Desmoplastic Fibroma of Bone: A Rare Bone Tumor – Single Institution Experience of 4 Cases.
Desmoplastic Fibroma of Bone: A Rare Bone Tumor – Single Institution Experience of 4 Cases.
Dr Yogarakshith A.R 1*, Dr Pramod S Chinder2, Dr. Narendra Singh Butola 3
1,3. Fellow in musculoskeletal oncology, HCG Cancer Centre, Bengaluru.
2. Head of Dept. Musculoskeletal Oncolgy, HCG Cancer Centre, Bengaluru.
*Correspondence to: Dr. Yogarakshith A.R, Fellow in musculoskeletal oncology, HCG Cancer Centre, Bengaluru.
Copyright.
© 2024 Dr. Yogarakshith A.R. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 January 2024
Published: 27 January 2024
DOI: https://doi.org/10.5281/zenodo.14185363
ABSTRACT
Background: Bone desmoid fibromatosis is a rare benign tumor characterized by infiltrative growth and a high propensity for local recurrence. There is no consensus on the optimal treatment strategy for bone desmoid fibromatosis, and surgical resection remains the primary treatment option.
Methods: We present a case series of four patients diagnosed with bone desmoid fibromatosis, all of whom were treated at our institution. Preoperative imaging, histopathological evaluation, and clinical data were collected for each patient. Surgical options included –wide local excision, Extended curettage involved thorough intralesional curettage, followed by adjuvant techniques such as thermal ablation and local adjuvants. All patients underwent regular follow-up evaluations, including clinical examination and imaging studies, to assess recurrence.
Results: The four patients included in the case series were aged between 21 and 35 years. All patients underwent successful surgical procedure without any intraoperative complications. Histopathological examination confirmed the diagnosis of bone desmoid fibromatosis in all cases. During the follow-up period, one of the patients exhibited tumor recurrence who underwent repeat surgery . Functional outcomes were excellent, and patients experienced minimal postoperative morbidity.
Conclusion: This case series highlights surgical management as an effective treatment strategy for bone desmoid fibromatosis. Our results demonstrate one recurrence among four patients during follow-up, suggesting that extended curettage/wide local excision may offer a favorable outcome.
Keywords: Fibromatosis, Intra-ossous fibromatosis, Benign bone tumor.
Abbreviations: MRI-Magnetic resonance imaging.
Desmoplastic Fibroma of Bone: A Rare Bone Tumor – Single Institution Experience of 4 Cases.
Introduction
A rare primary bone tumour known as desmoplastic fibroma shares structural similarities with its soft tissue equivalent, the desmoid-type fibromatosis that is frequently observed in the abdomen wall. It was initially described by Jaffe in 1958 and there are roughly 270 known instances in literature accounting for less than 0.1% of primary bone tumours (1). The histological criteria for desmoplastic fibroma have since been clarified by a number of writers; in 2013, the World Health Organisation reported that the microscopic appearance of this condition is comprised of thin, spindle-to-stellate cells with little cytological atypia and a lot of collagenous matrix.(2). Desmoplastic fibromas were thought by some to be the osseous equivalent of extraabdominal desmoid tumours due to their infiltrative growth pattern [3]. Nevertheless, a recent investigation found that desmoplastic fibromas of bone could be genetically distinguished from desmoid-type fibromatosis because exon 3 of CTNNB1, which codes for B-catenin, was unmutated [4]. Patients usually arrive with discomfort and localised swelling. A lucent, expansile lesion that is trabeculated and frequently has lobulated edges can be seen on plain radiographs (5). Cortical thinning with breakthrough and a soft-tissue mass may also be detected (6). The literature on desmoplastic fibroma of the bone is limited to a few dispersed case reports in the literature on radiography, orthopaedics, and pathology because it is a rather uncommon tumour. We describe our experience with four instances, all of which had different manifestations before a biopsy revealed a desmoplastic fibroma.
Methods
All patients treated at our unit with a diagnosis of desmoplastic fibroma of bone were located by a retrospective search of a cancer database. A multidisciplinary evaluation of the patient's clinical history, relevant radiological imaging, and histological results led to the confirmation of the diagnosis. The site of the disease, the management, and the patient's demographics were all documented. The end-points of the study were local recurrence and the requirement for revision surgery.
Results
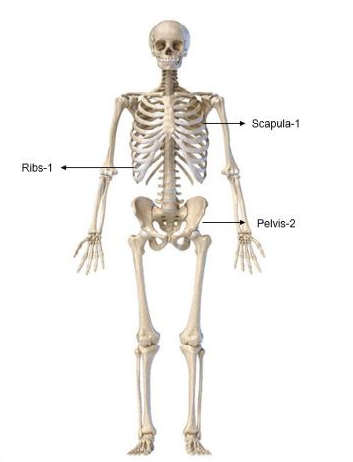
31 cases of fibromatosis were found in our database, which has data on over 10,000 patients, including those with benign bone tumours. Of these patients, 4 had desmoplastic fibroma of the bone, meaning that the incidence of fibromatosis in our population was 0.04%. Out of which three (75%) were men and one (25%) was a woman. The average age was 29.25 years (range: 21–35 years old). The skeletal distribution was one scapula, two pelvises, and one chest wall- rib. Fig-1.
The clinical symptoms were, pain, swelling, or a combination of both was found in two patients.
All patients had been referred to our hospital with suspicious plain radiographs following a history of pain/swelling of the affected body area and subsequently underwent magnetic resonance imaging, PET scan when necessary and J- needle biopsy to confirm the diagnosis. Histopatholoical diagnosis fibromatosis was established before planning of surgical procedure.
Out of 4 patients 2 underwent wide local excision and 2 patients underwent extended curettage along with reconstruction with cement based on the location of the tumor. 2 Patients who had pelvic lesion underwent extended curettage along with reconstruction with poly-methyl methacrylate cement, in one patient k-wire was used along with cement for stability.
Figure 1,2,3,4,5,6
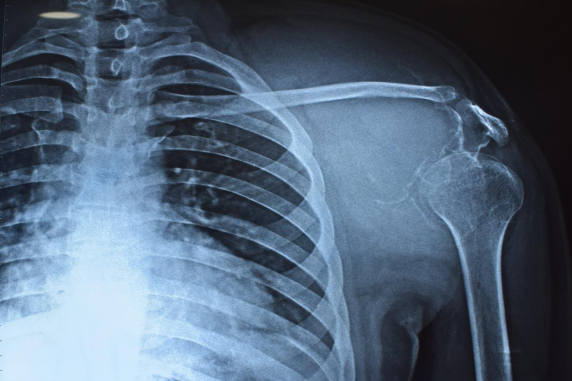
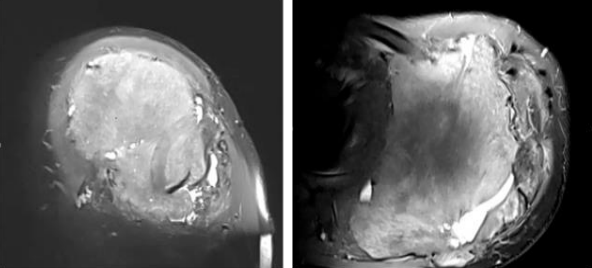
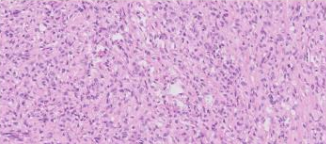
Case 1- 21 year old male who presented with pain and swelling over the left scapular area , was diagnosed with left scapula fibromatosis underwent wide local excision of tumour in 2014 after clinico-radiological evaluation and post-op histopathology confirmed to be Intra-osseous fibromatosis, after 6 years patient presented with pain and local swelling and upon evaluation with X-ray Fig-2 and MRI which showed Hyper-intense lesion on T2 sequence measuring 11.2x14.5x11.3cm with destruction of scapula body and spine with soft tissue deep to the deltoid - coronal and axial images Fig-3 and Biopsy confirmed to have local recurrence and considering chance of recurrence again patient underwent Type 3 intra-articular scapulectomy with gross histopathology image and microscopic image Fig-4. And currently on 3 year follow up and no local recurrence.
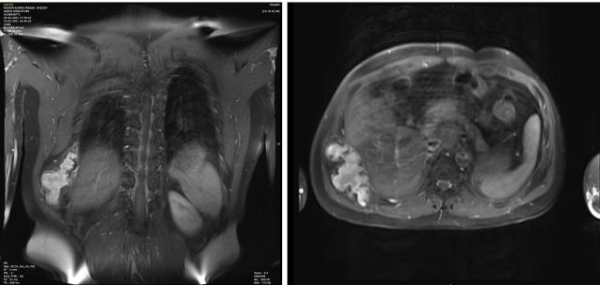
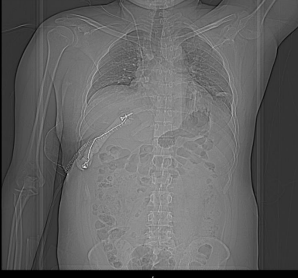
Case 2- 35 year old male who presented with a chest wall swelling and pain upon evaluation MRI was suggestive of a T1 intermediate and T2/STIR intermediate to Hyper-intense lesion from the Right 9 rib with extra-osseous soft-tissue component – coronal and axial images Fig-5 and histo-pathologically was found to have introsseous fibromatosis of the 9th rib. Following multidisciplinary team discussion and keeping in mind about the extra-osseous component and complex location of tumor patient was planned for a wide local excision of the tumor. The tumor was removed En-bloc along with part of the 10th rib because of the close proximity to 10th rib. Reconstruction was done using screws fixed to the cut ends of the bone and tagged with sternal wire and poly-methyl methacrylate mould was used to reconstruct the rib cage and augmented with mesh Post-op reconstruction X-ray Fig-6. Following the surgery on 2 year follow-up patient is disease free and doing well.
Figure 7,8,9,10, 11, 12
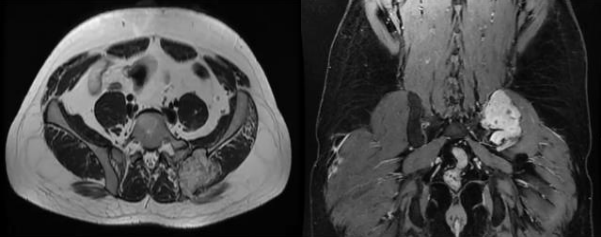
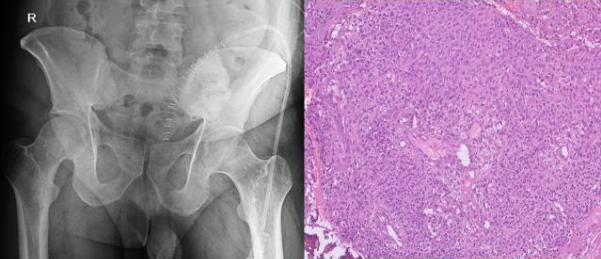
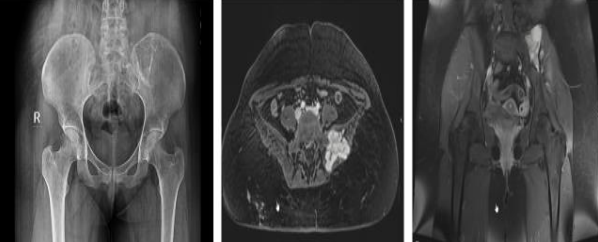
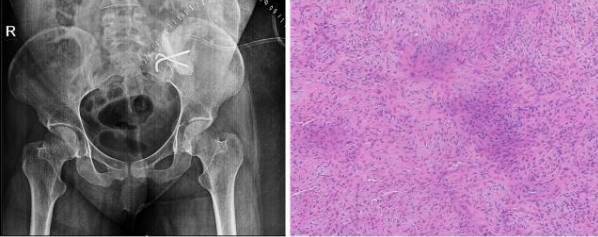
Case 3 - 35 year old male who presented with low back ache since 5 years and swelling since 2 year. Upon evaluation with X-ray of pelvis was found to have a lytic lesion in the left ileum on posterior aspect Fig-7. On MRI T2 hyper-intense lesion was found the posterior ileum with soft tissue component and cortical breech on posterior aspect measuring 5.7x 4.1x 7.3cm Fig-8.. Patient underwent extended curettage of the lesion and reconstruction with Poly-methyl methacrylate cement and Post-op Histopathology showed oval to spindle shaped cells with indistinct cell borders, round to oval hyperchromatic nucleus and moderate amount of cytoplasm- fibromatosis Fig-9. Upon follow up for 3 years patient is disease free.
Case 4- 21 year old female patient who presented with pain and swelling of the left lower back area since 8 months. Upon clinic radiological evaluation – on x ray was found to have a lytic lesion in the left postero-superior iliac wing and MRI showed T2 intermediate to hyper-intense lesion on the left iliac wing with cortical breech and extra-osseous soft tissue component involving the iliacus muscle anteriorly and gluteus medius posteriorly measuring 5.9x5.6x6.3 cm with T2 hypointense rim around the lesion Fig-10. Histopathology proved to be fibromatosis and after multidisciplinary team meeting patient was planned for extended curettage and reconstruction Fig-11. Reconstruction was done using poly-methyl methacrylate cement and two K-wire for stabilisation with post-op Histopathology confirming the diagnosis Fig-12. Upon one year of follow up patient does not have any complaints and doing well.
Discussion
A very uncommon tumour that grows slowly and contains collagen-producing, well-differentiated cells is called a desmoplastic fibroma. It is aggressive locally and has a peak occurrence between the ages of 15 and 25 years, despite being benign in nature. Patients frequently have pain for years at a time, suggesting sluggish progress. A desmoplastic fibroma can occasionally be discovered by accident. Desmoplastic fibromas can affect any bone, however they typically affect the long bones. Despite being regarded as the opposite of fibromatosis of the desmoid type (1). Numerous entities, such as fibrous dysplasia, giant cell tumours, unicameral bone cysts, chondromyxoid fibromas, non-ossifying fibromas, periosteal desmoids, eosinophilic granulomas, low-grade intra-osseous osteosarcomas, adamantinoma, and distant metastases, can radiographically mimic a desmoplastic fibroma. On radiographs, it typically appears as a well-margined osteolytic lesion with a limited transition zone. It could appear bubbly or trabeculated irregularly with cortical thinning. In cases of cortical breach, there may be an extra-osseous soft tissue mass. An intriguing magnetic resonance imaging characteristic of desmoplastic fibroma is the appearance of low to intermediate signal intensity foci on T2-weighted images, which radiographically do not correspond to calcifications, this feature may help narrow the differential diagnosis (7, 8).
The most reliable way to identify the precise type of bone lesion is by a biopsy since it offers a tissue diagnosis.
Correct diagnosis is crucial since, both radiologically and histologically, the lesion might be misdiagnosed as a benign fibrous lesion that is indolent or as a more aggressive spindle-cell sarcoma, with very different treatment options (6). It has been noted that relatively significant recurrence rates occur after basic curettage (9). Wide margin surgical excision is the recommended method of treatment since it has been demonstrated to have the lowest recurrence rates. Large tumours appear to be unsuitable for wide resection and reconstruction because they present a significant reconstructive difficulty. Furthermore, the reconstruction alternatives that are accessible either permanently limit function (e.g., arthrodesis and rotationplasty) or are incredibly expensive (e.g., allograft reconstruction and mega prostheses). These are at many times not acceptable to the patient.
Extended curettage has been widely regarded as a special kind of surgical treatment for bone tumours, and the technique has been refined throughout time. To avoid leaving any tumour cells around the corner next to the near-side cortex, it is recommended to build a cortical window at least as large as the lesion. Using a power burr, the hollow is expanded 1 to 2 cm in all directions after curettage is finished, being careful not to puncture the subchondral bone into the joint. Adjuvants that aid in the destruction of any remaining tumour cells, such as liquid nitrogen, phenol, bone cement, electrocautery, or an argon beam coagulator, are used to prolong the curettage process (10).
In a retrospective analysis, Evans et al. examined 13 patients: 6 had intralesional curettage, 3 had marginal excision, 1 had wide excision and endoprosthetic replacement, and 1 had below-knee amputation. Of these, two patients suffered recurrence and both had received intralesional curettage. Within the first year, both recurrences occurred (11).
Rastogi et al. reported three cases of unusual locations and concluded that intra-lesional curettage can be attempted if resection leads to major functional loss (12). Yokouchi et al. reported no recurrence at 12-year follow up after extended curettage and heat ablation for desmoplastic fibroma of the distal femur (13).
Out of the four patients in our current series, two underwent extended curettage, where the defect was filled with polymethyl methacrylate cement, and the other two underwent wide local excision and reconstruction. One patient underwent a type 3 scapulectomy for treatment of a local recurrence that occurred six years after the index surgery. Desmoplastic fibroma recurrence has been documented to happen often within a year. Although they are rare, late recurrences after many years have been documented, indicating the need for careful monitoring, particularly following a conservative surgical operation (9).
Given the histological similarities between desmoplastic fibroma and soft tissue fibromatosis, radiation therapy may be useful in achieving local control. Two case reports, one in the ilium and one in the distal femur, describe the use of radiation as the main therapeutic option for desmoplastic fibromas. (14, 15).
Conclusion
Desmoplastic fibroma is a locally aggressive tumor, which is usually diagnosed on biopsy. Extended curettage may be more appropriate for large tumors at pelvis and meta-diaphyseal locations where en bloc excision would result in a challenging reconstruction. However, surgical excision with wide margins is the treatment of choice and is appropriate for all small tumors. The role of radiotherapy is not established however, radiotherapy may be important as an adjuvant after conservative surgery such as extended curettage.
Conflict of interest: None.
References
1) Fornasico V, Pritzker KPH, Bridge JA (2002) Desmoplastic fibroma of bone. In: Fletcher CDM, Unni KK, Merten SF (eds) The World Health Organization classification of tumours. Pathology and genetics of tumours of soft tissue and bone. IARC Press, Lyon, p 28.
2) Hauben E, Cleton-Jansen AM. Desmoplastic fibroma of bone. WHO classification of tumors of soft-tissue and bone. Lyon: International Agency for Research on Cancer; 2013; 298.
3) Mirra JM. Desmoid tumours of bone (desmoplastic fibroma or “aggressive fibromatosis”). Bone tumours: clinical, radiological and pathological Correlations, vol. 1. Philadelphia: Lea and Febiger; 1989; 735–47.
4) Hauben EL, Jundt G, Cleton-Jansen AM. Desmoplastic fibroma of bone: an immunohistochemical study including beta-catenin expression and mutational analysis for beta-catenin. Hum Pathol 2005;36:1025–30.
5) Beabout JW. Malignant and borderline malignant fibrogenic tumours of bone. Radiology: diagnosis, imaging, intervention, vol. 5. Philadelphia: JB Lippincott Company; 1988; 1–11.
6) Inwards CY, Unni KK, Beabiut JW, Sim FH. Desmoplastic fibroma of bone. Cancer 1991;68:1978–83.
7)Vanhoenacker FM, Hauben E, De Beuckeleer LH, Willemen D, Van Marck E, De Schepper AM (2000) Desmoplastic fibroma of bone: MRI features. Skelet Radiol 29(3):171–175 http://www.ncbi. nlm.nih.gov/pubmed/10794556
8) Mahnken AH, Nolte-Ernsting CC, Wildberger JE, Wirtz DC, Günther RW (2001) Cross-sectional imaging patterns of desmoplastic fibroma. Eur Radiol 11(7):1105–1110 http://www. ncbi.nlm.nih.gov/pubmed/11471596.
9)Böhm P, Kröber S, Greschniok A, Laniado M, Kaiserling E (1996) Desmoplastic fibroma of the bone. A report of two patients, review of the literature, and therapeutic implications. Cancer 78:1011– 1023
10)Toy PC and Heck RK (2013) General principles of tumors. In: Canale ST, Beaty JH (ed.) Campbells operative orthopaedics. 12th Ed. Elsevier Mosby. pgs.’: 834–36
11)Evans S, Ramasamy A, Jeys L, Grimer R (2014) Desmoplastic fibroma of bone: a rare bone tumour. J Bone Oncol 3:77–79
12)Rastogi S, Varshney MK, Trikha V, Khan SA, Mittal R (2008) Desmoplastic fibroma: a report of three cases at unusual locations. Joint Bone Spine 75:222–225 http://www.ncbi.nlm.nih.gov/ pubmed/17980636.
13)Yokouchi M, Ueno Y, Nagano S, Shimada H, Nakamura S, Setoguchi T, Kawamura I, Ishidou Y, Komiya S (2014 Sep) Extended curettage and heat ablation for desmoplastic fibroma of the distal femur with a 12-year follow-up period: a case report. Oncol Lett 8(3):1103–1106
14) Sanfilippo NJ, Wang GJ, Larner JM (1995) Desmoplastic fibroma: a role for radiotherapy? South Med J 88:1267–1269 http://www. ncbi.nlm.nih.gov/pubmed/7502123
15) Nag HL, Kumar R, Bhan S, Awasthy BS, Julka PK, Ray RR (2003) Radiotherapy for desmoplastic fibroma of bone: a case report. J Orthop Surg 11(1):90–93 http://www.ncbi.nlm.nih.gov/pubmed/ 12810978.