Rare Localization of Osteoid Osteoma: Case Report and Review of the Literature.
Rare Localization of Osteoid Osteoma: Case Report and Review of the Literature.
Dr.Cherni Hamza *
*Correspondence to: Dr. Cherni Hamza, orthopedic consultant SALAMAT hospital (Hail, KSA).
Copyright
© 2024 Dr. Cherni Hamza. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 February 2024
Published: 01 March 2024
DOI: https://doi.org/10.5281/zenodo.10727190
Rare Localization of Osteoid Osteoma: Case Report and Review of the Literature.
Introduction
Osteoid osteoma is a benign osteoblastic tumor frequently found in the cortex of long bones (femur and tibia). Its located in the fingers and toes is very rare. It accounts around 10% of all primary bone tumors.
Classically, the most frequent clinical form is nocturnal pain, which disappears with the use of non-steroidal anti-inflammatory drugs (aspirin test).
A characteristic radiographic appearance of the tumor, when present, points to the diagnosis (nidus-like appearance surrounded by sclerosis), which is confirmed histologically.
The presence of osteoid osteoma in the phalanges of the toes is very likely to happen, and therefore a misdiagnosis is very likely.
The presence of local inflammatory signs (swelling and redness) raises the possibility of other diagnoses (infectious, metabolic, rheumatic...) as well as the cortical location of the nidus.
In this article, we present a case of osteoid osteoma in the distal phalanx of the big toe.
Keywords: osteoid osteoma, phalanx, foot.
Clinical Case
A 23-year-old woman presents with nocturnal pain of the right big toe, with persistent swelling, which has been present for a year and a half. Mistaken for an ingrown toenail, she underwent two operations with no improvement.
Clinical examination revealed pain at the base of the second phalanx of the big toe and localized edema. A positive aspirin test was performed.
Figure 1: A radiographic work-up included an X-ray of the big toe, which was found to be normal despite the presence of a non-specific condensation at the base of distal phalanx.
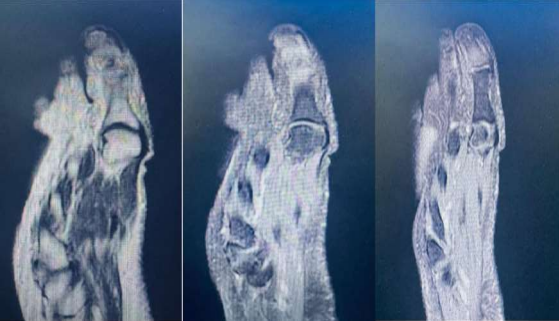
Figure 2: An MRI was requested, showing a hyper-signal at the base of distal phalanx of the big toe.
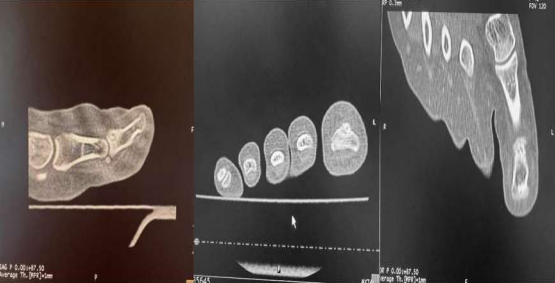
Figure 3: A CT scan showed the nidus surrounded by sclerosis.
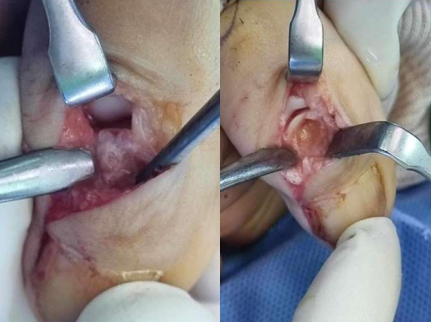
Figure 4: The patient underwent surgery. Excision of the bone tumor.
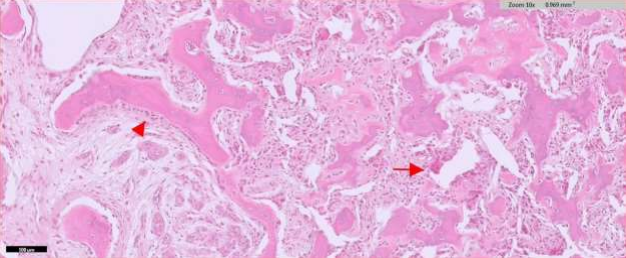
Figure 5: Histopathologic study confirm the diagnosis
Discussion
Osteoid osteoma is a benign primary bone tumor occurring in approximately 10% of cases. It is mainly seen in the cortices of long bones (femur and tibia) (1).
In our case, it’s located in the distal phalanx of the toe which is very rare to happen according to the literature (2).
Epidemiologically, a higher incidence among males was consistently observed, with a predominance in the 20-30 age range (3).
Clinically, it presents as nocturnal pain that is relieved by anti-inflammatory medication.
When it is seen in the toes, swelling (macrodactyly) is associated in 86% of cases (3), with inflammatory signs (redness and local heat) in 30% of cases (3), which can mislead the diagnosis. Differential diagnoses are often infectious (osteomyelitis) or paronychia.
Standard radiographic findings show the size of the tumor it could be normal sometimes. Bone lysis may be absent at first.
MRI aids diagnosis by showing bone marrow edema in the form of a hyper signal. Misdiagnosis occurs in 1/3 of cases (3).
CT is the technique of choice, with a sensitivity of 96-100% (3), and enables us to visualize the tumor in its pathognomonic form.
Despite a typical anamnesis and simple clinical features that point to the diagnosis, an average delay of 12 months has been found in the literature between the appearance of signs and the establishment of the diagnosis (3). In our case, the delay was 18 months.
The treatment of choice is surgery, which allows both complete excision and rectification of the diagnosis in the event of infection or other factors.
The use of radiofrequency is sometimes difficult, given the risk of damage to the nail apparatus, skin necrosis and damage to adjacent vascular and nerve structures [4].
Reference
[1] ANGEL CASTILLO-FORTUÑO, Osteoid Osteoma of the Toe: A Rare Presentation with Diagnostic Challenges, Journal of the Belgian Society of Radiology. 2023; 107(1): 64, 1–4. https://doi.org/10.5334/jbsr.3250.
[2] Hakan BaGar, Osteoid Osteoma of Distal Phalanx of Toe: A Rare Cause of Foot Pain, Case Reports in Orthopedics Volume 2014, Article ID 560892, 4 pages http://dx.doi.org/10.1155/2014/560892
[3] Ruth thieman, difficult diagnosis of osteoid osteoma of the big toe orthopedist 2021. Orthopade 2021 50:689–699 https://doi.org/10.1007/s00132-021-04082-z
[4] Giampaolo Bianchi, Interventional Radiology’s Osteoid Osteoma Management: Percutaneous Thermal Ablation, J. Clin. Med. 2022, 11, 723. https://doi.org/10.3390/jcm11030723.