive electrocardiol.2017;22;e12370.
8.Libby,Bonow et al Braunwalds Heart Disease-a text book of cardiovascular medicine 12th edition page-183.