Mafld a New Emerging Liver Disease
Mafld a New Emerging Liver Disease
Dr. Salvatore Stefano Sciarrone1* , Dr.ssa Lucia Fini2, Dr. Luca De Luca3
1,2. Gastroenterology and endoscopy unit, Department of Surgery, San Carlo University Hospital, Milan University-ASST San Carlo e Paolo , Milan Italy.
3. Chief of Gastroenterology, Gastroenterology and endoscopy, Department of Surgery, San Carlo University Hospital Milan University-ASST San Carlo e Paolo, Milan Italy
*Correspondence to: Dr. Salvatore Stefano Sciarrone MD, Gastroenterology and endoscopy Unit, Department of Surgery, San Carlo University Hospital, Milan University-ASST Santi Paolo e Carlo , Milan Italy.
Copyright
© 2025 Dr. Salvatore Stefano Sciarrone, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 February 2025
Published: 15 February 2025
DOI: https://doi.org/10.5281/zenodo.15140107
Abstract:
Nonalcoholic fatty liver disease (NAFLD), affecting about 25% of general population and more than 50% of dysmetabolic patients, is an emerging cause of chronic liver disease and its complications. Recently, an international consensus of experts proposed to rename this disease as 'Metabolic dysfunction-Associated Fatty Liver Disease' (MAFLD) to focus on the bidirectional interplay between fatty liver and metabolic alterations and to stress the need of assessing fatty liver independently from alcohol consumption and other coexisting causes of liver disease. The peculiarity of NAFLD/MAFLD lies in the presence of a higher risk of not only - as expected - liver-related events but also of extrahepatic events, mostly cardiovascular and cancers. Available evidence suggests that these associations are not only the expression of sharing the same risk factors but shed light about the ability of NAFLD/MAFLD and particularly of its progressive form - nonalcoholic/metabolic dysfunction-associated steatohepatitis - to act as an independent risk factor via promotion of atherogenic dyslipidemia and a proinflammatory, profibrogenic, and procoagulant systemic environment. The present review summarizes available epidemiological and clinical evidence supporting the concept of NAFLD/MAFLD as a multisystemic disease, and highlights potential explanatory mechanisms underlying the association between NAFLD/MAFLD and extrahepatic disorders.
Key words: metabolism, Steatosis, Multysistemic, dislypidemia, Extrahepatic.
Mafld a New Emerging Liver Disease
Core Tips
In the last 10 years, with the advent of Direct antiviral (DAA) to eradicate Hepatitis C (HCV) and with a better control of Hepatitis B (HBV), a new era is beginning, that regard not only hepatologist but also diabetologist and bring us the need to work in team.
Metabolic associated fatty liver disease is increasing avoid population, so we need to understand phatholgy underneath the disease to find non-invasive test to evaluate the course of this disease.
Main Text
The worldwide spread of obesity and diabetes, the prevalence of NAFLD and its complications is increasing. Recent cohort studies reported a very high prevalence of NAFLD – from 25% in general population to 50–60% in obese and diabetic patients – with an estimated increase in 2030 ranging from +11.3% in Germany to +12% in Spain.4–6 When considering the new definition, a recent meta-analysis showed that MAFLD affects more than a third of the global population with and estimated global MAFLD prevalence of 50.7%, specifically in overweight and obese adults, with a higher prevalence in male than female (59.0% versus 47.5%).7,8
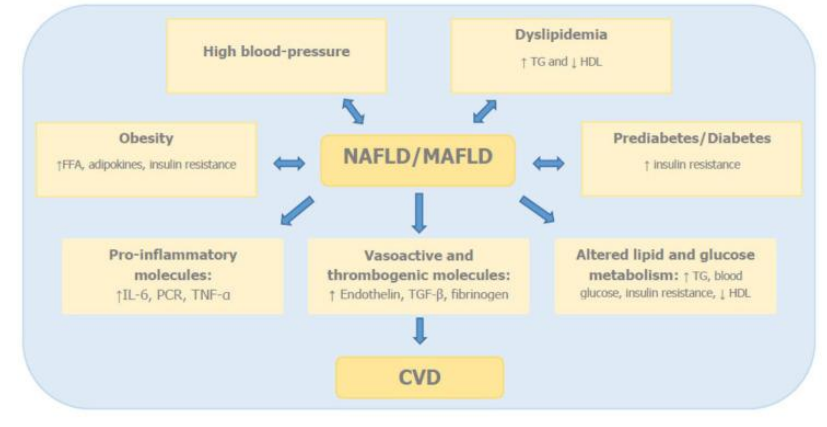
Various studies clearly demonstrated that NAFLD and MAFLD patients have not only a higher risk of hepatic events but also of extrahepatic complications mostly cardiovascular disease (CVD) and extrahepatic cancers, suggesting that NAFLD/MAFLD is part of a multisystemic disease and identifying in the severity of liver fibrosis the most relevant prognostic factor. In addition, different studies conducted to compare NAFLD and MAFLD highlighted that differences exist between the two entities on identifying patients at high risk of progression and of extrahepatic complications.
To evaluate the severity of the disease, as the authors explain, we have a lot of instruments as:
Lipidic assect (with related panels derived from these biochemical indicators are also
subject to low accuracy and specificity, such as fatty liver index for hepatic steatosis, and Bayesian Argumentation via Delphi score (body mass index, AST/ALT ratio, and presence of diabetes) for hepatic fibrosis, BMI (the aid of artificial intelligence makes it more and more accurate) and Current imaging-based biomarkers have poor diagnostic performance for steatohepatitis, especially distinguishing steatohepatitis from fibrosis. Ultrasound-based measurements of liver stiffness by vibration-controlled transient elastography (VCTE), commercially marketed as FibroScan, have demonstrated very good diagnostic accuracy for advanced fibrosis. Likewise, magnetic resonance elastography (MRE) shows low failure rate in diagnosis of advanced fibrosis. More importantly, MRE outperforms VCTE in diagnostic accuracy for earlier stages of fibrosis Liver Biopsy is avoided to staging steatosis, because the risks that are less than benefit, and because we need instrument to evaluate not only the liver but also the general state of the patients.
To control the situation is important the collaboration between different figure (diabetologist, Hepatologist) to figure out the risk of progression and for the surveillance of hepatocarcinoma, that could occur also if the patients is not in cirrhosis.
Statins (atorvastatin) is fundamental, in fact they demonstrate an anti-fibrogenesis action and an anti-inflammatory action that could make the disease go slowly.
So we think that is fundamental to have some non-invasive test to evaluate the patients globally.
Figure 1
Conclusion
From this consideration is fundamental to use non-invasive technique (we have illustrated it ) to follow up the pathology. Moreover, the most important things, is the education of the patience, and the explanation of his condition. We are moving to an era where the collaboration between different disciplines and the relation with patients will be fundamental to cure and prevent complications.
Author contributions: Dr. Luca De Luca, Dr.ssa Lucia Fini and Dr. Salvatore Stefano Sciarrone contribute equally to write this manuscript.
Conflict of Interest: None