Diabetic Striatopathy: Case Report and Literature Review
Diabetic Striatopathy: Case Report and Literature Review
Quintanilla C*1,Sánchez M1, Otazú M 1, Saccone S 1
1. Clínica de Endocrinología y Metabolismo. Prof. Dra Beatriz Mendoza, Hospital de Clínicas, Dr. Manuel Quintela.
*Correspondence to: Quintanilla C., Clínica de Endocrinología y Metabolismo. Prof. Dra Beatriz Mendoza, Hospital de Clínicas, Dr. Manuel Quintela.
Copyright
© 2024 Quintanilla C. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 March 2024
Published: 01 April 2024
Abstract
Diabetic Striatopathy (DS), also known as non-ketotic hyperglycemic hemichorea/hemiballism, is defined as a clinical-radiological syndrome characterized by chorea-ballism, hyperglycemia, and increased signal intensity in the striatum on Computed Tomography (CT) or Magnetic Resonance Imaging (MRI). It is a rare and underdiagnosed complication of diabetes, with an estimated prevalence of 1 case per 100,000 inhabitants, with a predominance in females.
Case Report: A 59-year-old woman with a history of hypertension and smoking presented with abnormal involuntary movements of the right hemibody for 14 days. CT scan showed alterations consistent with metabolic encephalopathy. She was diagnosed with mellitus diabetes. MRI revealed alterations in the left basal ganglia consistent with non-ketotic hyperglycemic hemichorea. Insulin therapy was initiated along with symptomatic treatment, resulting in complete resolution of symptoms.
Discussion: DS clinically presents as hemichorea, defined as involuntary, random, low-amplitude movements predominantly affecting the distal extremities of one hemibody. Characteristic neuroimaging findings include hyperdensity of the striatum on CT and hyperintensity on T1-weighted MRI, typically contralateral to the chorea.
Conclusions: The hallmark of DS is the presence of hyperglycemia concurrent with typical clinical and imaging manifestations. However, the main differential diagnosis is cerebral vascular pathology. DS is a very rare complication of diabetes mellitus, but with a high index of suspicion and prompt treatment, long-term repercussions can be avoided.
Keywords: diabetic striatopathy, chorea, hemiballism.
Diabetic Striatopathy: Case Report and Literature Review
Introduction
Diabetes mellitus (DM) is a multifactorial metabolic disorder characterized by chronic hyperglycemia resulting from a defect in insulin secretion and/or action, and it is associated with alterations in the metabolism of carbohydrates, fats, and proteins (1). Its prevalence is on the rise, with an estimated 422 million people worldwide and 62 million in the Americas suffering from this condition (2).
Diabetic striatopathy (DS) is defined as a state of hyperglycemia presenting with chorea-ballism and/or increased signal intensity in the striatum on imaging, either as hyperdensity on computed tomography (CT) or hyperintensity on T1-weighted magnetic resonance imaging (MRI) of the skull (3).
This clinical-radiological syndrome is a very rare complication of DM, with an estimated prevalence of 1/100,000 patients, which may contribute to its underdiagnosis. Clinically, it manifests as hemichorea or as acute onset generalized chorea, and it is more common in elderly women with type 2 diabetes mellitus (T2DM) and non-ketotic hyperosmolar hyperglycemic state (4).
The aim of this work is to describe a clinical case of this rare condition, which presented in the emergency department of “Hospital de Clínicas, Dr. Manuel Quintela”, in the year 2023.
Case Report
Female patient, 59 years old, with a family history of type 2 diabetes mellitus (DM2) in her mother, and personal history of mild smoking and controlled hypertension with treatment, without evidence of end-organ damage.
The patient presents to the emergency department with sudden, involuntary, purposeless movements affecting the right half of her body for the past 14 days. These movements are random, involving both proximal and distal areas. There are no signs of focal neurological deficit or increased intracranial pressure. There is no evidence of early diabetic syndrome, autoimmune diseases, or sexually transmitted diseases in her medical history.
Upon physical examination, the patient is alert, oriented to time and space, and demonstrates intact cranial nerves. There are choreo-ballistic movements observed in the right upper limb and right lower limb. Osteotendinous reflexes reveal hyporeflexia in the right upper limb and hypotonia in the right limbs. Sensation and coordination are normal. Given the presentation of right hemichorea and to further elucidate the etiology, the patient is admitted for further evaluation.
From the laboratory tests, it is notable that the fasting blood glucose level is 252 mg/dL, and in a subsequent sample, it rises to 353 mg/dL (reference range: 70-100 mg/dL). The glycated hemoglobin (HbA1c) level is 11%, indicating poor glycemic control. Ketone levels are negative. A diagnosis of diabetic debut is established.
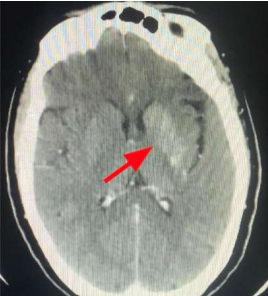
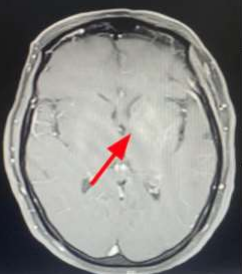
The cranial CT scan reveals a supratentorial intra-axial lesion adjacent to the left lateral ventricle body. It appears spontaneously hyperdense, rounded, well-defined, with heterogeneous enhancement after contrast administration. The lesion measures 11 x 9 mm and is associated with cortical veins draining into the deep collector vein. There is hyperdensity of the basal ganglia, more pronounced on the left, consistent with toxic/metabolic encephalopathy. Subsequently, a cranial MRI is performed, which indicates findings consistent with a left periventricular cavernoma. There are no signs of current complications, with an associated venous anomaly of development. Hyperintensity on T1-weighted images is observed at the head of the left caudate nucleus and lentiform nucleus, which do not enhance with gadolinium. These alterations in the left basal ganglia are compatible with non-ketotic hyperglycemic hemichorea.
Figure 1: Cranial CT scan showing hyperdensity of the left basal ganglia
Figure 2: Cranial MRI showing hyperintensity on T1-weighted images at the level of the head of the left caudate nucleus and lentiform nucleus, which do not enhance with gadolinium
With the diagnosis of diabetic striatopathy, the patient is admitted to the neurology ward and started on symptomatic treatment with tiapride and haloperidol. For metabolic control, a basal-bolus-correction insulin regimen is initiated with NPH insulin and regular insulin. Subsequently, metformin 850 mg is gradually added to lunch and dinner, resulting in significant improvement in metabolic control. During treatment, there is complete resolution of choreic movements. Given the excellent clinical response to the instituted treatment, the patient is discharged and scheduled for outpatient follow-up with endocrinology and neurology.
Discussion
DS is a rare cause of involuntary movements, often presenting as the initial manifestation of DM. It primarily affects adults and manifests as a triad comprising hemichorea-hemiballism, hyperglycemia, and increased signal intensity in the striatum on imaging studies such as CT and/or MRI of the brain, with MRI being the preferred modality (5).
Ballism and chorea represent a spectrum of hyperkinetic involuntary movement disorders. Chorea manifests as continuous, abrupt, rapid, brief, and irregular involuntary movements. When these movements are more severe, they are termed ballism. The term hemichorea-hemiballism is used for hyperkinetic involuntary movement disorders that affect one side of the body with an acute or subacute onset (6).
The pathophysiology of DS is not yet fully understood. Proposed mechanisms include increased blood viscosity due to hyperglycemia, leading to disruption of the blood-brain barrier, which increases the sensitivity of dopaminergic receptors in the postmenopausal period, thus explaining the higher prevalence in women. Additionally, there is a decrease in gamma-aminobutyric acid (GABA) in the striatum, secondary to the non-ketotic state (7).
Souvik Dubey et al. propose a sinister octet that includes the accumulation of gametocytes related to ischemic events leading to petechial hemorrhage, methemoglobin deposits, mineral deposition, cytotoxic edema, osmotic demyelination syndrome, gliosis, and atrophy. It is yet to be elucidated whether these events act interrelatedly or separately (8).
On the other hand, it is proposed that chorea may appear during episodes of hypoglycemia or when metabolic control is achieved, indicating that prolonged periods of hyperglycemia cause lesions in the striatum. This leads to the proposal that metabolic dysregulation alters the blood-brain barrier and leads to insufficient blood supply, resulting in acidosis and edema in the basal ganglia, which in turn generates choreic movements (9).
DS occurs in patients with poorly controlled metabolic status. In up to one-sixth of cases, it manifests in individuals without a prior diagnosis of DM, suggesting that it may be the first manifestation of DM, as in our case (3).
It has also been reported that diabetic striatopathy can develop weeks after the hyperglycemic event (10).
DS predominantly occurs in patients with type 2 diabetes mellitus, although cases have been described in individuals with type 1 diabetes mellitus (DM1) as well. Poor metabolic control is the primary determinant, with observed HbA1c levels reaching up to 18.9%. The average blood glucose levels at presentation are around 400 mg/dL, with corresponding HbA1c levels of approximately 14% (3, 4, 11, 12).
The treatment of DS is primarily based on controlling hyperglycemia and ensuring proper hydration; however, most cases require symptomatic anti-choreic treatment. Typically, antipsychotic drugs, dopamine antagonists, benzodiazepines, anticonvulsants, and selective serotonin reuptake inhibitors are employed. Haloperidol is the most used in monotherapy, followed by tetrabenazine, risperidone, and clonazepam (13).
In a large-scale study, it was observed that less than half of the patients managed to control the chorea solely with hyperglycemia treatment; the rest required symptomatic treatment (14).
The prognosis of DS is strongly associated with the severity of symptoms at diagnosis and secondarily with the time between symptom onset and treatment initiation; however, an early diagnosis and treatment result in better outcomes (15).
The time for chorea correction once glycemic control is initiated can range from 1 hour to 10 days. Other literature suggests a longer interval, ranging from a few days to 10 months, with an average of 6 months for complete correction (13, 16).
Nevertheless, imaging findings on CT and MRI may take between 3 to 8 months, respectively, for complete resolution. Few individuals persist with lesions on neuroimaging. Resolution of both movements and neuroimaging findings has been reported within a period of 2-12 months without distinguishing between them (8, 17).
Conclusions
Diabetic striatopathy is a very rare complication of DM that should be suspected in individuals with poorly controlled blood sugar levels and acute onset of movement disorders. Due to being an underdiagnosed condition, it is crucial to maintain a high level of clinical suspicion to initiate early and timely treatment in order to prevent long-term repercussions. Both clinical and imaging findings are reversible with an excellent prognosis if the cause is correctly identified, and good and consistent glycemic control is achieved.
References
5. Bekiesi?ska-Figatowska M, Romaniuk-Doroszewska A, Banaszek M, Kuczy?ska-Zardzewia?y A. Lesions in basal ganglia in a patient with involuntary movements as a first sign of diabetes - case report and review of the literature. Pol J Radiol. 2010;75(3):61–4.
10. Chiu-Jung Lin MD a PH. Delayed onset diabetic striatopathy: Hemichorea-hemiballism one month after a hyperglycemic episode Author links open overlay panel. The American Journal of Emergency Medicine Volume 35, Issue 7, July 2017, Pages 1036.e3-1036.e4. el 23 de junio de 2017;
11. Yoshinori Abe , Teiji Yamamoto , Tomoko Soeda. Tetsuya Ishihara. Enfermedad diabética del cuerpo estriado: presentación clínica, neuroimagen y patología. Intern Med. 2009;48(13):1135-41. https://doi.org/10.2169/internalmedicine.48.1996
12. Oh S-H, Lee K-Y, Im J-H, Lee M-S. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci [Internet]. 2002;200(1–2):57–62. Disponible en: http://dx.doi.org/10.1016/s0022-510x(02)00133-8
14. Elisabeth B. Lucassen, William T. Delfyett, Mark C. Stahl; Persistent Hemichorea and Caudate Atrophy in Untreated Diabetic Striatopathy: A Case Report. Case Rep Neurol 9 July 2018; 9 (3): 299–303. https://doi.org/10.1159/000484201
15. Alkhaja OY, Alsetrawi A, AlTaei T, Taleb M. Diabetic striatopathy unusual presentation with ischemic stroke-A case report and literature review. Radiol Case Rep [Internet]. 2023;18(6):2297–302. Disponible en: http://dx.doi.org/10.1016/j.radcr.2023.03.031
16. Homaida M , Kanodia AK , Young N , et al. Estriatopatía diabética: una condición rara y un dilema diagnóstico Informes de casos de BMJ CP 2021; 14: e240141.
17. Machado V, Alves L, Torres K, da Silva A. Hemicoreia-hemibalismo secundário a estado hiperglicêmico não cetótico: relato de caso. Brazilian Journal of Health Review. junio 2023. DOI:10.34119/bjhrv6n3-268.