Case Report: 13 Years Old Girl with Lips Pigmentation, Severe Anemia and Hearing Loss, King Abdulaziz Medical City of the National Guard, Saudi Arabia 2018.
Case Report: 13 Years Old Girl with Lips Pigmentation, Severe Anemia and Hearing Loss, King Abdulaziz Medical City of the National Guard, Saudi Arabia 2018.
Dr. Ahmed Moosa Yahya assery*
*Correspondence to: Dr. Ahmed Moosa Yahya assery, Paediatrics ambulatory care consultant. King Abdulaziz Medical City, National Guard Medical Affairs, Family Medicine-Ambulatory care, NGCSC.
Copyright
© 2018: Dr. Ahmed Moosa Yahya assery. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 July 2018
Published: 15 October 2018
Abstract
Dark lips and tongue pigmentation in children usually not exceeds two major -and rare- medical situations which are either Peutz-Jegher syndrome or McCune-Albright syndrome which are both well known to be a collection of a clinical stigmata’s of each recognise them from each other and also from other causes of lips and tongue hyperpigmentation in children, the interesting thing in such case report not only the lip and tongue pigmentation, the attractive thing here first is that the ultimate diagnosis of the case has not established till writhing this report ( neither of the previously mentioned two common causes of the hyperpigmentation) and the second thing the new uncommon association of such dark lips and tongue with severe unexplained anemia and hearing loss, the third point here also in our case is the onset of such manifestations being started in the paediatrics age in contrast to many cases reported with the same scenario that started late of age ,the question here are we dealing with a unknown new syndrome or paediatrics association? Can we also at the same time explain any relations between those findings - the lip darkness, anemia, hearing loss and the early onset patho-physiologically? Or what happened may just be a matter of a coincidence. This my presentation in this paper.
Case Report: 13 Years Old Girl with Lips Pigmentation, Severe Anemia and Hearing Loss, King Abdulaziz Medical City of the National Guard, Saudi Arabia 2018.
Keywords:
KingAbdullAziz Medical City: KAMC.
National Guard Comprehensive Specialized Clinics: NGCSC.
Peutz-Jegher syndrome: PJS.
Peutz-Jegher Polyps: PJP.
Mc-Cune Albright syndrome: MCAS.
Hyperpigmentation: HPGM.
neurofibromatosis: NF.
Anemia: ANM.
Haring loss: HL.
Mucocutaneous pigmented macules: MCPM.
Hamartomatous polyps: HTP.
Auditory-pigmentary disorders: APDs
Neurocristopathies: NCP.
neural crest: NC.
Waardenburg syndrome: WS.
oculocutaneous albinism: OCA.
Tietz syndrome: TS.
piebaldism: PBT.
congenital sensorineural hearing loss: SNHL
Laugier–Hunziker syndrome: LHS
Introduction
PJS: is an autosomal dominant syndrome characterized by multiple hamartomatous polyps in the gastrointestinal tract, mucocutaneous pigmentation, and an increased risk of gastrointestinal and nongastrointestinal cancer.
PJS is rare with an estimated prevalence of 1:8000 to 1:200,000 births. Males and females are equally affected.
Clinically melanin spots are present in more than 95 percent of individuals with PJS and are caused by pigment-laden macrophages in the dermis. They are typically flat, blue grey to brown spots 1 to 5 mm in size. These pigmented macules most commonly occur on the lips and perioral region (94 percent), palms of the hands (74 percent), buccal mucosa (66 percent), and soles of the feet (62 percent) (picture 1) . They may also be seen on the nose, perianal area, and genitals, and rarely in the intestines. Mucocutaneous pigmentation usually occurs during the first one to two years of life, increases in size and number over the ensuing years, and finally fades after puberty with the exception of those on the buccal mucosa. Malignant transformation is extremely rare. Mucocutaneous pigmented macules in individuals with PJS may be confused for ephelides (freckles). However, ephelides are typically sparse near the nostrils and mouth, are absent at birth, and never appear on the buccal mucosa. The mucocutaneous pigmented macules, although sensitive for PJS, are not specific and may be associated with other syndromes.
HTP are present in most patients with PJS. Although polyps most commonly occur in the small bowel (60 to 90 percent) and more specifically in the jejunum, they can be found throughout the gastrointestinal tract including the stomach (15 to 30 percent) and colon (50 to 64 percent). Gastrointestinal polyps develop in the first decade of life and most patients become symptomatic between the ages of 10 and 30. HTP may also occur outside the gastrointestinal tract, including the renal pelvis, urinary bladder, lungs, and nasopharynx. Although 50 percent of patients are asymptomatic at the time of diagnosis, individuals with PJS can present with obstruction caused by intussusception or occlusion of the gastrointestinal lumen by the polyp, abdominal pain caused by infarction, anemia from acute or chronic bleeding, or extrusion of the polyp through the rectum. Up to 69 percent of patients experience an intussusception during their lifetime, most often in the small intestine.
Picture 1: Photograph shows the characteristic circumoral pigmentation in a patient with the PJS. The pigmentation may not be obvious as in this patient, and it should always be sought carefully in young patients presenting with unexplained gastrointestinal bleeding, particularly if there is a family history of such bleeding.
On gastrointestinal endoscopy, the PJP have no major distinguishing features, and may be sessile, pedunculated, or lobulated. The number of polyps ranges from 1 to more than 20 per segment of bowel, although some patients have solitary lesions. The size of the polyps ranges from 0.1 to more than 5 cm in diameter (picture 2). On histology, PJ P are hamartomas that characteristically contain a proliferation of smooth muscle extending into the lamina propria in an arborization-like fashion; the overlying epithelium is normal (picture 3). Epithelial misplacement involving all the layers of the bowel has been reported in approximately 10 percent of small intestinal polyps in PJS. Epithelial misplacement, possibly due to mechanical forces, may extend into the serosa and be misdiagnosed as a well-differentiated adenocarcinoma.
Picture 2: Gross picture of an intestinal polyp (arrow) removed from a patient with the PJS.
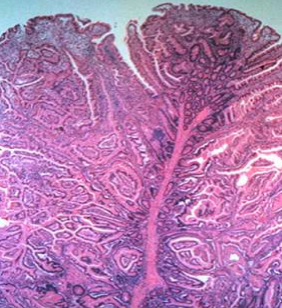
Picture 3: Low power view of a duodenal PJP shows a tree-like proliferation of smooth muscle lined by normal small intestinal epithelium; the overlying epithelium is normal.
Cancer risk — PJS is associated with an increased risk of gastrointestinal and extra-intestinal malignancies. In a systematic review of 20 observational studies which included 1644 patients with PJS, the reported lifetime risk for any cancer varied between 37 and 93 percent. The average age of developing a malignancy was 42 years. The most common sites for malignancy were colorectal, followed by breast, stomach, small bowel, and pancreas.
clinical diagnosis of PJS can be made by the presence of any of the following:
•Two or more PJS-type HTP of the gastrointestinal tract
•Characteristic mucocutaneous hyperpigmentation of the mouth, lips, nose, eyes, genitalia, or fingers in a person with a family history of PJS
•Any number of PJP in an individual with a family history of PJS in a first-degree relative
?Any number of PJP in a person with the characteristic mucocutaneous pigmentation of PJS. (1).
MCAS — is a rare disorder defined as the triad of peripheral precocious puberty, irregular café-au-lait ("coast of Maine") skin pigmentation (picture 4 A&B), and fibrous dysplasia of bone. MCAS should be considered in females with recurrent formation of follicular cysts and cyclic menses. The skin manifestations and bone lesions may increase over time. In females presenting with vaginal bleeding, the ovarian enlargement has often been mistaken for an ovarian tumor, leading to unnecessary oophorectomy. Females presenting with premature vaginal bleeding should therefore be evaluated for features of MCAS to avoid this potential mistake. The clinical phenotype varies markedly, depending on which tissues are affected by the mutation, but precocious puberty is the most commonly reported manifestation. As in other forms of peripheral precocity, the sequence of pubertal progression may be abnormal, in that vaginal bleeding often precedes significant breast development. Prolonged exposure to elevated levels of sex steroids may cause accelerated growth, advanced skeletal maturation, and compromised adult height. Although the precocious puberty is typically peripheral precocity, a secondary component of central precocious puberty may develop because of sex steroid withdrawal leading to activation of the hypothalamic-pituitary-gonadal axis. In males with MCAS, while sexual precocity is less common, there is a high prevalence of testicular pathology on ultrasound, including hyper- and hypoechoic lesions (most likely representing areas of Leydig cell hyperplasia), microlithiasis, and focal calcifications.
café-au-lait spots which are usually present at birth or shortly thereafter, are the most common but unappreciated "presenting" sign. Café-au-lait pigmentation - This consists of spots ranging from light brown to dark brown in colour, often displaying a segmental distribution, and frequently predominating on one side of the body without crossing the midline; these spots must be differentiated from those characteristics of NF. (2).
Picture 4: (A) A typical lesion on the face, chest, and arm of a five-year-old female with McCune-Albright syndrome, which demonstrates jagged "coast of Maine" borders and the tendency for the lesions to both respect the midline and follow the developmental lines of Blaschko (a configuration of skin lesions characterized by arcs on the upper chest, S shapes on the abdomen, and V shapes over the posterior midline, caused by patterns of X-chromosome inactivation).
(B) Typical lesions that are often found on the nape and crease of the buttocks are shown (arrows).
Our Case Presentation:
This is 13 years old girl who presented to my clinic in the late of late of May 2018 complaining of general fatigue and malaise and among the physical examination we noticed her striking lips dark pigmentations (Picture 5) that not found anywhere her parts of the body, the family denied any member who is relative to them having the same finding. The family denied any start of the menstruation in the girl or any picture of blood loss with any family history of bleeding tendency.
Picture 5: this is the 13 years old girl who is our case report, and you can note the tongue and some lips HPGM,
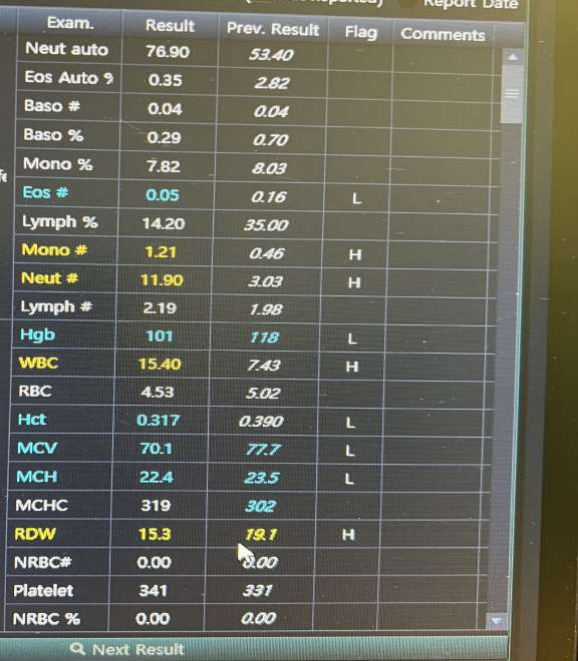
The patient sent for some routine blood works including CBC, ovarian ultrasound and general body skeletal survey that came all normal except the significant anemia (Picture 6) the patient was suffering from despite of the negative stool occult blood and urine analysis.
Picture 6: The complete blood count done for the patient that showing the microcytic hypochromic anemia.
I decided to take the opinion of other paediatrics subspecialties starting by the paediatrics dermatology, gastroenterology, and neurology.
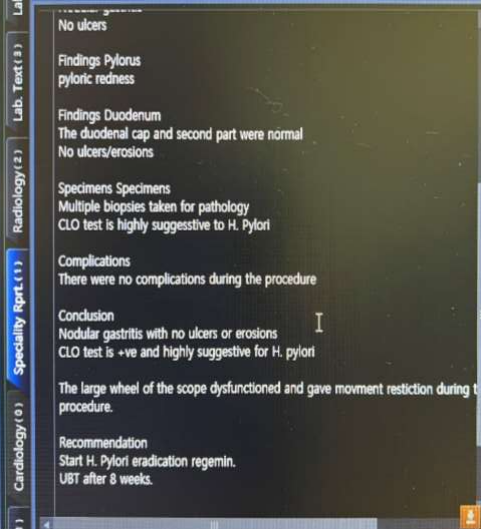
The sequence of the patient management started by me when I treated the anemia by iron supplement then the gastroenterology decided to do endoscopy that came free of any polyps or hamartomas the steps by which we rolled out both PJS and MCAS (picture 7).
Picture 7: This is the Endoscopy repot done by the gastroenterology team.
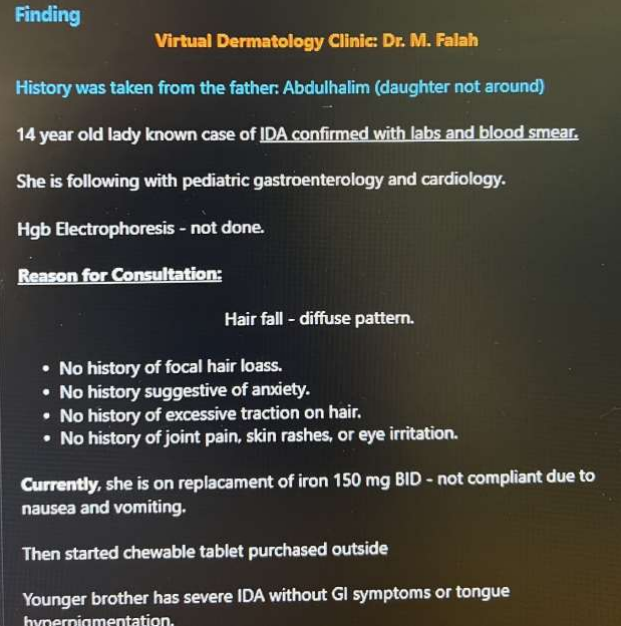
The dermatology after such findings lobed the final diagnosis as lips HPGM of unknown origin (picture 8).
Picture 8: This the final dermatology team report who categorized the case as a tongue HPGM of unknown origin.
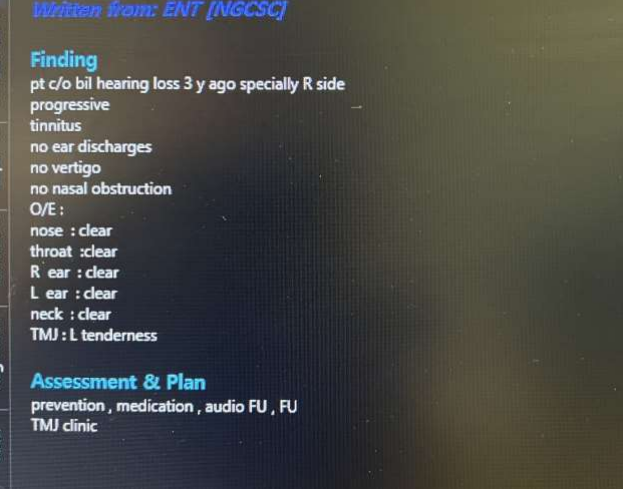
The paediatrics neurology team among their management found an element of hearing loss with patient so they done for her an audio barograph that came highly suggestive of bilateral hearing loss (picture 9).
Picture 9: The final ABR report showing the bilateral hearing loss of the case.
The patient also seen by the ophthalmology team that reported normal findings in the cornea, sclera, and retina.
Ultimately the patient sent to for further genetics counselling, but the family refused going to appointment for a private reason that we don’t know.
The Case Report Discussion
As you saw from then previous narration the patients’ findings were not compatible with any of the two major differential diagnosis of the lip HPGM, PJS and MCAS not only that the attractive thing here that we are dealing with a query new medical problem that has not been discovered yet and may be having its own clinical stigmata which are the lip and tongue HPGM, HL and unexplained anemia.
Among the midline searches about the most famous studies related the skin HPGM and the risk of the hearing loss i could only collect such articles here which most of them done on the adults’ individuals not in the paediatrics.
In the national library of medicine ( J Cutan Aesthet Surg. Published on 2011 Jan-Apr; 4(1): 58–60.doi: 10.4103/0974-2077.79199) a rare adult syndrome called LHS is an idiopathic macular hyperpigmentation of skin characterized by brownish black spots on oral mucosa including lips associated with longitudinal melanonychia of nails. Extended mucocutaneous pigmentation has been seen in few cases on the neck, thorax, abdomen, dorsal and lateral aspects of the fingers, palms and soles, and the perineum (picture 10). No associated HL or anemia in such case report. (3).
Picture 10: A rare adult syndrome called LHS of an elderly female with clear buccal mucosa HPGM.
Here is very interesting topic about the HPGM in paediatrics especially it is so close to our case report I am talking about now, here it says that Congenital sensorineural hearing loss may occur in association with inborn pigmentary defects of the iris, hair, and skin. These conditions, named APDs, represent extremely heterogeneous hereditary diseases, including Waardenburg syndromes, oculocutaneous albinism, Tietz syndrome, and PBT. APDs are part of the neurocristopathies, a group of congenital multisystem disorders caused by an altered development of the neural crest cells, multipotent progenitors of a wide variety of different lineages, including those differentiating into peripheral nervous system glial cells and melanocytes. We report on clinical and genetic findings of two monozygotic twins from a large Albanian family who showed a complex phenotype featured by sensorineural congenital deafness, severe neuropsychiatric impairment, and inborn pigmentary defects of hair and skin. The genetic analyzes identified, in both probands, an unreported co-occurrence of a new heterozygous germline pathogenic variant (c.2484 + 5G > T splicing mutation) in the KIT gene, consistent with the diagnosis of PBT, and a heterozygous deletion at chromosome 15q13.3, responsible for the neuropsychiatric impairment. This case represents the first worldwide report of dual locus inherited syndrome in piebald patients affected by a complex auditory-pigmentary multisystem phenotype. Here we also synthesize the clinical and genetic findings of all known neurocristopathies characterized by a hypopigmentary congenital disorder.
NCP represent a complex group of inborn conditions associated with a wide range of multiorgan congenital diseases determined by an aberration in growth, migration, and differentiation of NC cells. NC is a transient, multipotent cell population that generates a broad spectrum of numerous cell types, including melanocytes of the skin and hair follicles, neurons, and glial cells. As a result, patients with NCP develop an extensive range of multisystem abnormalities such as skin and hair pigmentation defects, neurological and ocular disorders. Among NCP, Hirschsprung, DiGeorge, Treacher-Collins, CHARGE, Axenfeld-Rieger, and Goldenhar syndromes are mainly featured by cardiac, auditory, eye, neurological, urinary, craniofacial defects, and/or missing enteric ganglia.WS, OCA, TS and PBT represent a subgroup of NCP, termed APDs. All APDs are clinically characterized by inborn skin and hair pigmentary anomalies. They can also be associated with a wide and heterogeneous spectrum of auditory, neurological, and ocular disorders. Precisely, SNHL is a very common feature in WS and TS patients; conversely, it has been described more rarely in PBT and OCA subjects. synthesizes the clinical and genetic findings of all known neural crest–associated diseases characterized by hypopigmentary congenital disorders. (4).as you noticed here in the last paragraphs that were talking about something near to our case but the difference here is the hypopigmentation element associating the cases mentioned not the hyperpigmentation one we have here.
In another place of the national library of medicine (Am J Epidemiol. 2017 Jul 1; 186(1): 1–10. Published online 2017 May 19. doi: 10.1093/aje/kwx024 ) showed that black individuals have a lower risk of hearing loss than do whites, possibly because of differences in cochlear melanocytes. Previous studies have suggested that darker-skinned individuals tend to have more inner ear melanin, and cochlear melanocytes are important in generating the endocochlear potential. Here in such study no particular and specific pointing to the lips or other body HPGM lesions but it talks about the global skin colour (white and black) which is finally related to a racial aspect the things we can’t elaborate it deeply with any patient in our culture of Saudi Arabia being a sensitive topic. (5).
Conclusion
A triad of buccal cavity dark hyperpigmentation (not hypopigmentation), unexplained anemia and profound hearing loss with onset in paediatrics age could be a new neurocutaneous disorder to be furtherly investigated in the futures days.
References
1_https://www.uptodate.com/contents/peutz-jeghers-syndrome-clinical-manifestations-diagnosis-and-management?source=history_widget
2_https://www.uptodate.com/contents/definition-etiology-and-evaluation-of-precocious-puberty?source=history_widget#H3989453
3_https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3081490/
4_https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6681376/
5_https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5860009/