The Evolution of Gallbladder Drainage: From Surgery to Endoscopic Ultrasound-Guided Techniques
The Evolution of Gallbladder Drainage: From Surgery to Endoscopic Ultrasound-Guided Techniques
Carson Creamer, D.O.1,2*, Mohammed Janajri, M.D.1, Bahar Rehan M.D.1,2, Kobina Essilfi-Quaye M.D.1,2, Mohhamad Abu Asi M.D.1,2, Yeshika Thapa M.D.1,2, Neeka Akhavan, M.D.3, Yaseen Perbtani, D.O.1,2, Tony Brar, M.D1,2
1.University of Central Florida College of Medicine, University of Central Florida, Orlando, Florida, USA.
2. HCA Florida North Florida Hospital, Graduate Medical Education Internal Medicine Residency Program, Gainesville, Florida, USA
3. The University of Florida College of Medicine, University of Florida, Gainesville, Florida, USA.
*Correspondence to: Carson Creamer; University of Central Florida College of Medicine, University of Central Florida, Orlando, Florida, USA.
Copyright
© 2025 Carson Creamer, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 February 2025
Published: 28 February 2025
DOI: https://doi.org/10.5281/zenodo.15140331
Abstract
The management of gallbladder disease has evolved from open cholecystectomy to minimally invasive approaches like laparoscopic cholecystectomy and endoscopic ultrasound-guided gallbladder drainage (EUS-GBD). For high-risk surgical candidates, percutaneous transhepatic gallbladder drainage (PT-GBD) has been an alternative option, though it presents limitations such as catheter dislodgement and reduced quality of life. EUS-GBD has emerged as a highly effective solution, offering internal drainage through transmural approaches. The use of lumen-apposing metal stents (LAMS) has further refined the procedure, enhancing safety, technical success, and clinical outcomes. This article provides a historical perspective on gallbladder disease management while highlighting the evolution and clinical impact of EUS-GBD.
The Evolution of Gallbladder Drainage: From Surgery to Endoscopic Ultrasound-Guided Techniques
Introduction
Gallbladder disease, including conditions like biliary colic, calculous cholecystitis, and acalculous cholecystitis, significantly impacts healthcare in the United States, affecting approximately 10%–15% of US adults. Acute cholecystitis, a common complication of gallstone disease, affects 1% to 4% of Americans and increases in prevalence with age. If untreated, acute cholecystitis can lead to severe complications such as gangrene, perforation, and septic shock. These episodes can increase readmission rates, hospitalization lengths, and overall health-related costs while diminishing patients’ quality of life. (1)
Cholecystectomy is the preferred treatment for symptomatic gallbladder disease; however, many patients are high-risk surgical candidates due to comorbidities, malignancy, underlying cirrhosis, or severe cardiac disease. For these individuals, less invasive alternatives are essential. Historically, Percutaneous transhepatic gallbladder drainage (PT-GBD) was performed to decompress the gallbladder in acute cholecystitis patients at high risk for cholecystectomy. Gallbladder drainage becomes a critical intervention to resolve gallbladder inflammation and prevent further complications in these patients. (1)
Transpapillary approach via Endoscopic Retrograde Cholangiopancreatography (ERCP) first emerged as a transformative development, offering a minimally invasive alternative to percutaneous and surgical techniques. (2) Later, EUS-GBD was introduced and involves creating a drainage pathway from the gallbladder to the gastrointestinal tract under endoscopic ultrasound guidance. This can be achieved through either a transmural approach, creating a cholecysto-gastric or cholecystoduodenal fistula. (2)
Historical Perspective on Gallbladder Disease Management
A. Early Surgical Approaches
Open cholecystectomy, first performed by Carl Langenbuch in 1882, was once the standard treatment for gallbladder pathology. It remains a viable surgical option, especially in complex cases or when minimally invasive surgery is contraindicated. However, it carries higher morbidity and mortality in high-risk patients. (3) Several factors, including advanced age and significant comorbidities, contribute to these poor outcomes, with open cholecystectomy mortality rates were reported as high as 2.9% compared to 0% for laparoscopic cholecystectomy. (3)
B. Introduction of Laparoscopic Cholecystectomy
Laparoscopic cholecystectomy, introduced by Philippe Mouret in 1987, revolutionized gallbladder surgery by reducing postoperative pain, hospital stay, and complications. (3) Early adoption was rapid due to clear benefits over open surgery, and by the early 1990s, laparoscopic cholecystectomy became the gold standard for symptomatic cholelithiasis and mild-to-moderate acute cholecystitis. (4,5) Despite an initial learning curve and skepticism, its success was driven by developments in laparoscopic instrumentation, operative cholangiography, and advanced surgical techniques. (6)
C. The Need for Non-Surgical Drainage Solutions
Non-surgical drainage options were necessitated by patients deemed too high risk for surgery. PT-GBD, first described in the 1970s, is one such intervention, offering gallbladder decompression with reported success rates of around 90%. (6) Nevertheless, PT-GBD can lead to significant adverse events (up to 25% of cases) including catheter dislodgement, infection, and quality-of-life concerns related to external drainage tubes. (2,7)
The Rise of Endoscopic Gallbladder Drainage
A. Early Attempts at Endoscopic Gallbladder Drainage - Endoscopic transpapillary gallbladder drainage (ET-GBD)
Driven by the need for less invasive alternatives to PT-GBD in high-risk patients, early endoscopic gallbladder drainage focused on ERCP-based strategies like transpapillary stenting. ET-GBD is performed during ERCP by selectively cannulating the cystic duct and placing a plastic stent for internal drainage. (2) Although ET-GBD achieves a technical success rate of about 84% and clinical success of 91%, (2) its effectiveness may be reduced by obstructing pathology—such as stones, strictures, or masses—in the cystic duct. (6) Additionally, ET-GBD does not allow for direct treatment of gallstones and may require repeated stent exchanges if migration or occlusion occurs. (7) In some patients, however, ET-GBD can be considered when they also require ERCP for other indications or have large-volume ascites or coagulopathy, as transpapillary drainage may be safer in these specific scenarios. (2)
B. Emergence of EUS-Guided Gallbladder Drainage (EUS-GBD)
EUS-GBD has emerged as a significant alternative to PT-GBD for high-risk surgical candidates, particularly with the introduction of lumen-apposing metal stents (LAMS).
EUS-GBD was first described in 2007 using a nasobiliary catheter. The technique has evolved significantly over the past two decades, driven by the need for less invasive and more effective drainage solutions for patients with acute cholecystitis who are not candidates for surgery. (8)
LAMS were introduced to address the limitations of earlier stents, such as pigtail plastic stents and biliary self-expandable metal stents, which had issues with leakage, migration, and occlusion. LAMS are designed with large flanges and short lengths, reducing the risk of these complications and allowing for the passage of gallstones or an endoscope for therapeutic cholecystoscopy. (2)
Current State of EUS-Guided Gallbladder Drainage
A. Advances in Technique and Technology
The current state of EUS-GBD has seen significant advancements, particularly with the introduction of electrocautery-enhanced lumen-apposing metal stents (EC-LAMS). These innovations have improved procedural efficiency and patient outcomes.
EC-LAMS have revolutionized EUS-GBD by integrating an electrocautery tip with the stent delivery system, allowing for a one-step procedure. This eliminates the need for multiple device exchanges and reduces procedural time. Studies have shown that EC-LAMS achieve high technical success rates of around 94.8% and clinical success rates of 100% in high-risk patients with acute cholecystitis. (12) The American Gastroenterological Association (AGA) highlights that the direct method using EC-LAMS can be performed solely under EUS guidance, further simplifying the procedure and enhancing safety. (2)
Moreover, EUS-GBD provides direct access to the gallbladder, enabling stone removal with lithotripsy and baskets under direct endoscopic cholecystoscopy. This direct approach not only facilitates effective stone management but also reduces the need for additional procedures.
EC-LAMS have been associated with fewer adverse events compared to traditional methods. A systematic review and meta-analysis found that EUS-GBD with EC-LAMS had lower rates of adverse events, recurrent cholecystitis, and hospital readmissions compared to PT-GBD. (13) Additionally, EC-LAMS have been shown to maintain effective gallbladder drainage with minimal adverse events during long-term follow-up. (12)
Figure 1. Endoscopic ultrasound (EUS) of the gallbladder. Courtesy of Tony Brar, M.D.
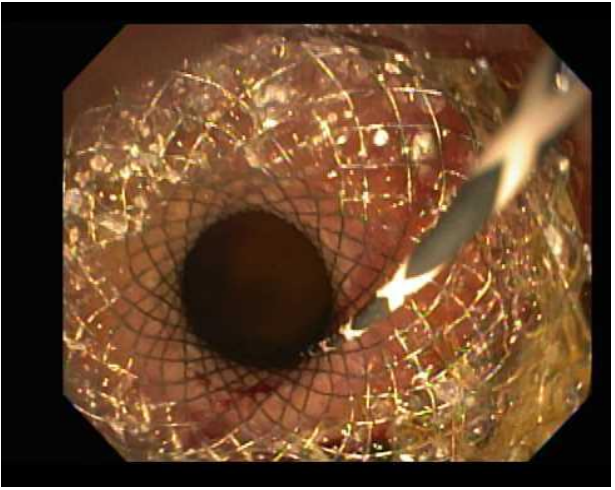
Figure 2. Endoscopic image showing an endoscopic ultrasound-guided LAMS deployed from the stomach to the gallbladder. Courtesy of Tony Brar, M.D.
Figure 3. EUS confirmation of the stent from the stomach to the gallbladder. Courtesy of Tony Brar, M.D.
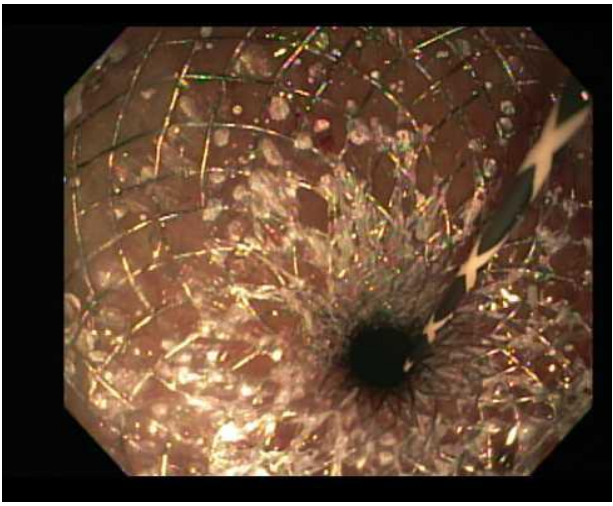
Figure 4. Endoscopic image showing the fully expanded lumen-apposing metal stent (LAMS) following balloon-assisted dilation, ensuring optimal drainage from the gallbladder to the stomach. Courtesy of Tony Brar, M.D.
B. Comparative Outcomes: EUS-GBD vs. PT-GBD
EUS-GBD with LAMS has shown superior outcomes compared to PT-GBD in several key areas.
EUS-GBD with LAMS boasts very high technical success rates ranging from 90% to 98.7% and clinical success rates from 89% to 98.4%. (2) A multicenter study reported technical success rates of 98% for EUS-GBD and 100% for PT-GBD, with clinical success rates of 96% and 91%, respectively. (9)
Patients undergoing EUS-GBD experience significantly lower post-procedural pain scores compared to those undergoing PT-GBD. One study reported mean post-procedural pain scores of 2.5 for EUS-GBD versus 6.5 for PT-GBD (P < .05). (9)
EUS-GBD is associated with fewer repeat interventions. The average number of repeat interventions per patient was significantly lower in the EUS-GBD group (0.2 ± 0.4) compared to the PT-GBD group (2.5 ± 2.8) (P < .05). (9) Another meta-analysis confirmed that EUS-GBD had significantly fewer reinterventions and unplanned readmissions compared to PT-GBD. (14)
Patients treated with EUS-GBD have shorter hospital stays. One study reported an average hospital stay of 3 days for EUS-GBD compared to 9 days for PT-GBD (P < .05). (9) This finding is supported by a systematic review and meta-analysis, which found that EUS-GBD patients had significantly shorter hospital stays. (14) Table 1 below.
Table 1. Key Comparative Outcomes for EUS-GBD vs. PT-GBD
|
Parameter |
EUS-GBD (Approx. Range/Value) |
PT-GBD (Approx. Range/Value) |
Reference(s) |
|
Technical success |
90%–98.7% |
90%–100% |
(2,9,10,14) |
|
Clinical success |
89%–98.4% |
~91% |
(9,10,14) |
|
Hospital stay |
3 days |
9 days |
(9) |
|
Postprocedure pain score |
2.5 |
6.5 |
(9) |
|
Reinterventions (mean) |
0.2 ± 0.4 |
2.5 ± 2.8 |
(9) |
C. Multidisciplinary Approach to Patient Selection
A collaborative approach among gastroenterologists, interventional radiologists, and surgeons is essential to determine whether EUS-GBD or PT-GBD is most appropriate. Gastroenterologists assess the feasibility of EUS-GBD by considering patient comorbidities, the anatomical relationship between the gallbladder and GI tract, and contraindications like gallbladder perforation. Interventional radiologists perform PT-GBD for patients with large-volume ascites or coagulopathy, or when immediate decompression is needed and EUS expertise is not available. Surgeons oversee long-term management, deciding on definitive surgery or continued drainage once a patient is stabilized.
EUS-GBD typically provides higher technical and clinical success rates, lower post-procedural pain, fewer re-interventions, and shorter hospital stays. It is especially suitable for patients with in-dwelling, uncovered metal biliary stents, malignant cystic duct obstruction, or extensive cholelithiasis. PT-GBD remains important in centers without EUS capability or when contraindications exist. Overall, this multidisciplinary approach maximizes outcomes by aligning patient-specific factors with the optimal drainage strategy.
Challenges and Barriers to Overcome
EUS-GBD offers several advantages over PT-GBD, but its adoption faces challenges and barriers, particularly related to specialized training and variability in healthcare settings.
EUS-GBD requires advanced endoscopic skills and training, which limits its availability to high-volume centers with expertise in biliary disease and interventional EUS. The AGA notes that achieving competency in EUS-GBD typically requires performing approximately 19 to 25 procedures, with initial training often involving the use of LAMS for pancreatic fluid collections before progressing to gallbladder drainage. (2) This learning curve and the need for specialized training can be significant barriers to widespread adoption.
The adoption of EUS-GBD varies significantly across different healthcare settings. High-volume centers with experienced endoscopists are more likely to offer EUS-GBD, while smaller or less specialized centers may rely on PT-GBD due to its relative ease and the ubiquity of procedural expertise. (2) A multicenter study in Japan demonstrated that even in centers newly introducing EUS-guided biliary drainage, the technical success rate was 91.4%, but the procedure's complexity and the need for specialized equipment can hinder its broader implementation. (15)
B. Cost and Access to Technology
High costs and limited access to advanced equipment pose significant barriers to EUS-GBD adoption. LAMS, although shown to be cost-effective compared with prolonged hospital stays in PT-GBD, (16) remains expensive, and specialized EUS equipment adds to the financial burden—particularly in low-resource settings where PT-GBD is more readily performed due to lower upfront costs. (2) Variability in resource availability and the need for specialized training further constrain EUS-GBD implementation, as only high-volume centers typically possess the requisite expertise. (2) Standardized training programs, reduced equipment costs, and broader access to advanced endoscopic technologies are crucial to overcoming these challenges and improving patient care.
C. Long-Term Outcomes and Stent-Related Complications
Further studies are needed to clarify the long-term efficacy and safety of EUS-GBD versus PT-GBD, focusing on stent migration, occlusion, and the need for additional interventions. Although EUS-GBD with LAMS generally achieves favorable outcomes, adverse events such as stent migration, occlusion, and recurrent cholecystitis can still occur in 4.8% to 22% of cases. (2) One multicenter study reported significantly lower 1-year adverse events (25.6% vs. 77.5%, p < 0.001) and 30-day adverse events (12.8% vs. 47.5%, p = 0.010) for EUS-GBD compared to PT-GBD. (17) However, data on stent patency and re-interventions over the long term remain limited. PT-GBD, while effective, is associated with higher morbidity and recurrent cholecystitis rates. (2)
Future Directions and Innovations
A. Next-Generation Stents and Techniques
The development of next-generation stents, including bioabsorbable stents, represents a significant advancement in EUS-GBD. Bioabsorbable stents are designed to degrade over time, reducing the need for stent removal and minimizing long-term complications. These stents are fabricated from materials such as biodegradable polymers and metals, which have shown promising results in preclinical and early clinical studies. The AGA highlights the potential of these stents to improve patient outcomes by reducing the risk of stent-related complications. (18)
Another innovative direction is the development of smart stents equipped with integrated sensors. These stents can detect early signs of complications such as stent occlusion or migration. Smart stents utilize advanced materials and nanotechnology to provide real-time data, which can be transmitted wirelessly to healthcare providers for timely intervention. This technology promises to enhance patient safety and improve the long-term efficacy of EUS-GBD. (19)
EC-LAMS have improved procedural efficiency by allowing a one-step deployment process. This innovation reduces procedural time and the need for multiple device exchanges, thereby enhancing the safety and success rates of EUS-GBD. The AGA supports the use of EC-LAMS for their ability to simplify the procedure and improve patient outcomes. (20)
B. Expanding Indications for EUS-Guided Drainage
endoscopic ultrasound-guided biliary drainage EUS- BD has expanded its indications beyond gallbladder drainage to include various biliary and pancreatic diseases. This expansion is supported by advancements in stent technology and procedural techniques.
EUS-BD is increasingly used as an alternative to PT-GBD and ERCP in cases of failed ERCP, particularly in patients with surgically altered anatomy or malignant biliary obstruction. EUS-BD techniques include choledochoduodenostomy and hepaticogastrostomy, which have shown high technical and clinical success rates. (21)
EUS-guided pancreatic duct drainage (EUS-PD) is utilized for patients with obstructive pancreatitis or pancreatic duct strictures when ERCP is not feasible. This approach offers a minimally invasive alternative with promising outcomes. (22)
EUS-guided drainage of pancreatic fluid collections, including pseudocysts and walled-off necrosis, has become a standard of care. The use of LAMS has improved the safety and efficacy of these procedures. (21)
Robotic-assisted endoscopy is an emerging field that aims to enhance precision and control during EUS-guided interventions. Robotic platforms can provide better stability, dexterity, and visualization, potentially improving the accuracy and safety of procedures such as EUS-GBD, EUS-BD, and EUS-PD. This integration is still in its early stages but holds promise for future advancements in therapeutic endoscopy. (21)
C. Optimizing Patient-Centered Care
Optimizing patient-centered care in the context of EUS-GBD and PT-GBD involves developing guidelines for selecting the most appropriate drainage approach and enhancing interdisciplinary collaboration for better clinical outcomes.
Evaluate the patient's overall health, comorbidities, and surgical risk. High-risk patients, such as those with severe organ failure or advanced malignancy, are prime candidates for non-surgical drainage. Use imaging studies to assess the anatomical relationship between the gastrointestinal tract and the gallbladder, ensuring that the distance is less than 10 mm for safe EUS-GBD stent deployment. (2)
EUS-GBD is preferred for its higher technical and clinical success rates, lower post-procedural pain, fewer re-interventions, and shorter hospital stays compared to PT-GBD. (2)
PT-GBD remains a viable option in settings where EUS expertise is not available or in patients with contraindications to EUS-GBD, such as large-volume ascites or coagulopathy. (2)
Enhance interdisciplinary collaboration involving gastroenterologists, interventional radiologists, and surgeons in the decision-making process. This ensures comprehensive patient evaluation and optimal treatment planning. Conduct regular multidisciplinary team meetings to discuss complex cases and determine the best approach based on available expertise and patient-specific factors. Develop standardized protocols for patient selection, procedural techniques, and post-procedure follow-up to ensure consistent, high-quality care across different healthcare settings. The AGA emphasizes the importance of gathering more data to establish these standards and ensure consistent, high-quality care. (2)
Conclusion
Gallbladder disease management has evolved from open cholecystectomy to laparoscopic techniques and, more recently, to EUS-GBD. Though PT-GBD remains valuable, especially in centers lacking EUS expertise, its external tubes and higher complication rates pose disadvantages. EUS-GBD with lumen-apposing metal stents has demonstrated high technical and clinical success rates, fewer adverse events, and shorter hospital stays, establishing it as a safer and more effective alternative for high-risk patients. (2,9,8)
Further investigations are needed to gather long-term data on stent patency, migration, and reinterventions. Innovations in stent technology, such as bioabsorbable or sensor-equipped stents, along with standardized patient selection protocols, will likely shape the future of gallbladder drainage. Close collaboration among multidisciplinary teams ensures that evolving techniques are both feasible and safe, ultimately enhancing patient-centered care.
Declarations of Interest: None
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Reference
1. Podboy, A., Yuan, J., Stave, C. D., Chan, S. M., Hwang, J. H., & Teoh, A. Y. B. (2021). Comparison of EUS-guided endoscopic transpapillary and percutaneous gallbladder drainage for acute cholecystitis: a systematic review with network meta-analysis. Gastrointestinal endoscopy, 93(4), 797–804.e1. https://doi.org/10.1016/j.gie.2020.09.040
2. Irani, S. S., Sharzehi, K., & Siddiqui, U. D. (2023). AGA Clinical Practice Update on Role of EUS-Guided Gallbladder Drainage in Acute Cholecystitis: Commentary. Clinical gastroenterology and hepatology, 21(5), 1141–1147. https://doi.org/10.1016/j.cgh.2022.12.039
3. Wolf, A. S., Nijsse, B. A., Sokal, S. M., Chang, Y., & Berger, D. L. (2009). Surgical outcomes of open cholecystectomy in the laparoscopic era. American journal of surgery, 197(6), 781–784. https://doi.org/10.1016/j.amjsurg.2008.05.010
4. Rosen, M., & Ponsky, J. (2001). Minimally invasive surgery. Endoscopy, 33(4), 358–366. https://doi.org/10.1055/s-2001-13689
5. Brandon, J. C., Velez, M. A., Teplick, S. K., Mueller, P. R., Rattner, D. W., Broadwater, J. R., Jr, Lang, N. P., & Eidt, J. F. (1991). Laparoscopic cholecystectomy: evolution, early results, and impact on nonsurgical gallstone therapies. AJR. American journal of roentgenology, 157(2), 235–239. https://doi.org/10.2214/ajr.157.2.1830188
6. Baron, T. H., Grimm, I. S., & Swanstrom, L. L. (2015). Interventional Approaches to Gallbladder Disease. The New England journal of medicine, 373(4), 357–365. https://doi.org/10.1056/NEJMra1411372
7. McCarty, T. R., Hathorn, K. E., Bazarbashi, A. N., Jajoo, K., Ryou, M., & Thompson, C. C. (2021). Endoscopic gallbladder drainage for symptomatic gallbladder disease: a cumulative systematic review meta-analysis. Surgical endoscopy, 35(9), 4964–4985. https://doi.org/10.1007/s00464-020-07758-3
8. Teh, J. L., Rimbas, M., Larghi, A., & Teoh, A. Y. B. (2022). Endoscopic ultrasound in the management of acute cholecystitis. Best practice & research. Clinical gastroenterology, 60-61, 101806. https://doi.org/10.1016/j.bpg.2022.101806
9. Irani, S., Ngamruengphong, S., Teoh, A., Will, U., Nieto, J., Abu Dayyeh, B. K., Gan, S. I., Larsen, M., Yip, H. C., Topazian, M. D., Levy, M. J., Thompson, C. C., Storm, A. C., Hajiyeva, G., Ismail, A., Chen, Y. I., Bukhari, M., Chavez, Y. H., Kumbhari, V., & Khashab, M. A. (2017). Similar Efficacies of Endoscopic Ultrasound Gallbladder Drainage With a Lumen-Apposing Metal Stent Versus Percutaneous Transhepatic Gallbladder Drainage for Acute Cholecystitis. Clinical gastroenterology and hepatology, 15(5), 738–745. https://doi.org/10.1016/j.cgh.2016.12.021
10. Siddiqui, A., Kunda, R., Tyberg, A., Arain, M. A., Noor, A., Mumtaz, T., Iqbal, U., Loren, D. E., Kowalski, T. E., Adler, D. G., Saumoy, M., Gaidhane, M., Mallery, S., Christiansen, E. M., Nieto, J., & Kahaleh, M. (2019). Three-way comparative study of endoscopic ultrasound-guided transmural gallbladder drainage using lumen-apposing metal stents versus endoscopic transpapillary drainage versus percutaneous cholecystostomy for gallbladder drainage in high-risk surgical patients with acute cholecystitis: clinical outcomes and success in an International, Multicenter Study. Surgical endoscopy, 33(4), 1260–1270. https://doi.org/10.1007/s00464-018-6406-7
11. Hayat, U., Al Shabeeb, R., Perez, P., Hensien, J., Dwivedi, A., Sakhawat, U., Ahmad, O., Haseeb, M., Siddiqui, A. A., & Adler, D. G. (2024). Safety and adverse events of EUS-guided gallbladder drainage using lumen-apposing metal stents and percutaneous cholecystostomy tubes: a systematic review and meta-analysis. Gastrointestinal endoscopy, 99(3), 444–448.e1. https://doi.org/10.1016/j.gie.2023.10.043
12. Chon, H. K., Lee, Y. C., Kim, T. H., Lee, S. O., & Kim, S. H. (2024). Revolutionizing outcomes: endoscopic ultrasound-guided gallbladder drainage using innovative electrocautery enhanced-lumen apposing metal stents for high-risk surgical patients. Scientific reports, 14(1), 12893. https://doi.org/10.1038/s41598-024-63608-5
13. Hemerly, M. C., de Moura, D. T. H., do Monte Junior, E. S., Proença, I. M., Ribeiro, I. B., Yvamoto, E. Y., Ribas, P. H. B. V., Sánchez-Luna, S. A., Bernardo, W. M., & de Moura, E. G. H. (2023). Endoscopic ultrasound (EUS)-guided cholecystostomy versus percutaneous cholecystostomy (PTC) in the management of acute cholecystitis in patients unfit for surgery: a systematic review and meta-analysis. Surgical endoscopy, 37(4), 2421–2438. https://doi.org/10.1007/s00464-022-09712-x
14. Luk, S. W., Irani, S., Krishnamoorthi, R., Wong Lau, J. Y., Wai Ng, E. K., & Teoh, A. Y. (2019). Endoscopic ultrasound-guided gallbladder drainage versus percutaneous cholecystostomy for high risk surgical patients with acute cholecystitis: a systematic review and meta-analysis. Endoscopy, 51(8), 722–732. https://doi.org/10.1055/a-0929-6603
15. Koga, T., Ishida, Y., Hashigo, S., Shimokawa, Y., Harima, H., Okamoto, K., Ohno, A., Miyagahara, T., Fujita, T., Fukuchi, S., Takahashi, K., Taguchi, H., Araki, N., Ohtsuka, Y., Uekitani, T., Tsuneyoshi, K., Akiyama, T., Ishigaki, N., Maruo, T., Saito, H., … Hirai, F. (2024). Feasibility and safety of EUS-guided biliary drainage in inexperienced centers: a multicenter study in southwest Japan. Gastrointestinal endoscopy, S0016-5107(24)03495-3. Advance online publication. https://doi.org/10.1016/j.gie.2024.09.014
16. Corral, J. E., Das, A., Kr?ner, P. T., Gomez, V., & Wallace, M. B. (2019). Cost effectiveness of endoscopic gallbladder drainage to treat acute cholecystitis in poor surgical candidates. Surgical endoscopy, 33(11), 3567–3577. https://doi.org/10.1007/s00464-019-07026-z
17. Teoh, A. Y. B., Kitano, M., Itoi, T., Pérez-Miranda, M., Ogura, T., Chan, S. M., Serna-Higuera, C., Omoto, S., Torres-Yuste, R., Tsuichiya, T., Wong, K. T., Leung, C. H., Chiu, P. W. Y., Ng, E. K. W., & Lau, J. Y. W. (2020). Endosonography-guided gallbladder drainage versus percutaneous cholecystostomy in very high-risk surgical patients with acute cholecystitis: an international randomised multicentre controlled superiority trial (DRAC 1). Gut, 69(6), 1085–1091. https://doi.org/10.1136/gutjnl-2019-319996
18. Choudhury, S., Asthana, S., Homer-Vanniasinkam, S., & Chatterjee, K. (2022). Emerging trends in biliary stents: a materials and manufacturing perspective. Biomaterials science, 10(14), 3716–3729. https://doi.org/10.1039/d2bm00234e
19. Hoare, D., Bussooa, A., Neale, S., Mirzai, N., & Mercer, J. (2019). The Future of Cardiovascular Stents: Bioresorbable and Integrated Biosensor Technology. Advanced science (Weinheim, Baden-Wurttemberg, Germany), 6(20), 1900856. https://doi.org/10.1002/advs.201900856
20. Huh, G., Choi, J. H., Lee, S. H., Paik, W. H., Ryu, J. K., Kim, Y. T., Jeong, S., Lee, D. H., Kim, G. H., & Kang, S. G. (2020). Innovation of EUS-guided transmural gallbladder drainage using a novel self-expanding metal stent. Scientific reports, 10(1), 11159. https://doi.org/10.1038/s41598-020-67374-y
21. Khan, R., & Law, R. (2024). Therapeutic Endoscopic Ultrasound and Endoscopic Ultrasound-Endoscopic Retrograde Cholangiopancreatography Interventions. Gastroenterology clinics of North America, 53(4), 683–707. https://doi.org/10.1016/j.gtc.2024.08.016
22. Wahba, G., & Lee, J. H. (2025). Updates on therapeutic endoscopic ultrasound. Current opinion in gastroenterology, 41(1), 16–28. https://doi.org/10.1097/MOG.0000000000001072.