Comparative Study of Early Neonatal Morbidities in Late Preterm Versus Term Neonates
Comparative Study of Early Neonatal Morbidities in Late Preterm Versus Term Neonates
Dr Vaishakh *1, Dr Sachin Padman 2
1. Dr Vaishakh VP junior Consultant Paediatrics Sunrise Hospital Kanhangad.
2. Dr Sachin Padman Director Paediatrics and Neonatology Sunrise Hospital Kanhangad.
*Correspondence to: Dr Vaishakh VP junior Consultant Paediatrics Sunrise Hospital Kanhangad.
Copyright
© 2024: Dr Vaishakh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 March 2024
Published: 01 April 2024
Abstract
This study aimed to evaluate the morbidity and mortality patterns among late preterm neonates, specifically those born before 37 weeks of gestation. The neonatal era accounts for a higher percentage of mortality in children under five, with preterm births being a major cause of many deaths. The study was a prospective observational cohort study conducted in the Neonatal Intensive Care Unit, Department of Pediatrics, at DDU Hospital, New Delhi.
The mean gestation distribution among late preterm infants was 35.39 weeks, while term neonates were 38.64 weeks. The mean birth weight distribution was 2.35 (±0.48) and 3.04 (±0.43) kgs. Males were commonly encountered in both study groups.
The study found that there was a significant difference in the distribution of hypoglycemia across the study groups, with late preterm infants accounting for more cases. There was also a significant difference in the incidence of post resuscitation care, with late preterm infants requiring more care.
Respiratory distress incidence was higher in late preterm infants, with a statistically significant increase. In cases of jaundice and sepsis, late preterm infants had more incidences than the other group.
Comparative Study of Early Neonatal Morbidities in Late Preterm Versus Term Neonates
Introduction
Infants born before 37 weeks of gestation are referred to as preterm by the WHO.(1) The National institute of child health and human development has defined and labelled a newer terminology namely the “late preterm” to those infants who are born between the 34th and 36th weeks of gestation. This terminology was earlier referred to as near term infants before (2). The term “Late preterm neonates” are defined as born at 340/7 to (36+6) weeks of gestational age. Whereas, a term neonate has been defined as those born between 370/7 weeks of gestation through 4/6/7 weeks of gestation (3,4).
Studies have shown that these late preterm infants are “functional mature” both in terms of physiology and metabolism, owing to their size and birth weight of new-borns born at term. The main difference between them lies in the neonatal outcomes, where preterm and late preterm are expected to have more of neonatal complications and long term neurological disturbances when compared to term neonates (4).
Several complications contributing to neonatal mortality and morbidity such as respiratory distress syndrome, jaundice, hyperbilirubinemia, apnoea, hypothermia, necrotising enterocolitis, anaemia, infections, sepsis, and haemorrhage are commonly encountered among preterm children (5). Furthermore, it is noted that these children are at an increased risk of having longer hospital stay and readmissions during their neonatal period (6). A study has shown that late preterm are at 7 times the higher risk of neonatal morbidity and mortality compared to term neonates (5). In addition to above mentioned severe complications, these children also face a wide variety of feeding problems, mainly due to immature sucking reflex, swallowing reflex, and delayed onset of lactation (7). These issues also tend to affect the growth of the child during its infancy leading to growth defects, poor weight gain and failure to thrive (8-10).
Despite being an important group of preterm subgroup, the late pre term group is not much researched topic as when compared to the preterm group altogether. Specifically, there is a lacunae in research from Indian settings. It is also evaluated that these late preterm subgroup can account to around 10% of all total births occurring worldwide, thus even a moderate increase in its proportion can lay a sufficient impact on our health systems in place. This is further strained by the increase in the total number of NICU admissions of late preterm across the globe and specifically in a developing country like India. Studies focusing on the neonatal outcomes (morbidity and mortality) among these late preterm children are necessary.
Thus, we conducted this study with the aim of evaluating the pattern of morbidity and mortality among this late preterm subgroup, with specific focus to early neonatal morbidities such as proportion requiring resuscitation, developing hypoglycemia, jaundice, sepsis, and respiratory distress.
Aims and Objectives
AIM
The aim of the study is to compare the early neonatal morbidities in late preterm neonates with term neonates admitted in NICU.
OBJECTIVE
To study the early neonatal morbidities like post resuscitation care, hypoglycemia, jaundice, respiratory distress, sepsis in late preterm neonates and to compare the morbidities with term neonates.
Material and Methods
The study was conducted in Neonatal Intensive Care Unit, Department of Pediatrics, in DDU Hospital, New Delhi after approval of the institutional ethical committee.
Study population: Late preterm neonates and term neonates delivered in DDU Hospital, admitted in NICU after fulfilling the inclusion criteria. Gestation was determined in weeks+days by LMP or USG if patient does not remember LMP.
Study design: prospective observational cohort study.
Study duration: Study was conducted over one and half years period starting from April 2021 to September 2022.
Methodology
The study was carried out over a period of 18 months at Deen Dayal Upadhyay hospital, New Delhi. All late preterm and term neonates admitted in NICU after fulfilling the inclusion criteria were enrolled in the study. Gestation was determined in weeks + days by LMP or USG. The babies were divided into three subgroups on the basis of weight for gestation as AGA/SGA/LGA (Annexure 1). A Pre structured proforma was used to record the information on sociodemographic details and to record clinical information pertaining to neonatal examinations and investigations. After getting the consent from the parents, clinical examination was done and relevant data was extracted and entered into the data collection proforma. The neonates were then followed up till discharge or death. The morbidity profile included in the study were defined as:
1) Post Resuscitation care: Requirement of post-resuscitation care as per latest NRP guidelines. (Annexure 2).
2) Hypoglycemia: Blood glucose of less than 40 mg/dL. Blood sugars were monitored at 12 hourly intervals in all late preterm, IUGR (intrauterine growth restriction), IDM (Infant of diabetic mother) and LGA (Large for gestation, birth weight >2SD) infants. Random blood sugar estimation was also done in all symptomatic infants as per the clinician's discretion.
3) Jaundice: Clinically visible jaundice requiring phototherapy or exchange transfusion as per hour specific total serum bilirubin (TSB) nomogram (AAP chart).
4) Respiratory distress: Presence of at least 2 of the following criteria: Respiratory rate
>60/min, Subcostal/ intercostal recessions, Expiratory grunt/groaning, and requiring oxygen therapy.
5) Sepsis: Probable sepsis. Positive septic screen (two of the five parameters namely, TLC
<5000/mm or >15000/ mm, band to total polymorph ratio of >0.2, absolute neutrophil count less than 1800/mm³ or >7200/mm³, C reactive protein > 0.5mg/dL, platelets <1 lakh mm); or Proven sepsis: Isolation of pathogens from Blood or CSF or Urine.
Inclusion criteria:
1. Group 1: All late preterm newborns between 340/7 weeks to 36+6 weeks.
2. Group 2: Newborns between 370/6 to 416/7 weeks of gestation delivered in DDUH, admitted in NICU were enrolled in the study.
Exclusion criteria:
1. Those infants having major congenital anomalies.
SAMPLE SIZE: 180
SAMPLE SIZE CALCULATION:
The sample size was calculated according to the formula: Cochran’s formula
|
Sample size N = |
r+1 x(zα + z1-β )2*(p1*(1-p1) + p2*(1-p2)) r (p1 – p2)2 |
The sample size for the study was based on a study by Jaiswal et al (2010) who reported the prevalence of any morbidity in late pre term and term babies as follows: (10)
|
|
Prevalence of Any Morbidity |
|
Late Preterm |
70.8% |
|
Term |
29.1% |
r (ratio of number of patients in each arm) = 1 p1 (prevalence in cases) = 0.708
p2 (prevalence in controls) = 0.291 Type I error (α) = 5%, zα= 1.96
Type II error (β) = 1%, Power = 1 – β = 99%, z1-β= 2.326
Based on the formula given above, using the mentioned values, the sample size required was calculated to be 87.27 (~90) per arm.
Thus, assuming 99% power and 95% confidence interval, the sample size required was finally estimated to as 90 patients per arm (total 180).
Measure of Outcome of Interest
1.Occurrence of early neonatal morbidities like need for post resuscitation care, hypoglycaemia, jaundice, respiratory distress, sepsis in late preterm neonates.
2.Comparison of the morbidity profile of late preterm with term neonates.
Statistical Analysis:
Data was coded and recorded in MS Excel spreadsheet program. SPSS v23 (IBM Corp.) was used for data analysis. Descriptive statistics was elaborated in the form of means/standard deviations and medians/IQRs for continuous variables, and frequencies and percentages for categorical variables. Data was presented in a graphical manner wherever appropriate for data visualization using histograms/box-and-whisker plots/column charts for continuous data and bar charts/pie charts for categorical data. Group comparisons for continuously distributed data was made using independent sample ‘t’ test when comparing two groups, and One-Way ANOVA when comparing more than two groups. In case of non-normally distributed, appropriate non-parametric tests in the form of Wilcoxon Test/Kruskal Wallis test were used. In case of comparison of categorical data Chi-squared test was used. Statistical significance was kept at p < 0.05.
Observation and Results
Table 1: Sociodemographic characteristics of the study participants (N=180)
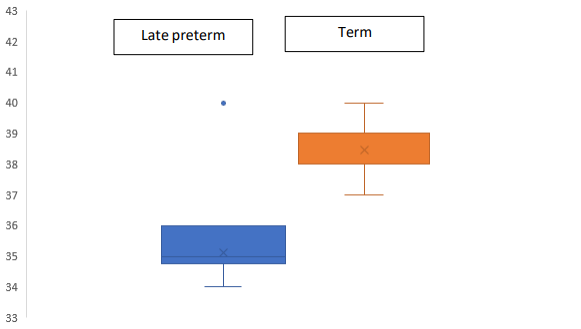
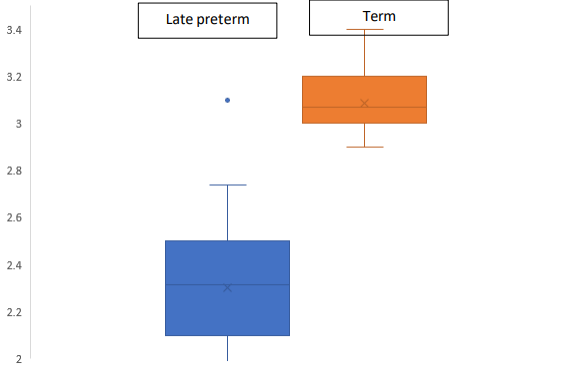
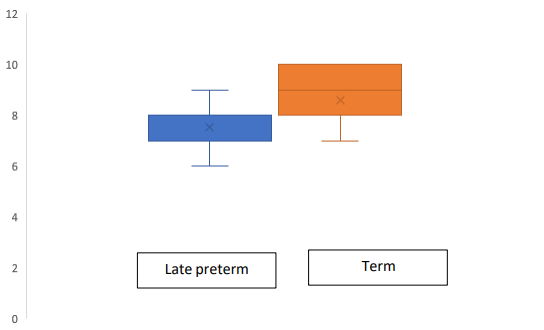
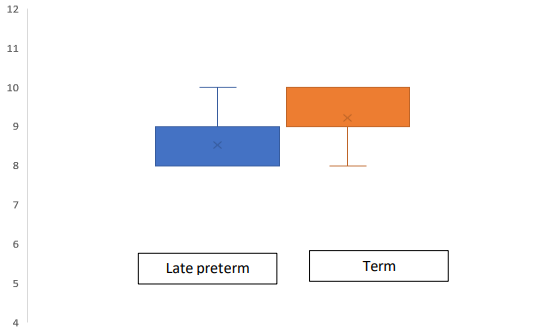
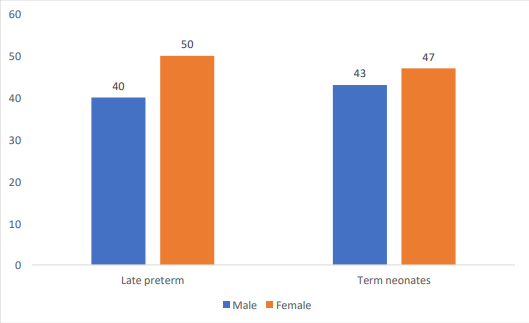
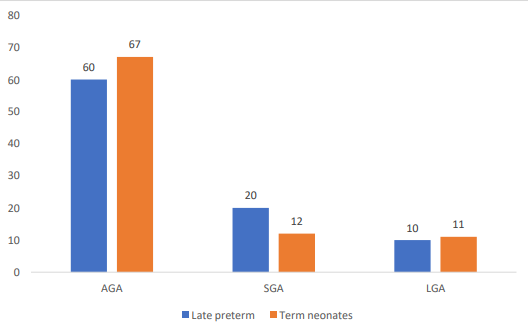
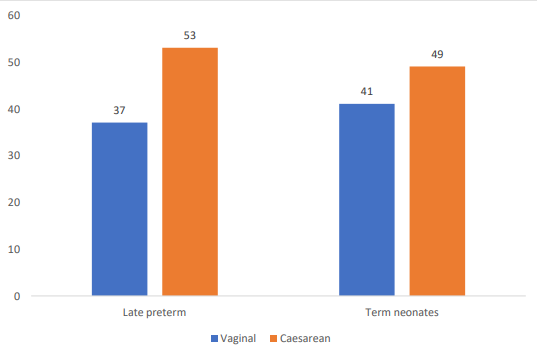
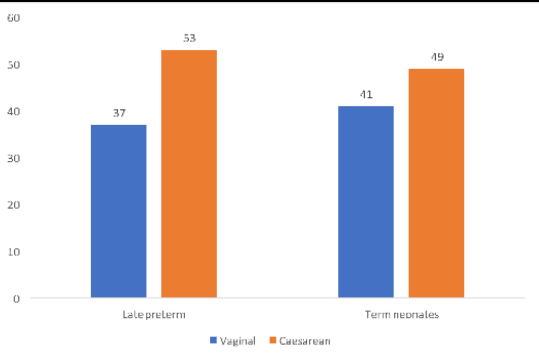
Table 1 describes the sociodemographic characteristics of the study participants. The mean distribution of gestation among the late preterm infants was observed to be 35.39 (±0.78) and term neonates were observed to be 38.64 (±1.11) weeks. The mean birth weight distribution was observed to be 2.35 (±0.48) and 3.04 (±0.43) kgs among late preterm and term neonates. The mean distribution of APGAR scores at 1 min and 5 minutes among late preterm and term neonates were also overserved to be 7.43 (±0.8) vs 7.72 (±0.7) and 8.49 (±0.6) vs 8.77 (±0.5). We observed that males were commonly encountered in both study groups. Small for gestational age children were commonly seen among the late preterm infants when compared to term infants. C section were also commonly observed among the late preterm infants compared to term infants. Almost half of the infants in both study groups had some comorbidity or the other. With respect to the booking status we observed that almost 4/5 of the study participants in both study groups had been previously booked.
Table 2: Comparison of general characteristics and clinical characteristics of the study participants between the study groups (N=180)
Table 2 explains the comparison of general characteristics and clinical characteristics of the study participants between the study groups (N=180). We noted that the groups were comparable with respect to socio demographic and clinical characteristics indicating that the groups were comparable with respect to the baseline characteristics (p value >0.05)
Fig 1,2,3,4,5,6,7,8
Outcome measurement:
Table 3: Comparison of outcome parameters between the study groups (N=180)
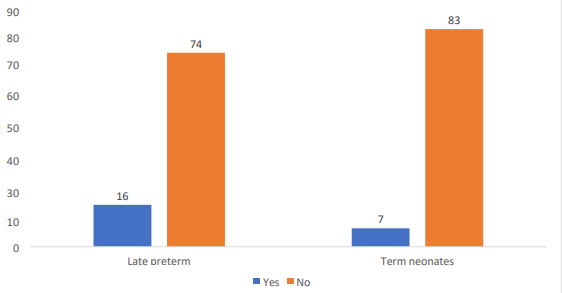
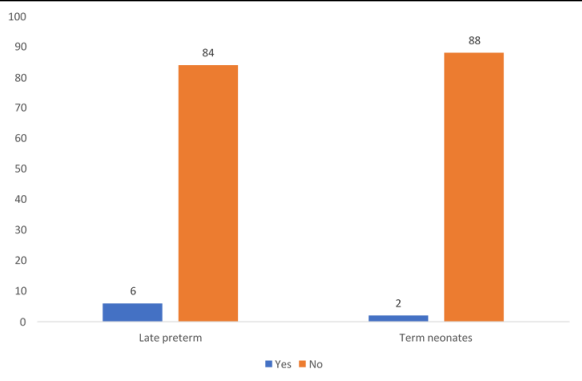
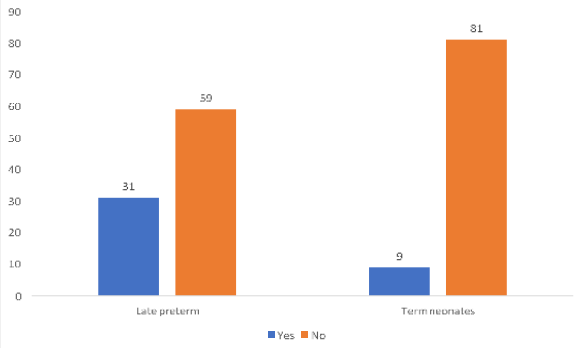
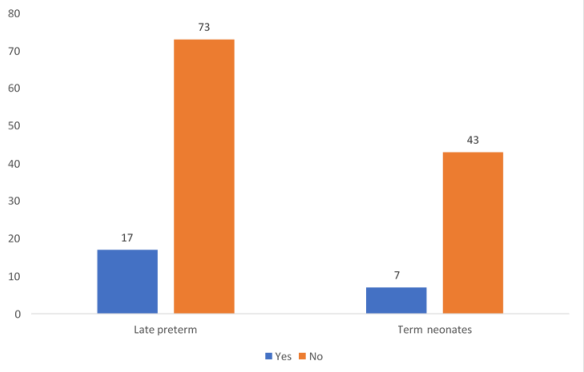
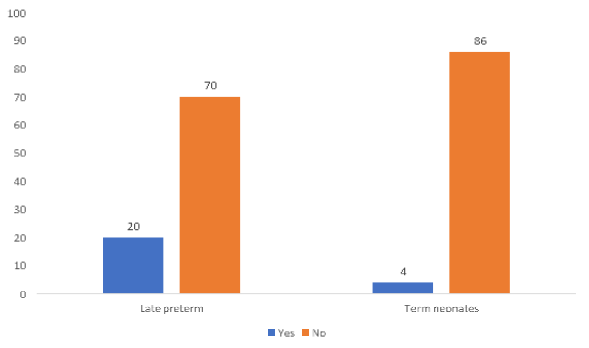
Table 3 represents the comparison of outcome parameters between the study groups. We observed that there was significant difference in the distribution of hypoglycaemia across the study groups with late preterm infants accounting for more hypoglycaemia cases (p value 0.05), we also observed that there was significant difference in the incidence of post resuscitation care across the study groups with late preterm infants requiring more care (p value 0.04) With respect to incidence of respiratory distress also we observed that late preterm infant had higher incidence and was found to be statistically significant (p value 0.001) In cases of incidence of jaundice (p value 0.04) and sepsis (p value 0.001) also we observed that late preterm infants had more incidence of cases when compared to the other group.
Figure 9,10,11,12,13
Please click here to view all figures and tables
Discussion
We basically did a prospective observational study in the Pediatrics - Neonatal Intensive Care Unit attached to a tertiary care setting to find the difference in the morbidity profile of late preterm neonates in comparison with term neonates among admission during a time period of 18 months. In our study, we observed the clinical spectrum of late preterm neonates and compared them with term neonates. We also evaluated the proportion of individuals who had various early neonatal morbidities in both groups. As our primary objective, we have estimated the incidence of early neonatal morbidities like post-resuscitation care, hypoglycemia, jaundice, respiratory distress, and sepsis among late preterm neonates and compared them with term neonates (11). Existent research on this area are mainly focused in western settings, and there is lack of literature from India, specifically from North Indian settings. Thus taking the varied burden of the incidence of preterm labour in recent times and the increased incidence of various morbidity and mortality pattern observed among them, we decided to evaluate the difference in morbidity profile of late preterm neonates in comparison with term neonates (12).
In our results, with respect to the sociodemographic characteristics of the study participants, we observed that the mean distribution of gestation among the late preterm infants was observed to be 35.39 (±0.78) and term neonates were observed to be 38.64 (±1.11) weeks. The mean birth weight distribution was observed to be 2.35 (±0.48) and 3.04 (±0.43) kgs among late preterm and term neonates. This finding was in line with the findings obtained from various other studies done in other study settings, which have also proved that the distribution of low birth weight babies among late preterm deliveries is more when compared to term deliveries, which could be explained by the fact that early preterm babies get little time for development and in utero maturation thereby having more low birth weight incidence (13).
With respect to the baby parameters, we observed that the mean distribution of APGAR scores at 1 min and 5 minutes among late preterm and term neonates was 7.43 (±0.8) vs 7.72 (±0.7) and 8.49 (±0.6) vs 8.77 (±0.5). This finding was also in line with other study findings done by Jain et al and Cheng et al, who have established that late preterm deliveries tend to have low APGAR scores compared to term neonates, owing to differences in maturation (14,15). We observed that males were commonly encountered in both study groups. This finding was however, found to be different from another study done by Ribicic et al, who noted that the incidence of late preterm was more commoner among females when compared to males. The probable reasons for this difference could be owing to the differences in the study characteristics such as study population, co-morbidity profile, and study settings (16).
We also observed that small for gestational age children were commonly seen among the late preterm infants when compared to term infants and C sections were also commonly observed among the late preterm infants compared to term infants. Higher incidence of small for gestational age babies among the preterm deliveries shows that SGA serves as an important risk factor for outcome determination of preterm deliveries, and also it is shown by several studies that being SGA substantially increases the already higher mortality of late preterm and early term newborns, which could be probably explained by the additive effect of both on other morbidity and mortality, or also by the increased prevalence of lethal congenital conditions among both the types. Studies by Pulver et al and Baretto et al, have proved that newborns with SGA and preterm delivery are at increased risk for other complications such as prematurity, neonatal asphyxia, hypothermia, hypoglycemia, hypocalcemia, polycythemia, sepsis, and death (17,18). Our finding of increased incidence of C-sections among preterm deliveries maybe due to increased incidence of complications and fetal hypoxia during labour which has resulted in elective or emergency C sections among preterm deliveries (19,20).
With respect to our primary objective of evaluating the difference in comorbidity profile among both the groups into consideration, we noted that the incidence of hypoglycaemia was observed to be more common in the late preterm groups compared to term infants, and this association was observed to be statistically significant (p value 0.05). Such a finding was observed to be similar to study findings from another study done by Morrocchella et al, who also observed that incidence of hypoglycaemia was observed to be statistically different between late preterm and term babies (21).
With respect to the distribution of post resuscitation care, we noted that the incidence of post resuscitation care was observed to be more common in the late preterm groups compared to term infants, and this association was observed to be statistically significant. (p value 0.04) Such a finding was observed to be similar to study findings from another study done by Rasania et al, who also observed that incidence of post resuscitation care was observed to be statistically different between late preterm and term babies. (22)
Taking the distribution of respiratory distress into consideration, we noted that the incidence of respiratory distress was observed to be more common in the late preterm groups compared to term infants, and this association was observed to be statistically significant (p value 0.001). Such a finding was observed to be similar to study findings from another study done by Kabilan et al, who also observed that the incidence of respiratory distress was observed to be statistically different between late preterm and term babies. (23)
With respect to the distribution of jaundice into consideration, we noted that the incidence of jaundice was observed to be more common in the late preterm groups compared to term infants, and this association was observed to be statistically significant. (p value 0.04) Such a finding was observed to be similar to study findings from another study done by Garg et al, who also observed that the incidence of jaundice was observed to be statistically different between late preterm and term babies (24).
Taking the distribution of sepsis, we noted that the incidence of sepsis was statistically different between the late preterm groups compared to term infants (p value 0.001) Such a finding was observed to be similar to study findings from another study done by Jaiswal et al, who also observed that the incidence of sepsis was observed to be statistically different between late preterm and term babies (25).
Understanding morbidity risk among late preterm infants is not only important for helping newborn care providers to anticipate and to manage potential morbidity during the birth hospitalization and earlier follow-up after hospital discharge, but also may possibly assist in guiding non-emergency obstetric intervention decisions. We could not find many studies, especially from a North Indian setting that has tried to venture into the difference in incidence of selected morbidities among late preterm and term deliveries. Thus, through our study results, we have found that there is increased incidence and a statistically significant difference in the distribution of morbidities among the late preterm when compared to term infants (25-30).
Conclusion
To conclude, in our study of 180 infants, for which we had taken 90 children with late preterm and 90 term infants, we found that the mean distribution of gestation among the late preterm infants and term infants was observed to be 35.39 (±0.78) vs 38.64 (±1.11) weeks, with male predominance in both study groups. Outcome analysis using chi-square test showed that there was a significant difference in the incidence of morbidities such as hypoglycemia, post resuscitation care, respiratory distress, jaundice and sepsis in the late preterm group when compared to term infants. By our results, we conclude that late preterm infants are at an increased risk of morbidity when compared to term infants.
Strengths:
Strengths and limitations
Our study had several strengths:
1. Ours was one among the very few studies that compared the clinical presentation late preterm and term infants of from a North Indian hospital-based setting.
2. Ours was one among the very few studies that tried to establish the association between the incidence of morbidities between late preterm and term infants from a North Indian hospital-based setting.
Limitations:
Despite all our study had certain limitations:
Limitations of this study are generally attributed to the observational nature of this study and the constraints of the ability to establish causal relationships between the exposure and outcome
1. The findings are generalisable only to similar study settings, as the study was conducted only from one single centre in North India.
References
1. Map of European Countries by Birth Rate [Internet]. Mapsofworld.com. 2016 [cited 1 December 2021]. Available from: http://www.mapsofworld.com/europe/thematic/ countries-by- birth-rate.html
2.Preterm Birth | Maternal and Infant Health | Reproductive Health | CDC [Internet]. Cdc.gov. 2016 [cited 14 December 2021]. Available from: http://www.cdc.gov/ reproductivehealth/maternalinfanthealth/pretermbirth.htm
3. Preterm birth [Internet]. World Health Organization. 2016 [cited 13 December 2021].Available from: http://www.who.int/mediacentre/factsheets/fs363/en/
4. Tsai ML e. Prevalence and morbidity of late preterm infants: current status in a medical center of Northern Taiwan. - PubMed - NCBI [Internet]. Ncbi.nlm.nih.gov. 2016 [cited 13 December 2021]. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22770105
5. Zeitlin J, Szamotulska K, Drewniak N, Mohangoo A, Chalmers J, Sakkeus L et al. Preterm birth time trends in Europe: a study of 19 countries. BJOG: An International Journal of Obstetrics & Gynaecology. 2013;120(11):1356-1365.
6. Picone S, Aufieri R, Paolillo P. Infection in late preterm infants. Early Human Development [Internet]. 2014 [cited 15 January 2016];90:S71-S74. Available from: http://www.sciencedirect.com/science/article/pii/S0378378214700222
7. Whyte RK, Canadian Paediatric Society, Fetus and Newborn Committee. Safe discharge of the late preterm infant. Paediatrics & child health. 2011 Feb 1;15(10):655- 60.
8. Gianni? M, Roggero P, Piemontese P, Liotto N, Orsi A, Amato O et al. Is nutritional support needed in late preterm infants?. BMC Pediatrics [Internet]. 2015 [cited 8 December 2021];15(1). Available from: http://bmcpediatr.biomedcentral.com
/articles/10.1186/s12887- 015-0511-8#CR5
9. Breastfeeding the preterm infant [Internet]. Uptodate.com. 2016 [cited 10 January 2021]. Available from: http://www.uptodate.com/contents/breastfeeding-the-preterm- infant?source=machineLearning&search=feeding+in+late+preterms+infants&selecteTitle=2~ 150§ionRank=3&anchor=H16#H16
10. Jaiswal A, Murki S, Gaddam P, Reddy A. Early neonatal morbidities in late preterm infants. Indian pediatrics. 2011 Aug 1;48(8):607.
11. Quinn JA, Munoz FM, Gonik B, Frau L, Cutland C, Mallett-Moore T, Kissou A, Wittke F, Das M, Nunes T, Pye S. Preterm birth: Case definition & guidelines for data collection, analysis, and presentation of immunisation safety data. Vaccine. 2016 Dec 1;34(49):6047-56.
12. Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J. Maternal psychological distress and parenting stress after the birth of a very low-birth-weight infant. Jama. 1999 Mar 3;281(9):799-805.
13. Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. The lancet. 2008 Jan 5;371(9606):75-84.
14. Lawn JE, Davidge R, Paul VK, Xylander SV, de Graft Johnson J, Costello A, Kinney MV, Segre J, Molyneux L. Born too soon: care for the preterm baby. Reproductive health. 2013 Nov;10(1):1-9.
15. Sebastiani G, Borrás-Novell C, Alsina Casanova M, Pascual Tutusaus M, Ferrero Martínez S, Gómez Roig MD, García-Algar O. The effects of alcohol and drugs of abuse on maternal nutritional profile during pregnancy. Nutrients. 2018 Aug 2;10(8):1008.
16. Michael Cohen-Wolkowiez P. Early and Late Onset Sepsis in Late Preterm Infants. The Pediatric infectious disease journal [Internet]. 2009 [cited 7 January 2016];28(12):1052. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/ PMC2798577/
17. Honnor MJ, Zubrick SR, Stanley FJ. The role of life events in different categories of preterm birth in a group of women with previous poor pregnancy outcome. European journal of epidemiology. 1994 Apr;10(2):181-8.
18. Sasidharan K, Dutta S, Narang A. Validity of New Ballard Score until 7th day of postnatal life in moderately preterm neonates. Archives of Disease in Childhood-Fetal and Neonatal Edition. 2009 Jan 1;94(1):F39-44.
19. Tucker JM, Goldenberg RL, Davis RO, Copper RL, Winkler CL, Hauth JC. Etiologies of preterm birth in an indigent population: is prevention a logical expectation?. Obstetrics and gynecology. 1991 Mar 1;77(3):343-7.
20. Shapiro-Mendoza C, Tomashek K, Kotelchuck M, Barfield W, Nannini A, Weiss J et al. Effect of Late-Preterm Birth and Maternal Medical Conditions on Newborn Morbidity Risk. PEDIATRICS. 2008;121(2):e223-e232.
21. Martin JA, Hamilton BE, Osterman MJ, Curtin SC, Matthews TJ. Births: final data for 2013. Natl Vital Stat Rep. 2015 Jan 15;64(1):1-65. PMID: 25603115.
22. Haroon A, Ali SR, Ahmed S, Maheen H. Short-term neonatal outcome in late preterm vs. term infants. J Coll Physicians Surg Pak. 2014 Jan;24(1):34-8. PMID: 24411540.
23. Engle WA, Tomashek KM, Wallman C, Committee on Fetus and Newborn. “Late- preterm” infants: a population at risk. Pediatrics. 2007 Dec;120(6):1390-401.
24. Das R, Palas R, Deb G, Paul P, Yesmin S. An Observational Study on Late Preterm Neonates from a Post- Graduate Teaching Hospital in North East India. Sch J App Med Sci. 2020: 4 (8). 2484-88
25. Wang ML, Dorer DJ, Fleming MP, Catlin EA. Clinical outcomes of near-term infants. Pediatrics. 2004 Aug;114(2):372-6. doi: 10.1542/peds.114.2.372. PMID: 15286219.
26. Visruthan NK, Agarwal P, Sriram B, Rajadurai VS. Neonatal Outcome of the Late Preterm Infant (34 to 36 Weeks): The Singapore Story. Ann Acad Med Singap. 2015 Jul;44(7):235-43. PMID: 26377057.
27. Late preterm infants [Internet]. Uptodate.com. 2016 [cited 11 January 2020]. Available from: http://www.uptodate.com/contents/late-preterm- infants?source =machine Learning&search=morbidity+preterm&selectedTitle=2~150§ionR ank=1&anchor=H8#H8
28. Consortium on Safe Labor, Hibbard JU, Wilkins I, Sun L, Gregory K, Haberman S, Hoffman M, Kominiarek MA, Reddy U, Bailit J, Branch DW, Burkman R, Gonzalez Quintero VH, Hatjis CG, Landy H, Ramirez M, VanVeldhuisen P, Troendle J, Zhang J. Respiratory morbidity in late preterm births. JAMA. 2010 Jul 28;304(4):419-25. doi: 10.1001/jama.2010.1015. PMID: 20664042; PMCID: PMC4146396.
29. Ballabh P. Intraventricular hemorrhage in premature infants: mechanism of disease. Pediatric research. 2010 Jan;67(1):1-8.
30. Dammann O, Leviton A. Maternal intrauterine infection, cytokines, and brain damage in the preterm newborn. Pediatr Res. 1997 Jul;42(1):1-8. doi: 10.1203/00006450- 199707000-00001. PMID: 9212029.