Sarcoidosis With COVID-19
Sarcoidosis With COVID-19
Attapon Cheepsattayakorn1,3*, Ruangrong Cheepsattayakorn2, Porntep Siriwanarangsun3*
1. 10th Zonal Tuberculosis and Chest Disease Center, Chiang Mai, Thailand.
2. Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
3. Faculty of Medicine, Western University, Pathumtani Province, Thailand.
Correspondence to: Attapon Cheepsattayakorn, 10th Zonal Tuberculosis and Chest Disease Center, 143 Sridornchai Road Changklan Muang Chiang Mai 50100 Thailand Tel : 66 53 140767 ; 66 53 276364 ; Fax : 66 53 140773 ; 66 53 273590 ; Email : Attapon1958@gmail.com
Copyright
© 2024 Attapon Cheepsattayakorn. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 January 2024
Published: 17 January 2024
Sarcoidosis With COVID-19
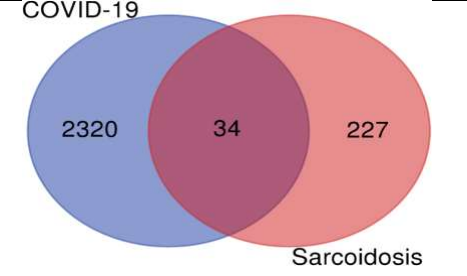
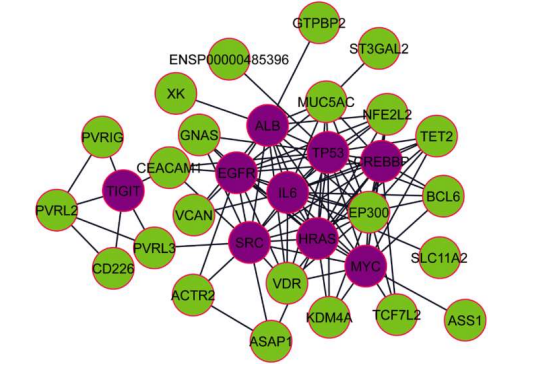
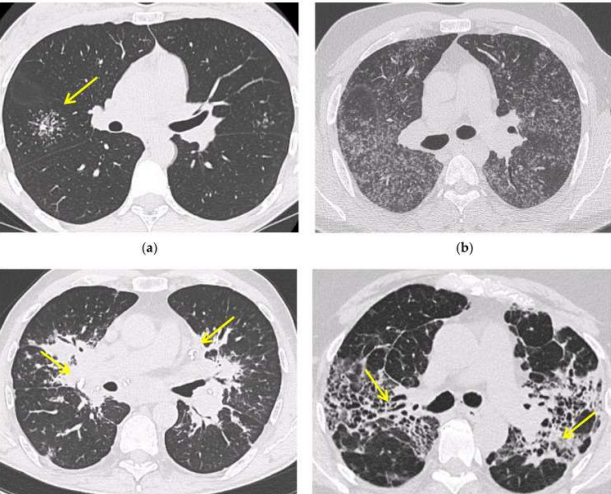
Several post-COVID-19 inflammatory disorders and autoimmune diseases have been discovered [1] since global COVID-19 pandemic started [2]. Association between these diseases is still to be investigated [2]. Common genes between COVID-19 and sarcoidosis are demonstrated in Figure 1, 2 [3]. Nevertheless, sarcoidosis organ involvement, demographics, and type of sarcoidosis treatment at the time of COVID-19 diagnosis are related to hospital admission, non-invasive ventilation or high flow oxygenation, intubation [4]. A retrospective hospital-based cohort study of 585 French sarcoidosis patients in 2017, demonstrated an estimate of a 5 % frequency of severe infections that resulting in hospital admission and death [5]. A typical HRCT feature in sarcoidosis is the presence of well-defined micronodules scattered along the broncho-vascular bundle, veins, fissures and pleura in a characteristic lymphatic distribution. Occasionally, “ galaxy sign ”,a highly suggestive of pulmonary sarcoidosis (predominance of a mid-to-upper lung zones) may demonstrates conglomerate masses that are surrounded by a multitude of micronodules (Figure 3) [6].
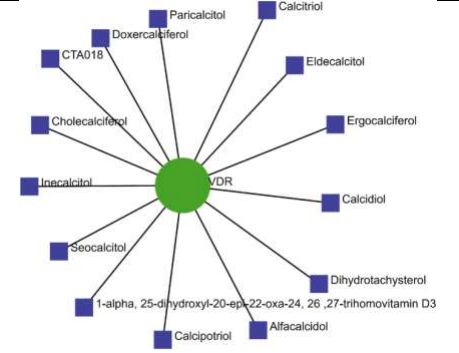
Where VDR dominantly connected to 14 different kinds of drug, protein drug interaction network collected from DrugBank provides proper treatment. Vitamin D and some of its analogous compounds might play significant roles in modulating both COVID-19 and sarcoidosis conditions is indicated by this network (Figure 4) [3].
Besides sarcoidosis of lungs, symptomatic and accidental extrapulmonary sarcoidosis is also found around the world (Figure 5, 6, 7) [7-9].
In conclusion, hub gene identification might have significant roles in modulating sarcoidosis and COVID-19 infection. In the literature, cases with sarcoid-like granuloma have been reported very few. Sarcoid-like immune response to COVID-19 could be noncaseating granulomas due to short time from disease to develop granuloma.
Figure 1 : Demonstrating a Venn diagram of commonly differentially expressed upregulated genes. Common 34 upregulated genes were identified from 2320 upregulated genes of COVID-19 infection and 227 upregulated genes of sarcoidosis [3].
Figure 2 : Demonstrating protein-protein interactions (PPIs) network for common upregulated genes from COVID-19 and sarcoidosis. The light green color nodes indicate common upregulated genes. Network consists of 32 nodes and 102 edges [3].
Figure 3 : Demonstrating irregularly marginated nodule surrounded by multiple small nodules (“Galaxy sign”, yellow narrow), this is typical of sarcoidosis (a); ground-glass-like increased attenuation resulting from diffuse micronodules randomly distributed (“Miliary sarcoidosis”) (b); enlarged and partially calcified (yellow narrows) bilateral hilar lymph nodes (c); fibrotic sarcoidosis with cystic changes and traction bronchiectases (yellow narrows) predominantly in the perihilar region and upper lobes. Nodular abnormalities are minimal/absent, but the appearance and the location of the fibrosis are very suggestive of the diagnosis of sarcoidosis (d) [6].
Figure 4 : Demonstrating drugs protein interaction network [3].
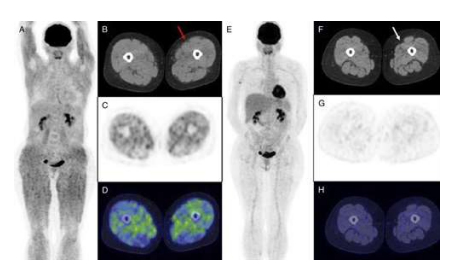
Figure 5 : Demonstrating isolated muscular sarcoidosis, revealed by hypercalcemia and 18F-FDG PET/CT [7].
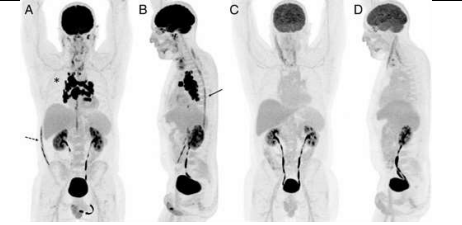
Figure 6 : 18F-FDG PET/MRI for Diagnosis and Treatment Efficacy Evaluation of Spinal Sarcoidosis [8].
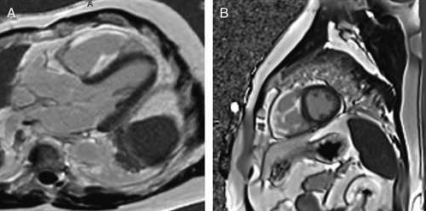
Figure 7 : Demonstrating FDG PET of Isolated Right Ventricular Sarcoidosis [9].
References
1. Galeotti C, Baryl J. Autoimmune and inflammatory diseases following COVID-19. Nat Rev Rheumatol 2020; 16 (8) : 413-414.
2. Racil H, Znegui T, Maazoui S, Touil A, Habibech S, Henda N, et al. Can coronavirus disease 2019 induce sarcoidosis : a case report. Thorac Res Pract 2023; 24 (1) : 45-48.
DOI : 10.5152/.ThoracResPract.2023.22076
3. Mogal R, Sovupa SA, Junayed A, Mahmod R, Abedin Z, Sikder S. Common genetic aspects between COVID-19 and sarcoidosis : a network-based approach using expression data. Biochemistry and Biophysics Reports 2022; 29 : 101219.
4. Nadeem O, Sharma A, Alaouie D, Bradley P, Ouellette D. Outcome in patients with sarcoidosis diagnosed with COVID-19. Presentation at Chest 2021 annual meeting, October 2021, 17-20.
DOI : https://doi.org/10.1016/j.chest.2021.07.1161
5. Dureault A, Chapelon C, Biard L, et al. Severe infections in sarcoidosis : incidence, predictors and long-term outcome in a cohort of 585 patients. Medicine (Baltimore) 2017; 96 : e8846.
6. Bernardinello N, Petrarulo S, Balestro E, Cocconcelli E, Veltkamp M, Spagnolo P. Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics (Basel). 2021 Aug 28;11(9):1558.
DOI : 10.3390/diagnostics11091558.
7. Dhomps A, Thibault F, Streichenberger N, Andrea S, Jeremie T. Isolated muscular sarcoidosis revealed by hypercalcemia. Clinical Nuclear Medicine 44(10):p 824-825, October 2019.
DOI: 10.1097/RLU.0000000000002678
8. Ashjan K, Darejan B, Lea F, Mathilde H, Vincent P, Imperiale, Alessio I. 18F-FDG PET/MRI for diagnosis and treatment efficacy evaluation of spinal sarcoidosis. Clinical Nuclear Medicine 49(1):p e28-e30, January 2024. DOI: 10.1097/RLU.0000000000004968
9. Alan S, Dagmar HS. FDG PET of Isolated Right Ventricular Sarcoidosis. Clinical Nuclear Medicine 48(2):p 184-185, February 2023. DOI: 10.1097/RLU.00000000000044013