Total Knee Arthroplasty for Acute Fractures around the Knee
Total Knee Arthroplasty for Acute Fractures around the Knee
Syed Muhammad Tayyab Hassan *
*Correspondence to: Syed Muhammad Tayyab Hassan, Registrar Orthopedic Surgery, Allied Hospital & Punjab Medical College Faisalabad, Pakistan.
Copyright
© 2020 Syed Muhammad Tayyab Hassan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 June 2020
Published: 21 June 2020
Abstract
Primary total knee arthroplasty (TKA) is a proposed alternative to open reduction and internal fixation for complex fractures in elderly osteoporotic patients. TKA aims to save the patient's life, limit decubitus complications, and save knee function and autonomy through early mobilization. The main indications include complex articular fractures in elderly patients with symptomatic osteoarthritis, complex articular fractures of the tibial plateau in elderly patients whose bone quality makes internal fixation hazardous, and major destruction of the distal femur in younger patients. Preoperative management is crucial, including multidisciplinary approaches to manage comorbidities, anemia and pain, and vascular and cutaneous conditions. Surgical technique is based on the basic principles of revision surgery, with primary temporary reduction for complex distal femur fractures. Complementary internal fixation may be required for diaphyseal extension and inter-prosthetic fractures. Primary TKA results are generally better than secondary TKA after failure of non-operative treatment or internal fixation, with lower revision rates, earlier full weight-bearing, and better functional results. However, loss of autonomy is frequent and 1-year mortality is high, especially following complex femoral fractures in the elderly.
Keywords: Distal femur fracture, Proximal tibia fracture, Total knee arthroplasty, Elderly Osteoporosis, Adult.
Total Knee Arthroplasty for Acute Fractures around the Knee
Introduction
Arthroplasty is a common treatment for acute fractures of the proximal femur, complex proximal humerus fracture, or elbow fracture, but is less common in complex knee fractures. The main objective of arthroplasty in fractures of the proximal femur is to save the patient's life by limiting decubitus complications, thanks to immediate resumption of weight-bearing. For the shoulder and elbow, the objective is to save joint function, thanks to immediate postoperative mobilization. Most complex knee fractures in the elderly are treated by internal fixation or even non-operatively. However, there are good reasons for treating certain acute complex fractures using an arthroplasty, such as significant symptomatic osteoarthritis prior to the fracture, fracture complexity, bone fragility making fixation hazardous, and the need for early mobilization and the earliest possible resumption of walking in elderly patients to avoid decubitus complications and the risk becoming bed-ridden (1).
The present study hypothesis was that knee arthroplasty could be a solution for acute fractures around the joint in elderly osteoporotic patients, in order to limit decubitus complications and preserve knee function (2). The fundamental principles of this treatment include the importance of early resumption of full weight-bearing and saving function thanks to immediate unrestricted joint mobilization. In the knee, reconstruction using arthroplasty is sometimes the only surgical option that fulfills the two requirements of saving the patient's life thanks to early resumption of full weight-bearing and saving function thanks to immediate unrestricted joint mobilization (3).
The incidence of complex epiphyseal knee fracture is much lower than for fractures of the femoral neck, proximal humerus, or elbow, accounting for around 1% of annual emergency admissions. The exact incidence of knee joint fracture is hard to determine, as it varies according to demographic and geographical factors. In a series of more than 6,000 fractures, annual incidence of proximal tibia fracture was 13.3 per 100,000 in adults, and 4.5 per 100,000 for distal femoral fracture (4).
Internal fixation of complex knee fracture in elderly patients shows loss of reduction in 30-79% of cases for the proximal tibia, with patient age, osteoporosis, comminution, and initial displacement as risk factors. Reliable internal fixation is difficult to achieve in diaphyseal, metaphyseal, and epiphyseal fracture in severely osteoporotic patients (5). For these patients, weight-bearing is often proscribed for at least 6 weeks, which greatly limits mobilization, as these patients are unable to use crutches without weight-bearing. In case of severe joint comminution with osteoporotic bone and osteoarthritis, the benefit of internal fixation followed by non-weight-bearing is highly questionable (6).
To minimize the number of procedures and optimize functional results, Wolfgang was the first to report a case of rheumatoid arthritis treated in emergency by total knee arthroplasty (TKA) for an epiphyseal fracture of the distal femur. Subsequently, case reports and small series have been published. Results in these first series were relatively satisfactory; indications were progressively refined and the technique developed (7).
Treatment
The primary arthroplasty can be an interesting solution for acute fractures around the joint in elderly osteoporotic patients, fulfilling two treatment requirements while reducing the number of procedures, saving the patient's life thanks to early resumption of weight-bearing, limiting decubitus complications, and saving function, thanks to immediate unrestricted joint mobilization, minimizing loss of autonomy.
The destruction of the distal femur in road accidents in younger patients is a controversial and less frequent indication. It is indicated only when internal fixation seems unfeasible due to the complexity of the fracture, and first-line arthroplasty can only be considered when a major bone defect might require a tumor-prosthesis implant or fusion using a modular or customized intramedullary nail. The integrity of the extensor mechanism should be checked, and in case of open fracture, skin cover and healing must be perfect before considering any arthroplasty (8,9).
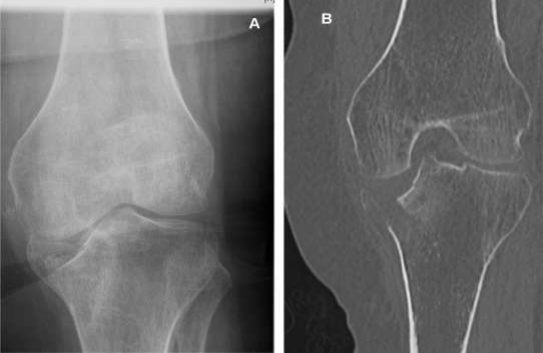
Fig. 1. A. The patient presents in emergency with complex comminuted joint fracture of the distal femur. Radiography shows signs of osteoarthritis, and interview usually finds that the patient is already suffering and that TKA had been indicated before the fall., B. Same situation, with tibial fracture.
Fig. 2. A–B. Check that there is no long hip implant stem or other material liable to hinder implantation
There is a major risk of infection and long-term prognosis, which limits indications. Therefore, these cases should be discussed on a case-by-case basis; reconstruction by implant should be chosen only if no conservative solution seems available. To optimize surgical planning, these patients are admitted in emergency but need to be prepared and managed as for scheduled surgery: local and general preparation of the patient, the surgical team itself, and it is important to order adequate implants and ancillary instrumentation so as not to delay treatment (10).
Rigid ortho-geriatric management is required for these patients, taking into account comorbidity, fracture-related anemia, pain control, adhesive traction or cast immobilization, and analysis of skin condition. Open fractures are rare in low-energy trauma in elderly patients, but open fracture may be observed in massive distal femur destruction in young poly-trauma patients. Vascular lesions are rare but should be systematically screened for before surgery. Venous insufficiency may contraindicate surgery if there is any doubt concerning satisfactory skin healing due to poor vascular condition.
Fig. 3. Elderly patient presents in emergency with complex joint fracture of the proximal tibia, with osteoporotic bone. The complexity of the fracture, which is often very proximal and with considerable step-off of the articular surface, makes internal fixation uncertain.
Fig. 4. In complex proximal tibial fracture in the elderly, it seems more logical to suggest first-line arthroplasty with metaphyseal and epiphyseal tibial reconstruction, to enable immediate weight-bearing, rather than attempting internal fixation, with its high risk of failure (A), requiring subsequent removal of the hardware followed by implantation (B) with the same reconstruction requirements as in first-line arthroplasty.
Surgical planning determines the precise needs for material, and although these patients are admitted in emergency, surgery has to be accurately planned as quickly as possible, taking account of the time needed to procure equipment. Technical specificities include thorough knowledge of the basic rules of revision surgery, such as choice of constraint, planning of joint-line restoration and component rotation, bone defect filling, implant fixation, and complementary internal fixation(11).
Fig. 5. Complete destruction of the distal femur in road accidents in younger patients is rarer (A), but may in some cases be a good indication for first-line arthroplasty (B)
In France, emergency traumatology surgery is usually performed by junior surgeons, but first-line TKA for fracture should be performed by or with the help of an experienced surgeon. The three main stages of TKA revision with joint reconstruction should be applied, with the main goal being to enable the patient to stand up and resume full weight-bearing immediately after surgery.
The choice of implant and constraint for a tibial fracture depends on the level and degree of metaphyseal destruction. For fractures involving tibial or femoral collateral ligament insertions, a rotating-hinge implant is recommended, as it is usually impossible to achieve solid internal fixation of the condyles preserving a functional collateral ligament insertion. In severe metaphyseal destruction up to the diaphysis, a segmental mega-prosthesis should be used, especially on the femoral side (12).
Preoperative analysis is crucial, with excellent preoperative radiographic views and CT with 3D reconstruction being helpful. Patient positioning is also important, with the surgeon's preference being used. Tourniquets are not used to release the extensor system and obtain adequate exposure, especially for mega-prostheses. Tranexamic acid is recommended for elderly patients, as contraindications are increasingly rare and cell-saver.
Fig. 6. Some fractures could be excellent indications (A), but severe venous insufficiency is not unusual (B) and may become a contraindication if there is any doubt regarding the proper healing of the skin due to poor vascular status.
The approach for revision TKA should be the surgeon's choice, using the extended sub-vastus approach, which is a quad-sparing solution and avoids the need for anterior tibial tubercle osteotomy or oblique quadriceps tenotomy. The main difficulty in tibial fracture is achieving a stable base-plate and appropriate fixation. Joint-line level and tibial rotation can be determined by following principles.
Comminuted lateral condyle fractures require respecting the medial plateau and reconstructing the tibial base, maintaining joint-line level, and determining rotation. Lateral defect filling is important for stability ((13,14).
In revision surgery, the joint-line is traditionally supposed to lie about 25 mm distal to the medial epicondyle and/or 10 mm proximal to the head of the fibula. Primary temporary reduction enables the individual native joint-line level to be restored, and the distance between the mark and the native joint-line is measured using a ruler. This distance will then be used for femoral reconstruction.
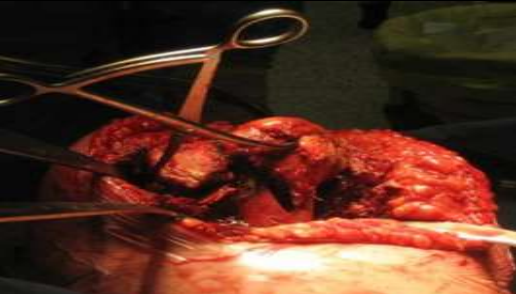
Fig: 7 Principle of primary temporary reduction.
In complex femoral fractures, the rotation of the future femoral implant can be difficult to determine. To determine the joint-line level, the native femoral rotation should be taken as reference. This can be done after temporary primary reduction, marking the femoral shaft axis with an electric cautery to indicate epiphyseal-metaphyseal rotation (15, 16).
In cases of complex fracture of the tibial plateau, tibial rotation should be determined based on the remaining classical bony landmarks, and notably the tibial tubercle, while ensuring congruence with the femoral component in extension. In such cases, the technique used for hip hemi-arthroplasties is recommended: measuring one of the native condyles with a caliper and selecting the corresponding femoral implant (17).
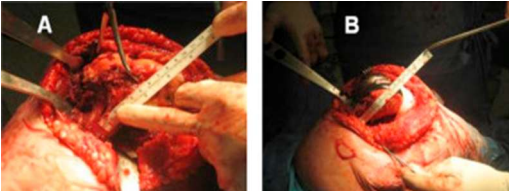
Fig. 8. A. Once this reduction has been achieved and stabilized by reduction clamps, a mark is made on the proximal femur using an electric cautery and a ruler measures the distance between the mark and the native joint-line. B. This distance will then be used for femoral reconstruction.
Bone defect filling or reconstruction implant? Two types of defects can be considered: segmental defects, reconstructed using structural graft, and cavitary defects, reconstructed using a bone cavity filling method. Various types of graft can be used, depending on the surgeon's habits, and should be included in the preoperative planning. Porous tantalum cones are particularly adapted when a conventional implant is used. In these osteoporotic patients, it is important to find a reliable metaphyseal support, which can be obtained with these cones or other metallic reconstruction systems (18).
The principles of implant fixation are those of prosthetic revision, with three zones of fixation: epiphyseal, metaphyseal, and diaphyseal. To be reliable, fixation should involve at least two of the three zones. The literature reports no superiority between a long uncemented stem with diaphyseal engagement and a shorter cemented stem in revision TKA. The current trend favors fully cemented stems, but with a short stem associated to metaphyseal reconstruction using a cone or a sleeve to optimize the metaphyseal reconstruction.
Complementary internal fixation is taken at the end of procedure and is also important due to sudden changes in bone elasticity caused by prosthetic implants in osteoporotic patients. It allows immediate resumption of full weight-bearing without risk of postoperative periprosthetic fracture (19).
Fig 9: The ultimate stage of segmental bone defect is complete metaphyseal and epiphyseal destruction in severely comminuted fracture, in which case a segmental implant may be needed.
Underlying diaphyseal fragility should not be ignored during adjacent metaphyseal reconstruction. Metallic cerclages associated to cemented stem fixation allow immediate resumption of weight-bearing and reduces the risk of periprosthetic fracture. Ipsilateral hip prostheses lead to a risk of interprosthetic fracture in the bone segment between the two stems, which could be a dramatic complication. Internal fixation using a plate is then recommended to bridge the area between the TKA and THA stems for a length at least twice the diameter of the diaphysis (20).
Postoperative management is needed to remedy blood loss, prevent decubitus complications, manage anticoagulation, and treat comorbidities. Key points include the classical principles of multidisciplinary postoperative management, including geriatricians, and current reconstruction techniques that allow immediate resumption of weight-bearing in most cases.
Results
The results of first-line arthroplasty for fracture are encouraging and better than those of arthroplasty secondary to failure of conservative treatment such as internal fixation. Complication rates of TKAs for recent fractures range between 8% and 42%, with low revision rates and usually satisfactory functional results. In secondary post-traumatic TKAs, complications rates range between 20% and 48%, implant revision rates range between 8% and 20%, and functional results are satisfactory in only 75% of cases.
In fragile patients, there are general complications potentially related to three successive operations (internal fixation, hardware removal, then TKA implantation) and a period of non-weight-bearing or protected weight-bearing following the internal fixation. The French Hip and Knee Society's multicenter series of TKA for acute fracture is the largest published to date, with 26 patients (21 female, 5 male), mean age 80.5 years, and mean ASA score 2.2. There were 2 local complications: 1 skin complication and 1 anterior tibial tubercle avulsion, in agreement with previous reports. Anterior tibial tubercle avulsion in fracture, sometimes considered as a contraindication for TKA, should be carefully screened for on the preoperative CT.
Functional results were satisfactory, with good recovery of range of motion but decreased by a mean 1.7 points, and results were poorer in case of low preoperative Parker score. The most recent published series was a French retrospective study of 21 TKAs in patients with a mean age of 79 years, with a mean time to surgery of 3.9 days. The local complications rate was 9%, and functional results were comparable with the literature but with a mean 2-point decrease in Parker score.
Conclusion
In comparison between two techniques in femoral fracture with severe metaphyseal destruction was in favor of the segmental prosthesis, without increased complications and with systematic resumption of weight-bearing. The surgical technique requires excellent knowledge and experience of the principles of prosthetic revision, and it is complex and should be performed on a delayed emergency basis to optimize planning and logistic preparation.
Reference
[1] Obert L, Saadnia R, Tournier C, Bonnevialle N, Saragaglia D, Sirveaux F, La SOFCOT. Four-part fractures treated with a reversed total shoulder prosthesis: prospective and retrospective multicenter study. Results and complications. Orthop Traumatol Surg Res 2016;102:279–85.
[2] Bonnevialle P, Feron JM. Fractures of the over 80 years old. Rev Chir Orthop Reparatrice Appar Mot 2003;89(suppl 5):S129–82.
[3] Bohm ER, Tufescu TV, Marsh JPJ. The operative management of osteoporotic fractures of the knee: to fix or replace? Bone Joint Surg Br 2012;94:1160–9.
[4] Ries MD. Primary arthroplasty for management of osteoporotic fractures about the knee. Curr Osteoporos Rep 2012;10:322–7.
[5] Boureau F, BenadK, Putman S, Dereudre G,Kern G, et al. Does primary total knee arthroplasty for acute knee joint fracture maintain autonomy in the elderly? A retrospective study of 21 cases. Orthop Traumatol Surg Res 2015;101:947–51.
[6] Parratte S, Bonnevialle P, Pietu G, Saragaglia D, Cherrier B, Lafosse JM. Primary total knee arthroplasty in the management of epiphyseal fracture around the knee. Orthop Traumatol Surg Res 2011;97(6 Suppl):S87–94.
[7] Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury
2006;37:691–7.
[8] Wolfgang GL. Primary total knee arthroplasty for intercondylar fracture of the femur in a rheumatoid arthritic patient. A case report. Clin Orthop Relat Res 1982;171:80–2.
[9] Bell KM, Johnstone AJ, Court-Brown CM, Hugues SP. Primary knee arthroplasty for distal femoral fractures in elderly patients. J Bone Joint Surg Br 1992;74:400.
[10] Rolston LR, Christ DJ, Halpern A, O’Connor PL, Ryan TG, Uggen WM. Treatment of supracondylar fractures of the femur proximal to a total knee arthroplasty. A report of four cases. J Bone Joint Surg Am 1995;77:924–31.
[11] Yoshino N, Takai S, Watanabe Y, Fujiwara H, Ohshima Y, Hirasawa Y. Primary total knee arthroplasty for supra condylar/condylar femoral fracture in osteoarthritic knee. J Arthroplasty 2001;16:471–5.
[12] Nau T, Pflegerl E, Erhart J, Vecsei V. Primary total knee arthroplasty for periarticular fractures. J Arthroplasty 2003;18:968–71.
[13] Killian U. Total knee replacement for primary treatment of intra-articular head fractures in elderly patients. Unfallchirurg 2003;106:1046–50.
[14] Rosen AL, Strauss E. Primary total knee arthroplasty for complex distal femur fractures in elderly patients. Clin Orthop 2004;425:101–5.
[15] Nourissat G, Hoffman E, Hémon C, Rillardon L, Guigui P, Sautet A. Total knee arthroplasty for recent severe fracture of the proximal tibial epiphysis in the elderly subject. Rev Chir Orthop Reparatrice Appar Mot 2006;92:242–7.
[16] Folbert EC, Hegeman JH, Vermeer M, Regtuijt EM, van der Velde D, Ten Duis HJ, et al. Improved 1-year mortality in elderly patients with a hip fracture following integrated orthogeriatric treatment. Osteoporos Int 2017;28:269–77.
[17] Huten D. Femorotibial bone loss during revision total knee arthroplasty. Orthop Traumatol Surg Res 2013;99(1 Suppl):S22–33.
[18] Morgan-Jones R, Oussedik SI, Graichen H, Haddad FS. Zonal fixation in revision total knee arthroplasty. Bone Joint J 2015;97-B(2):147–9. S80 S. Parratte et al. / Orthopaedics & Traumatology: Surgery & Research 104 (2018) S71–S80
[19] Appleton P, Moran M, Houshian S, Robinson CM. Distal femoral fractures treated by hinged total knee replacement in elderly patients. J Bone Joint Surg 2006;88B:1065–70.
[20] Pearse EO, Klass B, Bendall SP, Railton GT. Stanmore total knee replacement versus internalfixation for supracondylar fractures ofthe distalfemur in elderly patients. Injury 2005;36:163–8.