Case Series - Techniques for Removal of Proximally Migrated or Broken Pancreatic Stents.
Case Series - Techniques for Removal of Proximally Migrated or Broken Pancreatic Stents.
Rahil Desai, DO; Ahamed Khalyfa, DO; Navkiran Randhawa, DO; Mahnoor Inamullah, MD; Varshita Goduguchinta, DO; Kamran Ayub, MD, MRCP, FASGE*
*Correspondence to: Dr. Kamran Ayub, MD, MRCP, FASGE, US.
Copyright
© 2024 Dr. Kamran Ayub. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 April 2024
Published: 01 May 2024
Case Series - Techniques for Removal of Proximally Migrated or Broken Pancreatic Stents.
Introduction:
During endoscopic retrograde cholangiopancreatography (ERCP), pancreatic stents (PS) are commonly used to reduce the risk of post ERCP pancreatitis and to facilitate pancreatic drainage. While proximal PS migration is uncommon (reported in 2-5% of cases), migration of a pancreatic duct stent may cause pancreatitis, pancreatic abscess, or pancreatic duct stenosis. Therefore, it may be necessary to retrieve the migrated stent. In our study, we review the efficacy of different techniques including Spyglass retrieval basket, Soehendra Stent retriever, and Spyglass forceps for proximally migrated pancreatic stents.
Case/Methods:
A retrospective review of patients who received ERCP at our facility between November 2016 and July 2022 who were found to have proximally migrated pancreatic stents or broken stents in the PD were included. Stents were placed for prophylaxis of post-ERCP pancreatitis in two patients, chronic pancreatitis with stricture in one patient, and pancreatic duct (PD) stone in one patient. All four patients had previous attempts at removal of stents at outside institutions. After insertion of 0.025 mm guide wire, Spyglass pancreatoscopy (Boston Scientific, Natick, Massachusetts, USA) was performed on four patients. PD was balloon dilated in two patients. In two patients, stents were removed using Spyglass basket while one patient had a broken stent removed with Spyglass Forceps. In one patient the stent was cannulated with guidewire and removed using Soehendra retriever. This stent was impacted and therefore was amenable to removal by Soehendra retriever. The other stents were mobile in the dilated pancreatic duct and thus were not amenable to removal using Soehendra retriever.
Results:
The procedure was technically successful in all. All four patients were found to have migration of stents into the proximal portion of the pancreatic duct. Two of the patients were noted to have a broken stent. The migrated stents were 5 Fr x 7 cm, 5 Fr x 5 cm, and 5 Fr x 1.5 cm (broken stent) & 5 Fr x 2 cm (broken stent). Two patients were noted to have pancreatic duct narrowing and balloon dilation. Two stents were successfully retrieved using Spyglass retrieval basket. One was retrieved using large Spybite Forceps, and one using Soehendra retrieval device. The average duration of the procedure was 30 to 45 minutes for all patients. The patients had repeat stents placed. All patients were monitored in the hospital for 24 hours and all stents were removed in 3 to 4 weeks successfully.
Figure 1: Migrated Stent Retrieval Method
|
Patient |
Age |
Gender |
Size of stent retrieved |
Duration of original stent prior to extraction |
Methodology of stent extraction |
|
1 |
71 |
M |
5 Fr x 1.5 cm (Broken stent) |
4 weeks |
SpyGlass Forceps |
|
2 |
68 |
M |
5 Fr x 5 cm |
2 years |
Spyglass Basket |
|
3 |
63 |
F |
5 Fr x 7cm |
8 months |
Spyglass Basket |
|
4 |
67 |
M |
5 Fr x 2cm (Broken stent) |
1 year |
Soehendra retriever stent |
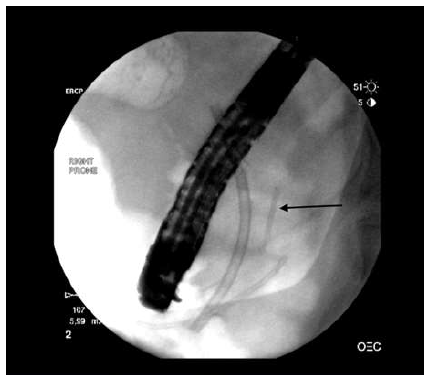
Figure 2: Broken Stent Neck of Pancreas
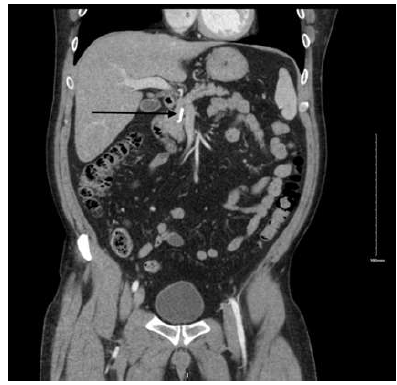
Figure 3: Stent Piece Neck of Pancreas
Conclusion:
In conclusion, the inward migration of a pancreatic duct stent can lead to complications such as pancreatitis, pancreatic abscess, or pancreatic duct stenosis. Consequently, retrieving the migrated stent may become essential. Our pilot study demonstrates the effectiveness of various methods, including the Spyglass retrieval basket, Soehendra stent retriever, and Spyglass forceps, in safely managing proximally migrated pancreatic stents.
References
1. ahimi A, Ejtehadi F. SpyGlass Pancreatoscopy and Successful Retrieval of a Proximally Migrated Pancreatic Stent; Unusual Case and Technical Tips. Middle East J Dig Dis. 2016 Jul;8(3):232-234. doi: 10.15171/mejdd.2016.26. PMID: 27698974; PMCID: PMC5045677.
2.Al-Shahrani AA, Swei E, Wani S, Shah RJ. Pancreatoscopy-guided retrieval of a migrated pancreatic duct stent. VideoGIE. 2022 Sep 30;7(11):417-418. doi: 10.1016/j.vgie.2022.08.007. PMID: 36407045; PMCID: PMC9669771.
3.Thongpiya J, Lanke G, Yingchoncharoen P, Das K. SpyGlass DS system-assisted retrieval of proximally migrated pancreatic duct stent in a patient with chronic pancreatitis. JGH Open. 2023 Nov 30;7(12):1009-1011. doi: 10.1002/jgh3.13007. PMID: 38162846; PMCID: PMC10757486.