Analyze the Different Cardiovascular Risk Assessment Tools Available.
Analyze the Different Cardiovascular Risk Assessment Tools Available.
Dr. Aamir MD *
*Correspondence to: Dr Aamir MD, Associate Clinical Cardiologist, Hyderabad, India.
Copyright
© 2024 Dr Aamir MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 Dec 2024
Published: 21 Dec 2024
Abstract
Background: Cardiovascular diseases (CVD) remain a leading cause of global morbidity and mortality, necessitating accurate and reliable tools for risk assessment. Various cardiovascular risk prediction models have been developed to identify at-risk individuals and guide preventive strategies.
Objective: This review aims to evaluate and compare widely used cardiovascular risk assessment tools, including their key variables, predictive accuracy, and population-specific applications.
Methods: A systematic review of cardiovascular risk assessment tools was conducted using data from peer-reviewed journals, clinical guidelines, and cohort studies. Tools analyzed included the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation (SCORE), Reynolds Risk Score (RRS), ASCVD 2018 Risk Estimator, China-PAR, PREDICT-CVD, JBS3, and advanced tools such as Astro-CHARM and Coronary Artery Calcium (CAC) Scoring. Key parameters such as age, sex, lipid profile, blood pressure, diabetes, smoking status, inflammation markers, and socioeconomic factors were compared. Risk thresholds, predictive outcomes, and population-specific applicability were systematically reviewed.
Results: The tools varied in their design, risk thresholds, and target populations. The Framingham Risk Score and ASCVD 2018 Risk Estimator are widely used for 10-year CVD risk prediction, whereas tools like JBS3 emphasize lifetime risk, incorporating “heart age” to guide long-term interventions. The Reynolds Risk Score and Astro-CHARM tools introduced novel variables such as inflammatory markers and coronary artery calcium scores, respectively, improving risk stratification for specific populations. Regional tools like China-PAR and PREDICT-CVD were tailored to account for ethnicity and socioeconomic disparities, enhancing accuracy within their respective cohorts.
Conclusion: Despite advancements in cardiovascular risk assessment, no single tool is universally applicable due to population-specific variations and differences in predictive accuracy. A tailored approach, integrating validated tools and patient-specific factors, is essential to improve risk prediction, encourage compliance, and reduce global CVD burden. Clinicians must adopt a holistic strategy incorporating lifestyle and therapeutic interventions to optimize outcomes.
Keywords: Cardiovascular Risk, Framingham Risk Score, ASCVD, SCORE, Reynolds Risk Score, Risk Stratification, Coronary Artery Calcium.
Analyze the Different Cardiovascular Risk Assessment Tools Available.
Introduction
Cardiovascular risk assessment tools are essential for identifying individuals at risk of cardiovascular disease (CVD) and for guiding effective interventions based on validated equations. These tools vary globally and are tailored to specific populations. The Framingham Risk Score (2008), developed from the Framingham Heart Study in the USA, was widely used until the American College of Cardiology and American Heart Association (ACC/AHA) released new cholesterol management guidelines in 2013, incorporating the Pooled Cohort Equations.
In Europe, the SCORE (Systematic Coronary Risk Evaluation) project assessed cardiovascular risk factors and mortality across twelve countries. Similarly, the Joint British Societies (JBS3) developed guidelines in 2014, introducing a lifetime cardiovascular risk estimation tool based on the QRISK model algorithm.
The Reynolds Risk Score (RRS), introduced in 2007 for women and in 2008 for men, predicts multifactorial cardiovascular outcomes, including myocardial infarction, ischemic stroke, coronary revascularization, and cardiovascular death. Other notable projects include the China-PAR (specific to white Mongolian populations in China) and PREDICT-CVD from New Zealand, designed for 5-year ASCVD risk assessment.
Advanced tools such as the Astro-CHARM and imaging calculators have improved risk prediction. Coronary Artery Calcium (CAC) Scoring, developed in the 1980s using computed tomography (CT), has become a cornerstone for predicting cardiovascular events, especially for individuals categorized as intermediate risk after initial assessment.
Methods
This study employed a comprehensive review methodology to evaluate and compare cardiovascular risk assessment tools. Primary sources included peer-reviewed journals, clinical guidelines, and cohort studies, which provided foundational data for tools such as the Framingham Risk Score (FRS), Systematic Coronary Risk Evaluation (SCORE), Reynolds Risk Score (RRS), ASCVD 2018 Risk Estimator, China-PAR, PREDICT-CVD, and the Joint British Societies Risk Calculator (JBS3). Advanced tools incorporating imaging, such as Astro-CHARM and Coronary Artery Calcium (CAC) Scoring, were also included to assess their predictive accuracy for cardiovascular disease outcomes.
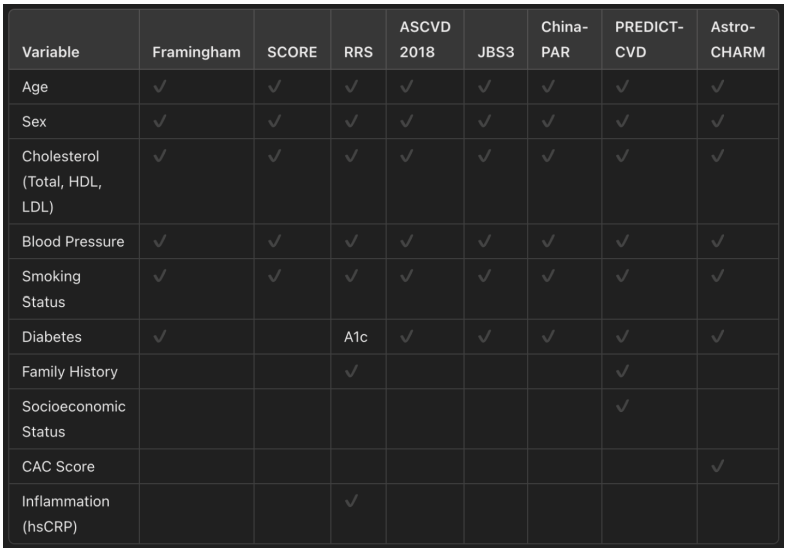
Data sources for the review included published cohort studies from diverse populations across the United States, Europe, Asia, and Oceania, ensuring geographical and ethnic representation. Key variables extracted for analysis were age, sex, blood pressure, cholesterol levels (total, HDL, LDL), diabetes status, smoking history, family history of cardiovascular disease, inflammatory markers (e.g., high-sensitivity C-reactive protein), and socioeconomic factors such as employment status and social deprivation. The tools were assessed for their ability to predict cardiovascular outcomes, including myocardial infarction, ischemic stroke, coronary revascularization, and cardiovascular mortality.
The tools were compared in terms of their risk classification thresholds (low, moderate, and high risk), target population, and predictive accuracy. Risk duration (e.g., 5-year, 10-year, or lifetime risk) was also analyzed to evaluate their clinical applicability. A comparative table summarizing variables, risk thresholds, and specific outcomes for each tool was developed to facilitate a structured comparison. The statistical validity of these tools was reviewed based on reported sensitivity, specificity, and area under the curve (AUC) values from published cohort studies.
Through this process, the review aimed to highlight the strengths, limitations, and population-specific relevance of each cardiovascular risk assessment tool. The findings emphasize the need for tailored approaches in different populations to improve accuracy, intervention strategies, and clinical outcomes.
Resultsae
The evaluation of cardiovascular risk assessment tools revealed significant differences in their design, key variables, predictive outcomes, and target populations. These tools vary in their ability to predict cardiovascular disease (CVD) risk across different demographics, highlighting the importance of population-specific models for accurate risk stratification.
Framingham Risk Score (FRS)
The Framingham Risk Score remains one of the most widely used tools globally for 10-year risk prediction of myocardial infarction (MI), stroke, and cardiovascular death. It incorporates traditional risk factors such as age, sex, blood pressure, cholesterol levels, smoking, and diabetes. However, its limitations include reduced accuracy for younger individuals, older adults (>65), and specific ethnic or social groups.
SCORE (Systematic Coronary Risk Evaluation)
The SCORE tool, developed for European countries, evaluates cardiovascular mortality risk using variables like age, sex, smoking status, cholesterol levels, and blood pressure. By stratifying populations into low- and high-risk categories, SCORE provides clinically relevant guidance for European adults aged 45-64. Its reliance on mortality as the outcome limits its use for non-lethal cardiovascular events.
Reynolds Risk Score (RRS)
The Reynolds Risk Score improves upon traditional risk models by incorporating inflammatory biomarkers such as high-sensitivity C-reactive protein (hsCRP) and family history of premature MI. While hsCRP adds predictive value, its contribution is modest compared to traditional variables. RRS has demonstrated strong accuracy in predicting MI, stroke, revascularization, and cardiovascular death in both men and women.
ASCVD 2018 Risk Estimator
The ASCVD 2018 Risk Estimator, updated by the American College of Cardiology (ACC) and the American Heart Association (AHA), provides a robust 10-year risk prediction for atherosclerotic cardiovascular disease (ASCVD). It considers age, sex, race, cholesterol levels, blood pressure, diabetes, and smoking status. The tool stratifies risk into four categories: low (<5%), borderline (5-7.5%), intermediate (7.5-19.9%), and high (>20%). It emphasizes early therapeutic interventions, particularly for individuals with LDL >190 mg/dL or diabetes.
China-PAR
The China-PAR Risk Equation, tailored for white Mongolian populations in China, demonstrated high accuracy in predicting 10-year ASCVD risk. It uses traditional variables such as age, sex, blood pressure, cholesterol, and smoking. Internal and external validation showed reliable stratification into <5%, 5-9.9%, 10-19.9%, and >20% risk groups, reflecting its suitability for the Chinese population.
JBS3 Risk Calculator
The Joint British Societies (JBS3) Risk Calculator emphasizes lifetime cardiovascular risk, introducing the concept of “heart age” to illustrate the impact of modifiable risk factors. This tool is particularly effective for individuals at low short-term risk but high lifetime risk, enabling early interventions and influencing long-term outcomes.
PREDICT-CVD
The PREDICT-CVD tool, developed in New Zealand, integrates traditional risk factors alongside socioeconomic variables such as ethnicity, employment status, and social deprivation. This holistic approach enhances its predictive accuracy for diverse populations and addresses the impact of social determinants on cardiovascular risk.
Astro-CHARM and Coronary Artery Calcium (CAC) Scoring
The Astro-CHARM tool incorporates coronary artery calcium (CAC) scores into cardiovascular risk prediction, significantly improving accuracy for younger populations (<65 years). CAC scoring, derived from computed tomography, identifies subclinical atherosclerosis and enhances risk stratification, particularly for patients at intermediate risk.
Summary of Findings
- Traditional Tools (e.g., Framingham, SCORE) are widely validated but limited by demographic applicability and reliance on conventional risk factors.
- Advanced Tools (e.g., RRS, Astro-CHARM, CAC) incorporate novel variables like inflammatory markers and imaging results, improving precision for specific populations.
- Population-Specific Models (e.g., China-PAR, PREDICT-CVD) address ethnic and socioeconomic factors, enhancing accuracy in targeted cohorts.
- Lifetime Risk Tools (e.g., JBS3) focus on long-term outcomes, promoting early interventions.
Table 1: Overview of Cardiovascular Risk Assessment Tools
Table 2: Comparison of Risk Categories in Tools
Table 3: Variables Considered in Cardiovascular Risk Tools
Discussion
Framingham Risk Score
The Framingham Risk Score remains a widely used tool incorporating variables like age, sex, smoking, diabetes, cholesterol levels, and systolic blood pressure. It categorizes individuals into risk groups to guide preventive interventions. Despite its utility, the Framingham Score has limitations:
- It excludes certain cardiovascular outcomes.
- It may be unreliable for specific ethnic and social groups.
- It is less accurate for individuals under 30 or over 65 years old.
ATP III Hard CHD Risk Score
The Adult Treatment Panel (ATP III), introduced in 2002, builds upon Framingham's model to estimate 10-year cardiovascular risk. It influenced statin therapy recommendations, particularly for individuals with a risk score ≥7.5%, while improving predictability by incorporating stroke outcomes.
Updated Guidelines (2018)
ACC/AHA cholesterol management guidelines addressed intermediate and low-risk individuals whose risks were underestimated. New factors included:
- Chronic Kidney Disease (CKD)
- Primary hypercholesterolemia
- Metabolic syndrome
- Chronic inflammatory conditions
The ASCVD 2018 Risk Estimator Plus stratifies individuals based on 10-year risk:
- Low (<5%)
- Borderline (5-7.5%)
- Intermediate (7.5-19.9%)
- High (>20%)
It emphasizes therapy initiation for individuals with LDL >190 mg/dL or between 70-190 mg/dL with diabetes.
SCORE Project
SCORE evaluates cardiovascular mortality risk across Europe by analyzing data from 205,178 individuals aged 45-64. It divides populations into low-risk and high-risk groups and is adaptable for nations lacking cohort studies using national mortality data.
JBS3 Risk Calculator
The JBS3 tool estimates lifetime cardiovascular risk, emphasizing “heart age” and demonstrating the long-term benefits of early intervention. It identifies individuals with low short-term but high lifetime risk, influencing sustainable risk reduction strategies.
Reynolds Risk Score (RRS)
The RRS incorporates additional risk factors, such as:
- Family history of premature myocardial infarction (before 60 years).
- Hemoglobin A1c (diabetics only).
- High-sensitivity C-reactive protein (hsCRP), a biomarker for inflammation.
While hsCRP's contribution is modest compared to traditional risk factors, it remains validated in multiple studies.
China-PAR and PREDICT-CVD The China-PAR Risk Equations were validated through 21,000 white Mongolian participants over 12 years. It stratifies 10-year ASCVD risk into <5%, 5-9.9%, 10-19.9%, and >20%.
The PREDICT-CVD tool incorporates socio-demographic factors (e.g., employment status, social deprivation) alongside traditional variables, enabling detailed risk stratification.
Astro-CHARM and CAC Scoring
The Astro-CHARM tool integrates Coronary Artery Calcium (CAC) scores, further refining cardiovascular risk prediction. CAC scoring is particularly effective in identifying individuals under 65 requiring early statin therapy.
Conclusion
Cardiovascular risk assessment tools have advanced significantly, yet global challenges persist. Many tools lack universal applicability due to population-specific variations and limited comprehensiveness in predicting outcomes. Furthermore, some individuals at risk struggle with risk factor management despite years of intervention.
To improve cardiovascular outcomes, healthcare systems must adopt tailored risk assessment models suited to their populations. Clinicians should use a holistic approach, emphasizing patient education, communication, and interventions such as diet and lifestyle modifications to enhance compliance and reduce cardiovascular morbidity and mortality rates.
Reference
Ardern, C.I., et al. (2005). ‘Revised Adult Treatment Panel III Guidelines and Cardiovascular Disease Mortality in Men Attending a Preventive Medical Clinic’ Circulation 112, 1478–1485. [Online] available at: https://doi.org/10.1161/CIRCULATIONAHA.105.548198 (accessed on 24 September 2021)
D’Agostino, et al., (2001). ‘Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation’. JAMA 286, 180–187. [Online] available at: https://doi.org/10.1001/jama.286.2.180 (accessed on 24 September 2021)
Mahmood, S et al (2013)' The lancet' The Framingham Heart Study and the Epidemiology of Cardiovascular Diseases: a Historical Perspective 383 (9921) (Online). Available at:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4159698/. accessed 15 September 2021.
Brindle, P et al. (2005) ‘British Journal of Medical Practice’ The accuracy of the Framingham risk-score in different socioeconomic groups: a prospective study 55 (520) (Online). Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1570792/. Accessed 16 September 2021.
Conroy, R.M., Pyörälä, K., Fitzgerald, A.P., et al. (2003) ‘Estimation of Ten-Year Risk of Fatal Cardiovascular Disease in Europe: the SCORE Project’, European Heart Journal, 24(11), pp. 987-1003. Oxford Academic [Online]. Available at: https://academic.oup.com/eurheartj/ (Accessed: 20 September 2021)
Rücker, V., Keil, U.et al. (2016) ‘Predicting 10-Year Risk of Fatal Cardiovascular Disease in Germany: An Update Based on the SCORE-Deutschland Risk Charts’, PLos One 11(9). PubMed Central [Online]. Available at: https://pubmed.ncbi.nlm.nih.gov/ (Accessed: 20 September 2021)
Ridker,P. Buring,J. Rifai,N et al. 2007. Development and Validation of Improved Algorithms for the Assessment of Global Cardiovascular Risk in Women: The Reynolds Risk Score. Available from: https://jamanetwork.com/journals/jama/article-abstract/205528. [15 September 2021].
Cook,N. paynter,N. Eaton,C. et al. 2012. Comparison of the Framingham and Reynolds Risk Scores for Global Cardiovascular Risk Prediction in the Multiethnic Women's Health Initiative. AHA Journals. Available from: https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.111.075929. [14 September 2021].
Blaha,J. Rivera,J. Budoff,J et al. 2011. Association between obesity, high-sensitivity C-reactive protein ≥2 mg/L, and subclinical atherosclerosis: Implications of JUPITER from the Multi-Ethnic Study of Atherosclerosis. AHA Journals. Available from: https://www.ahajournals.org/doi/full/10.1161/ATVBAHA.111.223768. [18 September 2021].
Deanfield, J., Sattar, N., Simpson, et al. (2014) 'Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3)', Heart (British Cardiac Society), 100(Suppl 2), pp. ii1-ii67.
Mohan J., Bhatti K., Tawney A., Zeltser R. (2021) ‘Coronary Artery Calification’ [online] Available at: https://www.ncbi.nlm.nih.gov/books/NBK519037/ (Accessed on September 23rd 2021)
Khera A., Budoff M., O’Donnell C., et al (2018) ‘ Astronaut Cardiovascular Health and Risk Modification (Astro-CHARM) Coronary Calcium Atherosclerotic Cardiovascular Disease Risk Calculator’ Circulation, American Heart Association Journal 138 (17) pp 1819-1827 [Online] Available at : https://doi.org/10.1161/CIRCULATIONAHA.118.033505 (Accessed on: 23rd September 2021)
GoffJr D., Lloyd-Jones D., Bennett G., et al (2013) ‘2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk’ Circulation, American Heart Association Journal [Online] 129(25) pp S49-S73 Available at: https://doi.org/10.1161/01.cir.0000437741.48606.98 (Accessed on: 23rd September 2021)
Xueli Yang, et al. (2016) ‘Predicting the 10-Year Risks of Atherosclerotic Cardiovascular Disease in Chinese Population: The China-PAR Project (Prediction for ASCVD Risk in China)’ Circulation; 134: 1430–1440, [Online] available at: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.116.02236, (accessed on 24 September 2021).
Ni Mei Zeng, et al (2018) ‘Validation of the China-PAR Equations for Cardio-cerebrovascular Risk Prediction in the Inner Mongolian Population’ Biomedical and Environmental Sciences 31(6): 463-466 [Online] available at: www.besjournal.com/en/article/doi/10.3967/bes2018.061 (accessed on 24 September 2021).