Belting Suture for Optic Zone Combined with Stitched Sutures for Paracentral Corneal Injury: Case Report
Belting Suture for Optic Zone Combined with Stitched Sutures for Paracentral Corneal Injury: Case Report
Asatur Hovsepyan, MD*1
*Correspondence to: Asatur Hovsepyan, MD. Chief Surgeon at the Mobile Eye Hospital (MEH) and Regional Eye Centres (RECs) of the Armenian Eyecare Project (AECP), Armenia.
Copyright
© 2024 Asatur Hovsepyan, MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 March 2024
Published: 01 April 2024
Abstract
The study focuses on the effectiveness of a combination of stitched suture and belting suture, along with wearing a soft contact lens during the early post-op period, for corneal wound adaptation without optical zone damage caused by needle trace-opacifications and fast spherical reshaping of the corneal scar. A 26-year-old male was injured by a pebble and had a visual acuity of 20/200, pH 20/100, and IOP T-1 (palpatory). The wound repair surgery involved a routine stitched-suturing technique for all edges of the wound, except for the one adjacent to the optical zone, which required a tension force directed to the center of the cornea and the one belting suture was placed for that direction. A gas-permeable soft contact lens was then attached to the patient's eye to reduce postoperative pain and improve visual acuity. Over several months, the scar formation progressed to a geometrically nearly spherical shape of the cornea, and the optical zone remained clear due to the belting suture. In April 2023, the VA=20/40 reached a week after suture removal. The combination of stitched-suturing and belting suturing techniques for corneal wound repair, combined with wearing a soft gas-permeable contact lens, allows for corneal spherical shape restoration with less opacification within the optical axis, promoting good patient rehabilitation after deforming penetrating cornea injuries.
Belting Suture for Optic Zone Combined with Stitched Sutures for Paracentral Corneal Injury: Case Report
Introduction
Penetrating injuries of the eyeglobe, especially of the central zone of the cornea require an accurate suturing of the wound to regain spherical shape and transparency of the cornea with achieving hermetic wound closure. Historically all surgeons must design an own plan with existed only two types of sutures as a tool:1) a simply stitched (single, X-shaped double or continious for linear wounds) and 2) a concentric pursue-string sutures. Both are making problems as close as they placed to the optical axis of the cornea due to needle-passings' opacifications and deformation of the spherical shape of cornea.
Presented clinical case proves benefits of the belting suture technique to achieving a best anatomical and functional rehabilitation of the cornea. The using of such sutures allowed to seal optic zone wounds of cornea without trace-opacifications and irregular astigmatism formation due to needle passings. The study aims to present the efficacy of combining stitched suture with belting suture and wearing a soft contact lens during the early post-op period for corneal wound adaptation without optical zone iatrogenous damage and fast spherical reshaping of the corneal scar.
Case Study
26 y.o. male asked in 22.06.2022 for medical help to MEH several hours after right eye injury caused by a pebble flying off from a lawn mower.
VA was 20/200 pH 20/100, IOP T-1 (palpatory). An oblique deforming penetrating wound revealed in the inferior-temporal paracentral zone of the right eye cornea. There was no active bleeding in the eye, pupillary shape was normal. There was an aqueous humor leakage in time of blinking. The lens and the vitreous were clear. There was a mild contusion macular edema.
The wound repair surgery performed: ? routine stitched-suturing technique was used for all edges of the wound with the exception of the one adjacent to the optical zone which required the tension force directed to the center of the cornea. The one belting suture was placed for that direction, and finally a gas-permeable soft contact lens attached to the patient's eye to reduce postoperative pain and some improvement of VA.
The eye was injured by flying a pebble in the time of grass mowing. Fig 1
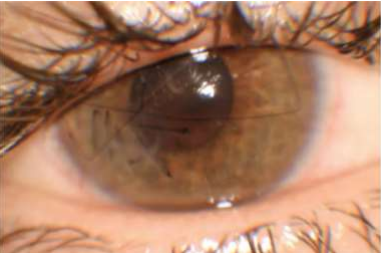
VA WAS 0.1 (20/200) PH 0.2 (20/100), IOP T-1. An oblique deforming penetrating wound revealed in the inferior temporal paracentral zone of the right eye cornea. Fig 2
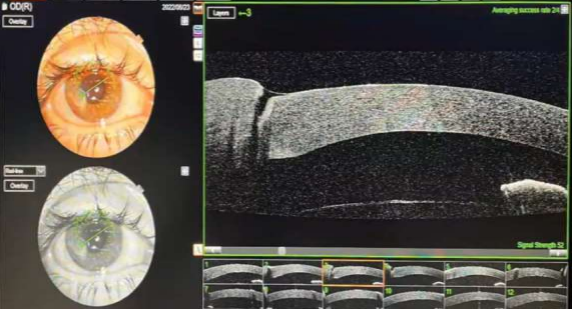
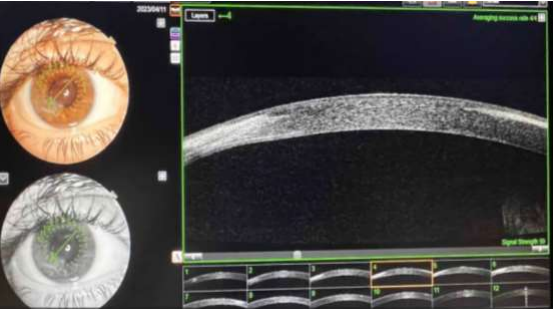
The OCT data of the 8:00 Meridian of Cornea Fig 3
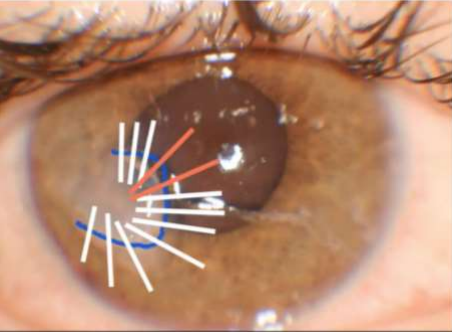
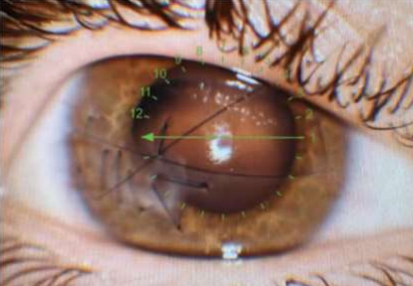
The traditional suturing plan for repairing wound. Fig 4
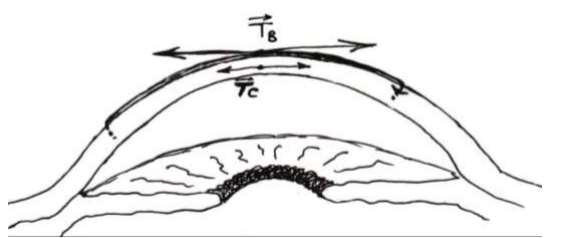
Harmful to optic zone 2 stitched sutures marked in red were replaced with the one belting suture. Fig 5
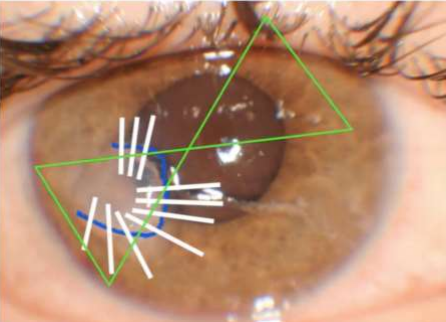
Tangential forces of suture make a pressing effect in the stroma. Fig 6
Results
In several months the scar formation was going with geometrically nearly spherical shape of cornea, and moreover, the optical zone was remaining clear thanks to the belting suture which allowed to keep optical zone of the cornea free of trace opacifications caused by suturing needle. Finally, in April 2023 the VA=20/40 reached a week after suture removal.
20 days after the trauma, note that the patient was with soft contact lens Fig 7
20 days after the trauma OCT data with the soft contact lens Fig 8
2 Months after the trauma, the photo was taken without the soft contact lens. Fig 9
10 Months after trauma (sutures removed 2 months earlier), final OCT Data Note that the VA=0.5 (20/40) Fig 10
Please click here to view all figures
And finally, now (about 15 months after trauma) patient visited local optician and declares that he can see the seventh row (i.e. VA=0.7 (20/30))!!
Conclusion
The using of the combination of routine stitched-suturing technique with the belting suturing technique for optical zone in corneal wound repair with final wearing of soft gas-permeable contact lens help surgeons to reach the cornea's spherical shape restoration with less opacification within the optical axis, and finally good patient rehabilitation after deforming penetrating injuries of cornea, there is no need for special instruments.
References
1. Q, Tang J, Han Y, Xiao Q, Deng Y. Brittle cornea syndrome:A case report and review of the literature. BMC Ophthalmology. 2018;18:252. [PMC free article] [PubMed] [Google Scholar]
2. Walkden A, Burkitt Wright EM, Au L. Brittle cornea syndrome:Current perspectives. Clinical Ophthalmology. 2019;13:1511–6. [PMC free article] [PubMed] [Google Scholar]
3. Natarajan R, Shah GY, Rao SK, Padamanabhan P. Penetrating keratoplasty as a globe-saving procedure in fragile cornea. Cornea. 2003;22:164–5. [PubMed] [Google Scholar]
4. Joshi SA, Uppapalli S, More P, Deshpande M. Unusual case of globe perforation:The brittle cornea without systemic manifestations. BMJ Case Rep. 2016:1–4. doi:10.1136/bcr-2016-215722. [PMC free article] [PubMed] [Google Scholar]
5. Avgitidou G, Siebelmann S, Bachmann B, Kohlhase J, Heindl LM, Cursiefen C. Brittle cornea syndrome:Case report with novel mutation in the PRDM5 gene and review of the literature. Case Rep Ophthalmol Med. 2015:637084. doi:10.1155/2015/637084. [PMC free article] [PubMed] [Google Scholar]
6. Burkitt Wright EM, Porter LF, Spencer HL. Brittle cornea syndrome:Recognition, molecular diagnosis and management. Orphanet J Rare Dis. 2013;8:68. [PMC free article] [PubMed] [Google Scholar]
7. Hussin HM, Biswas S, Majid M, Haynes R, Tole D. A novel technique to treat traumatic corneal perforation in a case of presumed brittle cornea syndrome. Br J Ophthalmol. 2007;91:399. [PMC free article] [PubMed] [Google Scholar]
8. Ramappa M, Wilson ME, Rogers RC, Trivedi RH. Brittle cornea syndrome:A case report and comparison with Ehlers Danlos syndrome. J AAPOS. 2014;18:509–11. [PubMed] [Google Scholar]
9. Izquierdo L, Jr, Mannis MJ, Marsh PB, Yang SP, McCarthy JM. Bilateral spontaneous corneal rupture in brittle cornea syndrome:Acase report. Cornea. 1999;18:621–4. [PubMed] [Google Scholar]
10. Srirampur A, Agrawal SK, Pesala V. Brittle cornea syndrome:Current perspectives [Letter] Clin Ophthalmol. 2019;13:1719–20. doi:10.2147/OPTH.S227147. [PMC free article] [PubMed] [Google Scholar].