Expanding Horizons with Combined Radio-Frequency Ablation and Erector Spinae Plane Catheter for Thoracic Vertebral Fracture in Multiple Myeloma Patient
Expanding Horizons with Combined Radio-Frequency Ablation and Erector Spinae Plane Catheter for Thoracic Vertebral Fracture in Multiple Myeloma Patient
Dr Neha Kanojia *, Dr. SK Gupta
1. DR NEHA KANOJIA , MD (Anaesthesia)- University Of Delhi
EDRA- Esra Board, Switzerland
FIPM- Kamineni Hospital, Hyderabad
Fellowship in Chronic Pain, Fellowship in Perioperative Anaesthesia- University Of Toronto, Canada
2. DR SK GUPTA, MBBS, MD, DM (Clinical Haematology)- AIIMS, Delhi
Fellowship Leukemia/Bmt/Car-T Cells, UBC, Canada
*Correspondence to: Dr Neha Kanojia, Continental Hospitals, IT and Financial District, Gachibowli, Hyderabad- 500032, India.
Copyright.
© 2025 Dr Neha Kanojia This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 December 2024
Published: 06 January 2025
Abstract
A 71 years old male patient diagnosed case of multiple myleoma was suffering from severe back pain due to thoracic vertebral fracture. He underwent Radio frequency ablation of the thoracic facets along with Erector spinae plane catheter insertion for pain and palliation. The patient responded to this treatment modality and shows that combined technique could be useful for better pain management.
Keywords: Thoracic facets, vertebral fracture, Radio-frequency ablation, Erector spinae plane catheter
Expanding Horizons with Combined Radio-Frequency Ablation and Erector Spinae Plane Catheter for Thoracic Vertebral Fracture in Multiple Myeloma Patient
Introduction
Multiple myeloma is a malignant plasma cell disorder characterized by proliferation of plasma cells in the bone marrow that leads to osseous destruction.It is characterized by pathological fractures in 30% cases substantially reducing quality of life due to back pain and functional limitation (1). The facet or zygapophysial joints of the spine are well innervated by the medial branches of the dorsal rami and these facet joints can be a significant source of pain in compression fractures (2).
We describe here a novel technique of combined Radio frequency ablation (RFA) of the facet joints above, below and at the level of compression fracture along with Erector spinae plane (ESP) block with catheter for palliative care who are not candidates for other interventional treatments.
Case Report
A 71 years old man with history of active Multiple myleoma was admitted with complaints of severe back pain on movements. He was unable to turn side ways and to get up from the bed. He was receiving chemotherapy for the same. Past history was significant for hypertension, Coronary artery disease on medical management, hypothyroidism. He was on Fentanyl transdermal patch 50 mcg every third day, Intravenous Morphine 3 mg SOS, Zolendronic acid, tablet Tramadol and paracetamol combination twice daily. On clinical examination, patient was having a pain score on NRS 8-9/10. On palpation, tenderness was elicited over the area corresponding to D8 level over the midline and right paraspinal region in the thoracic back. The pain was not radiating to bilateral upper limbs, anterior chest wall or lower limbs and no motor or sensory deficits were noticed. His MRI Spine revealed multiple wedge compression fractures at D5, D8, D10 levels (Fig1)
Fig- 1. MRI SPINE saggital section showing D8 vertebral fracture
However in comparison to the previous MRI, D8 fracture was relatively new but there was no underlying marrow oedema.
After thorough examination and imaging review, we decided to proceed with the radiofrequency ablation of the medial branch nerves supplying the facet joints of bilateral D7-D9 vertebral levels along with ESP block with catheter on the right side at D7 level.
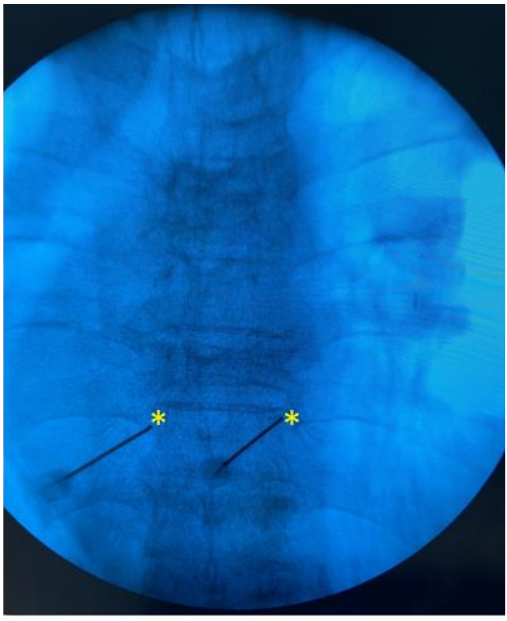
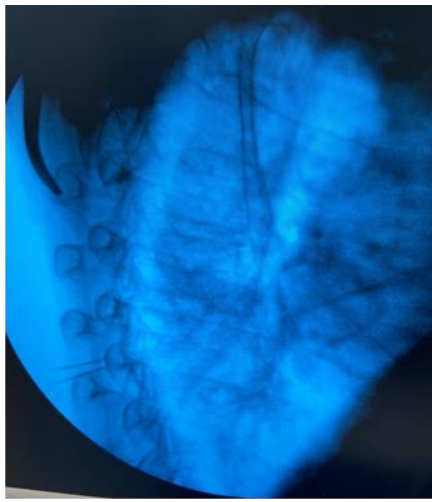
Pre anesthestic checkup was done and consent taken before the procedure. Patient was positioned in the prone position with a pillow underneath the chest and arm by the side. Standard anesthesia monitors were applied. Fluoroscopy was used to identify the right level, counting up from the 12th vertebral body. Target was the supero-lateral aspect of the Transverse process of the vertebra, for the radiofrequency ablation of the medial branches. Adequate caudal and contralateral oblique tilt was given to position the fluoroscope beam parallel to the targeted nerve. 20 G, 10 cm RF cannula ,10 mm curved tip (Boston scientific, USA), were advanced to the target sites in a parallel manner after anesthetizing the skin by lidocaine 2%. (Fig 2) Another two RF cannuale were inserted at T8 and T9 levels in a similar fashion. True lateral views were taken to ensure proper depth of all needles (Fig. 3). The stylets were withdrawn and radiofrequency probes were inserted. At all levels, sensory stimulation at 0.5 V, 50Hz and motor stimulation at 2 Hz up to 1.5 V/2V were obtained. After Iv sedation, two Radio-frequency lesions were done at 80 degrees Celsius for 90 seconds 2mm apart. 10 mg of methylprednisolone in 1ml lidocaine 2% was injected ta each level to prevent post-ablation neuritis. The same procedure was repeated at the same levels on the other side.
Fig 2 - RF needle placement over the super-lateral aspect of the Transverse process.
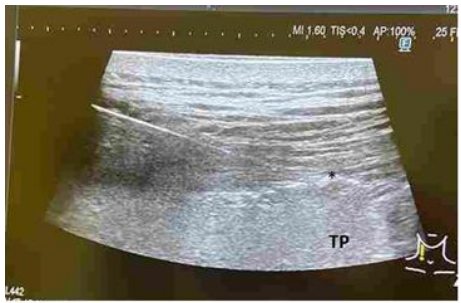
For ESP block , a linear high frequency transducer (Fujifilm, Arette, Germany) was prepped in a sterile fashion and right T7 transverse process was visualized in a longitudinal manner. 17 G epidural Tuohy needle was inserted in plane from cephalo - caudal manner till the tip of the needle touched the Transverse process of T7. (Fig 4,5)The ESP was distended with 10 ml Normal saline followed by 15 ml 0.25 % bupivacaine and 25 mcg Fentanyl. 18 g Epidural catheter was then inserted in to the plane and fixed at 13 cm and connected with an elastometric pump (230 ml 0.2% Ropivacaine and 200 mcg Fentanyl) for three days at a rate of 4-6 ml per hour infusion through the catheter. His immediate NRS scores were 1/10.
Fig 3 - Lateral view. Needle depth over the TP
Fig 4 Tuohy needle insertion for ESP block at T7
Fig 5 In plane needle insertion at T7 TP. * represents ESP
No complications were noted. Fentanyl patch was removed and his medications gradually came down in a couple of days post operatively.
The NRS scores were 1/10 in the follow up period after 4 weeks and 3 months.
Discussion
The pathogenesis of back pain in cancer patients is multifactorial, resulting from combination of local release of pro-inflammatory cytokines, vertebral body instability causing compression of the spinal cord or the nerve roots leading to neuropathic pain. (3)
Anterior wedge compression fractures increases the stress on facet joints leading it to be a significant pain generators. (2)
Vertebral fractures can be treated by vertebroplasty and kyphoplasty, however not all patients are candidates for these procedures, especially pain arising from the posterior elements (lamina & facet joints), particularly the joints above and below the wedge compression fractures. (4)
In those cases, less invasive treatment approaches such as RFA of the painful facet joints offer better pain control, reduces the recovery period and lower morbidity and mortality. (5)The disruption of the sensory nerve fibres supplying the periosteum, seem to be the cornerstone of its effectiveness in pain control.
In various studies, painful osteolytic bone metastasis were treated by radiofrequency of the lesions leading to successful pain management and decreased opioid consumption.(6,7)
Erector spinae plane block has emerged as an analgesic technique for the treatment of both acute and chronic pain with good results.(8,9) The versatility of this block can be extrapolated to the patients having pathological oncological vertebral fractures not amenable to other interventional options ( 10)
Conclusion
Thoracic facet joints may be pain generator in vertebral compression fractures, secondary to biomechanically induced thoracic flexion moment. The advantages of the combined procedure are low complications, short procedural duration, reduced patient discomfort, lower need for analgesics and better quality of life.
References
1. Rajkumar SV. Plasma cell disorders. In: Goldman's cecil medicine. 24th ed. Edited by Goldman L, Schafer AI. Philadelphia (PA), Elsevier Saunders. 2012, pp 1237-40
2. Mitra R,Do H,Alamin T et al. Facet pain in thoracic compression fractures. Pain Med. 2010 Nov;11(11):1674-7.
3. Giammalva, G.R.; Costanzo, R.; Paolini, F.; Benigno, U.E.; Porzio, M.; Brunasso, L.; Basile, L.; Gulì, C.; Pino, M.A.; Gerardi, R.M.; et al. Management of Spinal Bone Metastases with Radiofrequency Ablation, Vertebral Reinforcement and Transpedicular Fixation: A Retrospective Single-Center Case Series. Front. Oncol. 2022, 11, 5896
4. Proschek, D.; Kurth, A.; Proschek, P.; Vogl, T.J.; Mack, M.G. Prospective Pilot-study of Combined Bipolar Radiofrequency Ablation and Application of Bone Cement in Bone Metastases. Anticancer Res. 2009, 29, 2787–92.
5. Bagla, S.; Sayed, D.; Smirniotopoulos, J.; Brower, J.; Neal Rutledge, J.; Dick, B.; Carlisle, J.; Lekht, I.; Georgy, B. Multicenter Prospective Clinical Series Evaluating Radiofrequency Ablation in the Treatment of Painful Spine Metastases. Cardiovasc. Interv. Radiol. 2016, 39, 1289–97.
6. Gharaei H, Imani F, Vakily Masoud. Rdaiogrequency thermal ablation in painful myeloma of the clavicle. Korean J Pain.201;Vol 27,1:72-6
7. Cédric Cirenei, Pierre Boussemart, Benoit Tavernier. Bilateral Erector Spinae Plane Block in the Management of Thoracic Spine Fracture: A Case Report Erector Spinae Plane Block for Spine Fractures. Biomed J Sci & Tech Res 42(2)- 2022. BJSTR. MS.ID.006719.
8. Glunic V, Bonasera L, Gonzalez S et al. Combination of the T7 unilateral Erector spinae pane block and T10 bilateral retro laminar blocks in a patient with multiple rib fractures on the right and T10-12 vertebral compression fractures: a case report. Local Reg Anesth 2021,14;99-102
9. Kanojia N, Basvanapalli AR, Chagalakonda V, Sekhar B. Efficacy of ultrasound guided bilateral single shot erector spinae plane block for post?operative analgesia in patients undergoing lumbar spine surgery. Indian J Pain 2020;34:202
10. Castillo Ramirez L, Guillen Nuñez M, Jùarez Lemus À, et al. Effectiveness of Erector Spinae Muscle Block in Vertebral Oncologic Fracture. Cureus 202416(3): e55599. DOI 10.7759/cureus.5559