Management of Fresh Traumatic Macular Holes with High Dose Steroids (Tandon’s Regime) - A Comparative Study
Management of Fresh Traumatic Macular Holes with High Dose Steroids (Tandon’s Regime) - A Comparative Study
Prof. Manish Tandon *1, Prof David Maberley 2, Dr Jeevan A Kale 3
1. Prof. Manish Tandon, DNB, Prayag Retina Care, Prayagraj, India.
2. Prof David Maberley, MD, University of Ottawa, Canada.
3. Dr Jeevan A Kale, MS, Aravind Eye Hospital and post graduate institute of ophthalmology, Madurai, India.
*Correspondence to: Prof Manish Tandon, 8/9/4 Panna Lal Road, Prayagraj, India
Copyright
© 2025 Prof. Manish Tandon. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 March 2025
Published: 01 April 2025
Abstract:
Purpose: To evaluate the safety and efficacy of intravenous methylprednisolone (IVMP) in treating traumatic macular holes (TMH).
Design: Prospective Study.
Methods: In this study 11 patients with TMH who presented within 72 hours of injury were offered either IVMP (500mg/day for 4 days) or observation (controls). Rates of macular hole closure was the primary outcome while improvement in visual acuity on day 1 and at 1 and 3 months was a secondary outcome.
Results: Eleven eyes of 11 patients with a mean age of 17.3 + 6.4 years were included in the study of which 6 received IVMP. The holes were larger (1933 + 1093μ vs 1505 + 580, p=0.58) and vision slightly lower (1.27 + 0.5 vs. 1.16 + 0.3, p=0.69) in the IVMP group. All 6 eyes (100%) in the IVMP group experienced hole closure at a median of 2 days after IVMP initiation while none in the control group experienced spontaneous closure at 3 months. The visual acuity improved to 0.67 + 0.3 in the IVMP group at 3months (p=0.02) but remained almost unchanged in controls.
Conclusions: Pulse IVMP is well tolerated and may be a viable treatment option for TMH when administered within the first few days of trauma
Management of Fresh Traumatic Macular Holes with High Dose Steroids (Tandon’s Regime) - A Comparative Study
Introduction
Traumatic macular holes (TMH) are uncommon occurrences after ocular trauma and occur more frequently after blunt trauma but can rarely occur after open globe injuries as well. Spontaneous closure of TMH have been reported in 20 to 66% of eyes in the past,(1–4) and this occurs within the first two to three months of trauma,(2) prompting most retina specialists to wait and watch for spontaneous closure as the first measure and resort to vitrectomy with internal limiting peeling in case of non – closure.(5) Yet, the timing of surgery for TMH has been debated over the years with proponents for both, early and delayed surgery, especially since vitrectomy success rates may be as low as 60% in some cases.(6,7)
Optical coherence tomography features for non–closure of TMH have been reported in the past and include larger holes >250 microns in basal diameter and the presence of cystoid edema (CME) at one or both edges of the hole.(8–10) Early vitrectomy may be considered in these eyes, especially if there are no signs of spontaneous closure after 6-8 weeks of observation but visual outcomes are guarded in such cases. The presence of CME at the edges of the TMH suggests localized inflammation because of traumatic disruption of the blood-retinal barrier. This excess fluid at the edges of the hole may contribute to non–closure by contributing to the centrifugal traumatic forces and retracting the inner retinal surface. Indeed, two case reports using topical ketorolac in this scenario have reported hole closure due to resolution of the inflammatory edema, thus giving credence to this theory of severe inflammation leading to persistent non – closure of TMH.(11,12) In this comparative study, we report on the TMH closure rates and visual outcomes of eyes treated with intravenous methyl prednisolone initiated in the first few days of trauma.
Methods
This was a prospective observational comparative study of patients with TMH who presented to our institution over 3 years. The study was approved by the institutional ethics committee and was conducted as per the tenets of the declaration of Helsinki. Informed consent was obtained from all patients or their legal guardians in case they were below 18 years of age.
The study included all consecutive consenting patients who presented to our institution with TMH due to closed globe injury during the study period and were willing for a follow up of at least 3 months. Patients were excluded if the TMH was due to open globe injury, or duration of trauma and vision loss was > 3 days, and those with coexistent trauma to other ocular structures such as hyphema, zonular or retinal dialysis, raised intraocular pressure, traumatic cataract, angle recession and such other trauma related pathologies were also excluded. Similarly, patients with a history of previous ocular trauma, systemic co-morbidities like diabetes and any previous signs of ocular inflammation were excluded from this study. Lastly, patients with other severe trauma such as head injury leading to coma, and injuries to other organs as part of road traffic accidents were also excluded.
Patients were offered initial treatment with either intravenous methyl prednisolone (IVMP) or observation for a period of 3 months. Prior to treatment, the ocular and systemic risks and benefits of IVMP and its experimental nature were clearly explained in detail to the patients and their guardians by one of the authors. Only patients who voluntarily (or consenting parents/guardians in case of minors) agreed to the IVMP were included in the treatment arm while those who chose observation served as controls. For patients in the treatment arm, medical clearance was obtained from the in-house internist. The IVMP was administered at dose of 500mg per day (for age <18 years) or 1000mg per day (for age >18 years) via slow intravenous infusion over 1-1.5hours for four consecutive days without a tapering maintenance dose. Fasting and random blood sugars and a review by the internist were performed prior to each dose of IVMP. All patients also received topical prednisolone eye drops in a tapering fashion in view of some degree of traumatic uveitis.
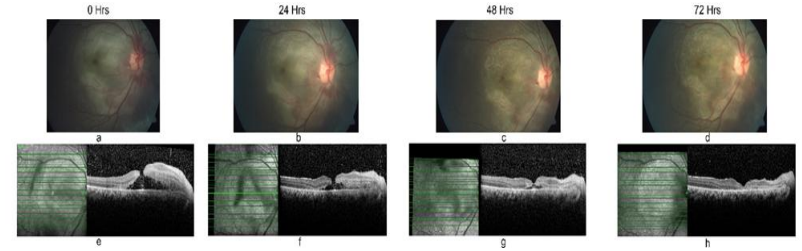
All participants underwent a comprehensive ophthalmic evaluation at baseline including best corrected visual acuity (BCVA) using the Snellen’s chart (converted to logarithm of minimal angle of resolution (logMAR) for analysis), slit lamp clinical examination, gonioscopy to rule out angle recession, intraocular pressure (IOP) using the applanation tonometry, colour fundus photography (Topcon, USA) and optical coherence tomography (OCT) (Heidelberg, Germany, Version 1.9.20.0). The BCVA and serial OCT scans (figure 1) were performed for all patients daily for the first 4 days and then at 1 month and 3 months follow up. All scans were done at all time points by an OCT technician masked to the treatment status of patients. Similarly, a fellowship trained retina specialist (XX) who evaluated images at the time of analysis was masked to the treatment status. Serial images obtained daily from eyes in both groups were presented to him in a jumbled fashion such that no two images from consecutive days from the same eye were presented one after the other. He commented on the maximal apical and basal diameter of the TMH at baseline at each time point as well as presence of CME at the hole edges and closure of macular hole defined as approximation of the internal and external limiting membranes across the full thickness macular defect along with approximation of the other neurosensory retinal layers. The apical diameter was the closest distance between the two elevated edges of the TMH and the basal was the largest distance at the base on the two sides of elevated edges.
Figure 1 Legend: Sequential fundus photo and OCT of one patient treated showing closure of macular hole in 72 hours.
Statistical analysis
All continuous variables were presented as mean with standard deviation or median with interquartile range and group differences between IVMP group and controls were assessed using the student t test or the Wilcoxon’s ranksum test for non – parametric distributions. Categorical variables were presented as proportions (n, %) and group differences were assessed using the chi square or the Fischer’s exact test. The paired t test was used to compare BCVA before and after treatment at various time points.
All data were stored using Microsoft Excel and analysed using Stata 12.1 I/c (Stata Corp, Fort Worth, Texas, USA) and p values of <0.05 were considered statistically significant.
Results
The study included 11 eyes with TMH of which 6 eyes received IVMP and 5 served as controls. The mean age of participants was 17.3 + 6.4 years and 10 out of 11 (91%) were men. The right eye was slightly more commonly involved (n=7, 64%) compared to the left (n=4, 36%). Injury with a cricket or tennis ball was the commonest mode of trauma (n=3, 27%) while injury with a stone (n=2, 17%) and cricket bat (n=2, 17%) were the common modes. The median duration between trauma and presentation was 2 days (IQR=1 day). The mean basal diameter of the TMH was 1718 + 732 microns and the presenting BCVA in the study cohort was 1.21 + 0.4 logMAR (20/320 Snellen’s equivalent).
A comparison between eyes that received IVMP (n=6) vs. those that did not (n=5 controls) is shown in table 1. Patients in the IVMP group were significantly younger compared to the controls. This group also had larger basal diameters of the TMH and lower BCVA compared to controls, though differences between groups were not statistically significant. All 11 eyes (100%) had CME at the edges of the TMH at presentation. All eyes in the IVMP group experienced closure of the TMH (figure 1) while none of the controls had spontaneous closure. The closure occurred on day 1 in 2 eyes (33%), on day 2 in 3 eyes (50%) and on day 3 in the remaining eye (17%), though all participants in the IVMP group completed the 4 day course of therapy as planned. The visual acuity improved significantly in the IVMP group on day 1 itself (table 1) and continued to improve at the 1 and 3 month time period, while this was marginal and not significant in the controls. There was foveal thinning in all eyes at 3 months following IVMP therapy with the mean central foveal thickness of 193 + 32 microns accounting for reduced visual acuity at 3 months.
One patient experienced sudden hyperglycemia after three doses of IVMP with blood sugar rising to >400mg and was transiently managed with insulin. The fourth dose of IVMP was given on day 5 under the internist’s observation. None of the other patients experienced any adverse events of therapy.
Table 1: Comparison of baseline and follow up characteristics in eyes receiving IVMP vs. controls
|
Variable |
IVMP (n=6) |
Controls (n=5) |
P value |
|
Age (years) |
22.4 + 5.3 |
13 + 3.5 |
0.006 |
|
Age range (years) |
17 - 29 |
11 – 20 |
-- |
|
Gender (% boys) |
6 (100%) |
4 (80%) |
0.87 |
|
Baseline TMH basal diameter |
1933 + 1093 |
1505 + 580 |
0.58 |
|
Baseline TMH apical diameter |
454 + 418) |
674 + 306 |
0.27 |
|
Visual acuity |
|||
|
Baseline |
1.27 + 0.5 |
1.16 + 0.3 |
0.69 |
|
Day 1 |
1.06 + 0.4 |
1.16 + 0.3 |
0.46 |
|
Month 1 |
0.74 + 0.3 |
1.04 + 0.4 |
0.27 |
|
Month 3 |
0.67 + 0.3 |
1.04 + 0.4 |
0.17 |
|
CFT at last follow up |
|
|
|
|
P-value** D0 Vs D1 D0 Vs M1 D0 Vs M3 |
0.04 0.03 0.02 |
0.33 0.16 0.16 |
|
|
Macular hole closure |
6 (100%) |
0 |
--- |
** paired t test.
Discussion
In this series of eyes with fresh but very large TMH in relatively young men, all eyes in the IVMP group experienced closure of the macular hole within two to three days of initiating IVMP therapy, while none in the observation group had spontaneous closure within the first three months of injury. Hole closure was seen on day 1 of IVMP itself and vision continued to improve at 1 and 3 months follow up, with an almost five line gain from 20/320 at baseline to 20/100 Snellen’s equivalent, though this gain was limited by some degree of foveal thinning at three months. The IVMP was tolerated well by majority of patients with only one patient experiencing sudden hyperglycemia that was managed medically with insulin.
The role played by inflammation and inflammatory cytokines at the cellular level in eyes with TMH has not been studied well. In an experimental study, Gregor and Ryan induced blunt trauma to pig eyes using led pellet shots from an air pistol and performed fundus photography, fluorescein angioscopy and histopathology at 24 hours and on days 3 and 7 following trauma.(13) They showed disruption of the retinal pigment epithelium (RPE) and the outer blood retinal barrier with collection of extracellular fluid in the outer retina up to 3 days followed by disappearance of fluid by day 7. The authors attributed this fluid collection to traumatic disruption of the RPE cells followed by recovery after 3 days. Sudden excess fluid collection in the outer retina may lead to TMH due to a break through mechanism at the point of least resistance i.e. the centre of the fovea where the retina is at its thinnest. It is possible that pulse IVMP may hasten the recovery of the RPE cells leading to early fluid resorption and hole closure within 3 days of trauma. If this were true, IVMP may not be effective after the first 7 days of TMH formation, though this needs to be studied further.
Biomarkers on OCT that predict non – closure of TMH include large sized holes and those with excess fluid at one or both edges of the hole.(9,14) Most TMH are larger than idiopathic macular holes(15) likely due to severe perifoveal inflammation and fluid collection that itself exerts an outward force and retracts the inner retinal surface thereby preventing the approximation of the separated edges of the neurosensory retina. With IVMP, this inflammation may resolve rapidly, with disappearance of the fluid thereby leading to relief of the outward force. This may help in approximation of the edges of the separated macula which fall back into anatomical position with resultant hole closure. Additionally, the tangential tractional forces in TMH are transient lasting only during the trauma and hence may not impede hole closure after the first 24 hours of trauma, unlike in idiopathic holes where the antero-posterior traction along with tangential traction due to ILM changes lead to persistent tractional forces and closure of holes only once this traction is relieved surgically with PVD induction and ILM peeling.
In a recent case report, Li and Ferrone demonstrate closure of a TMH in a 15 year old healthy girl with topical ketorolac eye drops initiated nearly two months after TMH onset without spontaneous closure.(12) The ketorolac was applied 4 times a day for 1 month, and then tapered gradually. Though the patient had a TMH with a basal diameter of 400 microns, much smaller than our series, and BCVA of 20/40, much better than our typical patient, traumatic hole closure within four weeks of topical NSAID with disappearance of CME, suggests that ketorolac’s anti-inflammatory properties exerted a therapeutic effect leading to hole closure. In another case reported more than a decade ago, Kurz et al reported the case of a 63 year old man with a TMH and BCVA of 20/80 at presentation.(11) The hole closed with topical ketorolac, and then reopened after stopping the drug, to close again after 11 weeks of using topical nepafenac, another topical NSAID. In both these cases, the TMH were observed initially and anti – inflammatory drops initiated later lead to hole closure. We were unable to find any other reports of this nature. To the best of our knowledge, there are no reports exploring the influence of IVMP on closure rates of TMH.
Given our findings and previous reports, it appears that early hole closure may be enhanced by the healing effects of pulse IVMP on the disrupted RPE cells and closure of delayed TMH. On the other hand, topical anti – inflammatory therapy may be able to resolve the CME at the edges of the TMH and might be effective in closure of smaller TMH that haven’t closed due to persistent CME at its edges. We observed retinal thinning involving the centre of the fovea at the 3 months’ time point in all eyes in the IVMP group limiting further visual gain. However, this is expected even after vitrectomy surgery and may be a result of RPE damage due to the trauma. We included only fresh cases of TMH with presentation within 72 hours of trauma i.e. when there would be intense RPE injury, and administered the strongest anti – inflammatory agent available i.e. high dose corticosteroids in the form of pulse IVMP to hasten recovery. A similar strategy has been used in other cases of trauma, most notably for traumatic brain(16) and spinal cord injury with mixed results.(17) Lastly, IVMP is well tolerated by the young patient population who experience TMH due to general good health without comorbidities.
Caution must be observed while interpreting conclusions from this case series with limited numbers without randomization and larger studies with better study design and longer follow up are needed to validate these results. However, our study provides initial evidence of the effectiveness of high dose pulse steroids for TMH that can be used for eyes with fresh and large holes.
In conclusion, IVMP may be a viable treatment option for TMH when administered within the first few days of trauma, especially when observation and waiting for spontaneous closure is the current norm at this time point. It is tolerated reasonably well by young men and may be a used as option for holes with characteristics that predict spontaneous non – closure.
References
1. Chen H-J, Jin Y, Shen L-J, Wang Y, Li Z-Y, Fang X-Y, et al. Traumatic macular hole study: a multicenter comparative study between immediate vitrectomy and six-month observation for spontaneous closure. Ann Transl Med. 2019 Dec;7(23):726.
2. Miller JB, Yonekawa Y, Eliott D, Kim IK, Kim LA, Loewenstein JI, et al. Long-term Follow-up and Outcomes in Traumatic Macular Holes. Am J Ophthalmol. 2015 Dec;160(6):1255-1258.e1.
3. Gao M, Liu K, Lin Q, Liu H. Management Modalities for Traumatic Macular Hole: A Systematic Review and Single-Arm Meta-Analysis. Curr Eye Res. 2017 Feb;42(2):287–96.
4. Yamashita T, Uemara A, Uchino E, Doi N, Ohba N. Spontaneous closure of traumatic macular hole. Am J Ophthalmol. 2002 Feb;133(2):230–5.
5. Sheth JU, Weng C, Singh R, Khatri M, Saurabh K, Chawla S, et al. Vitreoretinal Society of India practice pattern survey 2020: Surgical retina. Indian J Ophthalmol. 2021 Jun;69(6):1442–9.
6. Ghoraba HH, Leila M, Zaky AG, Wasfy T, Maamoun Abdelfattah H, Elgemai EM, et al. Results of Pars Plana Vitrectomy for Different Types of Macular Holes. Clin Ophthalmol. 2021;15:551–7.
7. Thanos A, Todorich B. Traumatic macular holes: to operate, or not to operate, that is the question. Ann Transl Med. 2020 Aug;8(15):916.
8. Miller JB, Yonekawa Y, Eliott D, Vavvas DG. A review of traumatic macular hole: diagnosis and treatment. Int Ophthalmol Clin. 2013;53(4):59–67.
9. Huang J, Liu X, Wu Z, Lin X, Li M, Dustin L, et al. Classification of full-thickness traumatic macular holes by optical coherence tomography. Retina. 2009 Mar;29(3):340–8.
10. Lei C, Chen L. Traumatic Macular Hole: Clinical Management and Optical Coherence Tomography Features. J Ophthalmol. 2020;2020:4819468.
11. Kurz PA, Kurz DE. Macular hole closure and visual improvement with topical nonsteroidal treatment. Arch Ophthalmol. 2009 Dec;127(12):1687–8.
12. Li AS, Ferrone PJ. TRAUMATIC MACULAR HOLE CLOSURE AND VISUAL IMPROVEMENT AFTER TOPICAL NONSTEROIDAL ANTIINFLAMMATORY DRUG TREATMENT. Retin Cases Brief Rep. 2020;14(4):324–7.
13. Gregor Z, Ryan SJ. Blood-retinal barrier after blunt trauma to the eye. Graefes Arch Clin Exp Ophthalmol. 1982;219(5):205–8.
14. Johnson RN, McDonald HR, Lewis H, Grand MG, Murray TG, Mieler WF, et al. Traumatic macular hole: observations, pathogenesis, and results of vitrectomy surgery. Ophthalmology. 2001 May;108(5):853–7.
15. Huang J, Liu X, Wu Z, Sadda S. Comparison of full-thickness traumatic macular holes and idiopathic macular holes by optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2010 Aug;248(8):1071–5.
16. Alderson P, Roberts I. Corticosteroids for acute traumatic brain injury. Cochrane Database Syst Rev. 2005 Jan 24;2005(1):CD000196.
17. Bracken MB. Steroids for acute spinal cord injury. Cochrane Database Syst Rev. 2012 Jan 18;1:CD001046.