Analysis of Risk Factors, Clinical Features and Microbiology Findings in Neonates with Central Nervous System Infections caused by Gram-positive Bacteria
Analysis of Risk Factors, Clinical Features and Microbiology Findings in Neonates with Central Nervous System Infections caused by Gram-positive Bacteria
Ilija Palic*
*Correspondence to: Ilija Palic, Intensive Care Unit, Institute of Neonatology, 50 Kralj Milutin, 11000 Belgrade, Serbia.
Copyright
© 2025: Ilija Palic. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 Mar 2025
Published: 01 Apr 2025
Abstract
Background: Meningitis and its complications are important causes of mortality and morbidity in neonates. Preterm neonates and low birth weight neonates are more susceptible to bacterial meningitis than full-term neonates and older children. Gram-positive bacteria, especially coagulase-negative Staphylococci have been identified as a common cause of late-onset neonatal sepsis and meningitis. The most common complication of meningitis is ventriculitis.
Objective: The purpose of this study was to evaluate perinatal and clinical characteristics, risk factors, as well as bacteriological findings in cerebrospinal fluid in neonates with meningitis and/or ventriculitis caused by Gram-positive bacteria.
Patients and Methods: A retrospective study included neonates diagnosed with Gram-positive bacterial meningitis and/or ventriculitis from 2009 to 2024. Diagnosis of meningitis and/or ventriculitis was based on clinical picture and analyses of cerebrospinal fluid. The data for analysis were obtained from the medical history.
Results: Analysis included 12 preterm neonates. More than half, 8 (66.7%), were born before 28 weeks of gestation. There were 10 (83.3%) female neonates. Eight (66.7%) neonates were born by cesarean section. The mean gestational age was 27.3 and the mean birth weight was 1019.2 g. Apgar score ranged from 2 to 8 in the first minute of life. Ten (83.3%) neonates requiring endotracheal intubation at birth. Seven (58.3%) neonates had late-onset sepsis complicated with meningitis and 5 (41.7%) had shunt-related ventriculitis. Gram-positive bacteria from genus Staphylococcus was the most common cause of neonatal central nervous system infections. Coagulase-negative Staphylococci was detected in cerebrospinal fluid in three neonates and Staphylococcus haemolyticus in two neonates. Staphylococcus epidermidis was the most common cause of ventriculitis in neonates requiring cerebrospinal fluid drainage with Ommaya subcutaneous reservoir. One extremely preterm neonate was diagnosed with late-onset meningitis caused by group B Streptococcus. Other Gram-positive bacteria detected in cerebrospinal fluid were Enterococci. Death was recorded in one neonate.
Conclusion: Prematurity and prolonged hospitalization in neonatal intensive care unit are the main risk factors for late-onset neonatal sepsis and meningitis caused by Gram-positive bacteria. Neonates with posthemorrhagic ventricular dilatation are at strong risk for ventriculitis.
Keywords: prematurity, newborn, meningitis, ventriculitis, Gram-positive bacteria.
Analysis of Risk Factors, Clinical Features and Microbiology Findings in Neonates with Central Nervous System Infections caused by Gram-positive Bacteria
Introduction
Various types of bacteria can cause infections of the central nervous system (CNS) and meninges with devastating effects on its structure and function. Central nervous system infections can occur during intrauterine development, during delivery, or in the first days and weeks after birth. Regardless of the causative microorganism and time of onset, CNS infections can lead to neonatal death and, among survivors, to permanent neurological sequelae, such as epilepsy, vision and hearing impairment, cognitive deficits, motor disabilities and behavioral problems (1-3). Due to the immature of various components of the cellular and humoral immune system and the poor function of the blood-brain barrier, the neonates, especially those born prematurely, are at increased risk of developing CNS infections (3-6). Meningitis, defined as direct invasion and inflammation of the meninges, is the most common bacterial CNS infection in neonates (3,7). In most neonates, bacterial meningitis is associated with recognizable bacteremia and sepsis. However, studies have shown that about 30% of neonates had meningitis with negative blood cultures (3,8,9). The main risk factors for neonatal meningitis are prematurity, low birth weight (BW) (< 2500 g), prolonged hospitalization in the neonatal intensive care unit (NICU), chorioamnionitis and prolonged rupture of the chorioamniotic membrane (PROM) (> 18 hours), traumatic delivery, fetal hypoxia and maternal group B Streptococcus (GBS) colonization (10-12). Gram-negative bacteria are more commonly cause of meningitis in preterm than in full-term neonates. In early-onset meningitis, group B Streptococcus is the most common cause in full-term neonates, but meningitis caused by Escherichia coli primarily occurs in preterm neonates. Over the past two decades, with the increasing survival of preterm neonates, especially extremely preterm neonates, coagulase-negative Staphylococci (CoNS) have been identified as a common cause of late-onset neonatal sepsis and meningitis. The most common complication of meningitis is ventriculitis (3,6,13-15). The objective of this study was to analyse perinatal and clinical characteristics, risk factors, as well as bacteriological findings in cerebrospinal fluid (CSF) and neurosonography findings in neonates with Gram-positive bacterial meningitis and ventriculitis.
Patients and Methods
In this retrospective study were included 12 neonates with meningitis and/or ventriculitis caused by Gram-positive bacteria (GPB) who were treated in our hospital between 2009 to 2024. Meningitis and/or ventriculitis were confirmed according to clinical characteristics and positive results of CSF culture. Antenatal, demographic and delivery characteristics, clinical features and comorbidities, as well as bacteriological findings in CSF and neurosonography findings were analyzed from data in medical history of patients.
Detailed data obtained from the medical history included type of conception, number of pregnancy, type of pregnancy (singleton, twin, triplet), age of mother and mother’s diseases and conditions during pregnancy, such as chorioamnionitis, urinary tract infection, PROM and placental abruption. Other demographic and perinatal data about neonates included sex, gestational age, mode of delivery, BW, Apgar score at first minute and fifth minutes after birth, and need for endotracheal intubation (ET) at birth. Postnatal data about neonate’s clinical features and comorbidities included need for invasive mechanical ventilation (MV) and high-frequency oscillatory ventilation (HFOV), the use of inotropic support, neonatal sepsis and meningitis, ventriculitis, pneumonia, pulmonary hemorrhage, pneumothorax, neonatal seizures, necrotizing enterocolitis requiring surgical treatment, patent ductus arteriosus requiring treatment (medical, surgical or both), bronchopulmonary dysplasia, retinopathy of prematurity treated by intravitreal application of anti–vascular endothelial growth factor (anti-VEGF), the use of red blood cell transfusion for anemia and the use of fresh frosen plasma for various hemorrhage (pulmonary, gastrointestinal, et al.). Also, CSF cultures and cranial ultrasound findings were analyzed. Mortality rate was recorded. Data were analyzed using SPSS (ver. 27.0).
Results
The neonates with meningitis and/or ventriculitis caused by GPB treated at our hospital during a period of 15 years, 12 of them, were included in this retrospective study. All included neonates were tranfered in our hospital, 10 (83.3%) from tertiary Maternity Ward and 2 (16.7%) from secondary Maternity Ward. In our sample, 10 (83.3%) pregnancy were singleton and there were two neonates from a twin pregnancy. One pregnancy was achieved with assisted reproductive technology. Ten (83.3%) neonates were born from controlled pregnancy and 6 (50%) mothers were primigravida. The median age of mother was 30.6 (ranged 22 – 43). Four (33.3%) mothers were diagnosed with cervico-vaginal infection and one mother had placental abruption. Two mothers presented with PROM. One pregnancy was complicated by twin-to-twin transfusion syndrome.
Out of a total of 12 included neonates were born preterm, and eight (66.7%) of them were born before 28 weeks of gestation (GW). The median gestational age (GA) was 27.3 (ranged 24.0 – 36.0) and median BW 1019.2 g (ranged 710 – 2200 g). Demographic and delivery characteristics of included neonates are presented in Table 1.
Table 1. Demographic and delivery characteristics of included neonates
|
Mode of delivery vaginal delivery caesarean section |
4 (33.3%) 8 (66.7%) |
|
Sex male female |
2 (16.7%) 10 (83.3%) |
|
Classification of neonates by gestational age extremely preterm (< 28) very preterm (28 – 31+6/7) moderate preterm (32 – 33+6/7) late preterm (34 – 36+6/7) full-term (≥ 37) |
8 (66.7%) 3 (25.0%) 0 (0.0%) 1 (8.3%) 0 (0.0%) |
|
Classification of neonates by birth weight extremely low birth weight (< 1000 g) very low birth weight (1000 – 1499 g) low birth weight (1500 – 2499 g) normal (2500 – 4000 g) |
8 (66.7%) 3 (25.0%) 1 (8.3%) 0 (0.0%) |
|
Apgar score at first minute of life 0 – 3 4 – 7 8 – 10 |
4 (33.3%) 7 (58.3%) 1 (8.3%) |
|
Apgar score at fifth minute of life 0 – 3 4 – 7 8 – 10 not determined |
0 (0.0%) 10 (83.3%) 0 (0.0%) 2 (16.7%) |
|
Endotracheal intubation at birth |
10 (83.3%) |
All included neonates had late-onset sepsis, complicated by meningitis in 7 (58.3%) cases. Five (41.7%) neonates developed ventriculitis after Ommaya subcutaneous reservoir (SCR) implantation, well-known in literature as shunt-related ventriculitis. In our cohort, there were five (41.7%) neonates diagnosed with pneumonia.
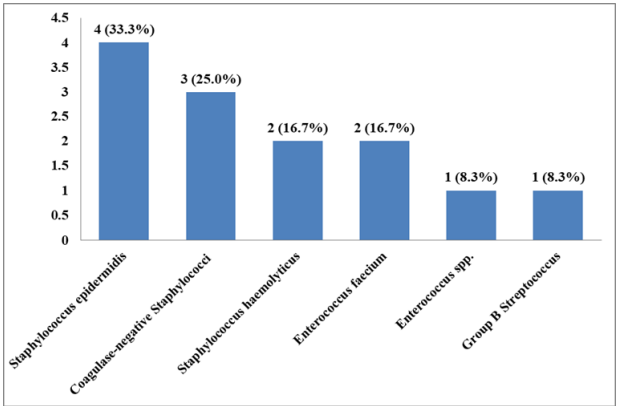
The neonatal meningitis and/or ventriculitis was caused by GPB from genus Staphylococcus, in 9 (75.0%) neonates. Three (25.0%) of included neonates had meningitis and/or ventriculitis caused by bacteria from genus Enterococcus. In one neonate, meningitis was caused by GBS. One neonate had ventriculitis twice, caused by two different bacteria, Enterococcus faecium and CoNS. Th most common causes of meningitis were Gram-positive bacteria from the genus Staphylococcus. Staphylococcus epidermidis was the most common cause of ventriculitis in neonates with posthemorrhagic ventricular dilatation (PHVD) treated with Ommaya SCR implantation. Etiology of meningitis and/or ventriculitis in our sample are presented in Chart 1.
Chart 1. Etiology of neonatal meningitis and/or ventriculitis
Ten (83.3%) of these neonates required ET at birth, but in other two neonates, who initially received non-invasive ventilation, ET and MV were required during hospitalization due to respiratory failure. A third of these neonates, 4 (33.3%), required the use of HFOV. Clinical features and comorbidities of these neonates are presented in Table 2.
Table 2. Clinical features and comorbidities of included neonates
|
Hypotension requiring inotroping drugs |
4 (33.3%) |
|
Patent ductus arteriosus |
6 (50.0%) |
|
Pulmonary hemorrhage |
2 (16.7%) |
|
Pneumothorax |
1 (8.3%) |
|
Bronchopulmonary dysplasia |
8 (66.7%) |
|
Neonatal seizures |
7 (58.3%) |
|
Anemia corrected with red blood cell transfusion |
12 (100.0%) |
|
Hemorrhage corrected with fresh frosen plasma |
2 (16.7%) |
|
Necrotizing enterocolitis |
1 (8.3%) |
|
Retinopathy of prematurity |
5 (41.7%) |
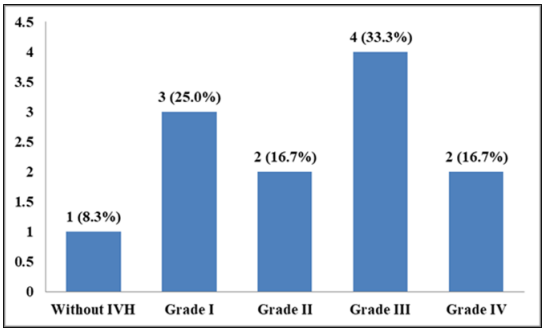
The most common structural lesion diagnosed by cranial ultrasound (CUS) was intraventricular hemorrhage (IVH), in 11 (91.7%). The frequency of IVH according to the Volpe's classification is shown in Chart 2.
Chart 2. The frequency of intraventricular hemorrhage
In 7 (58.3%) neonates, CUS showed PVHD. In one neonate, ventriculomegaly was transient, 6 (50.0%) of these neonates required neurosurgical treatment, implantation of Ommaya SCR and/or ventriculoperitoneal (VP) shunt. Five neonates diagnosed with ventriculitis had a similar CUS findings highly suggestive associated with inflammation of the choroid plexus and ependyma covering the lateral ventricles. This CUS findings include increased thickness, irregularity and echogenicity of the ependyma, the presence of intraventricular debris and stranding and fibrin sept formation in lateral ventricles.
In our cohort, one neonate died due to sepsis and multiple organ dysfunction syndrome.
Discussion
Meningitis is one of the important causes of mortality and morbidity in neonates. During the last few decades, advances in antenatal and neonatal intensive therapy and care, survival of preterm neonates and low birth weight neonates have increased. These group of neonates are more susceptible to bacterial meningitis than full-term neonates and older children (3,6,9). In this retrospective study, it was identified 12 neonates with meningitis and/or ventriculitis caused by GPB. Our data indicated that CNS infection caused by GPB is found predominantly in female neonates. In our sample, all neonates were born before 37 GW and more than half were extremely preterm neonates. There were neonates required ET intubation, the use of MV, prolonged hospitalization in the NICU and received several different antibiotics during hospitalization. Also, 6 (50.0%) of included neonates had neurosurgical treatment of PHVD. All of these are well-known risk factors for developing late-onset neonatal infection, after seventh day of life.
The bacterial distributions of neonatal meningitis and/or ventriculitis caused by GPB in our cohort were consistent with those reported in previous studies (6,16-18). In our study, bacteria from genus Staphylococcus were the most commonly detected by CSF culture. Other bacteria were GBS and Enterococcus spp. In consistent with the increased survival of preterm neonates, especially low birth weight neonates, CoNS is now represent one of the major nosocomial microorganism and important cause of late-onset sepsis and meningitis (3). Jean-Baptiste N, et al. (19) in retrospective cohort study reported that CoNS infection was inversely related to GA and BW. Drinkovic D, et al. (20) reported of successfully treated CoNS meningitis in two extremely preterm neonates without shunt for CSF drainage. In our study, two neonates were diagnosed with CoNS meningitis. One of them was born at 29 GW and second neonate with CoNS meningitis was late-preterm, born at 36 GW. Coagulase-negative Staphylococci was identified as a cause of ventriculitis in one extremely preterm neonate, born at 26 GW, treated PHVD with Ommaya SCR implantation.
Staphylococcus epidermidis is a common microorganism causing hospital-acquired infections in many NICU. Central nervous system infections caused by Staphylococcus epidermidis were most frequently reported in neonates particularly in association with neurosurgical procedures, such as intraventricular catheters implantation (3,21,22). In this study, there were four (33.3%) neonates with ventriculitis caused by Staphylococcus epidermidis. All of these neonates had PHVD and required temporary CSF drainage with Ommaya SCR. Ventricular puncture was performed by a neurosurgeon. In three neonates, CSF analysis showed pleocytosis, hyperproteinorachia and hypoglycorrhachia, but one neonate had unremarkable CSF white blood cell counts, glucose and protein concentrations.
In this analysis, there were no identified Staphylococcus aureus as a cause of meningitis and/or ventriculitis in neonates. Meningitis due to Staphylococcus aureus is relatively uncommon, accounting about 10% of cases of bacterial neonatal meningitis. It is found that Staphylococcus aureus, as a cause of neonatal meningitis, occurs in a wide variety of patological condition, such as hydrocephalus and presence the shunts for CSF drainage, cranial trauma and after neurosurgical procedures (3,23,24).
Bateria from genus Enterococcus are unusual cause of neonatal CNS infections. However, in recent years, Enterococci have become a significant cause of hospital-acquired infections. The main risk factors for enterococcal infections in neonates are prematurity and prolonged hospitalization in NICU (25,26). In our study, it was identified extremely preterm neonate, born at 25.5 GW with BW of 900 g, with late-onset sepsis complicated by meningitis and ventriculitis caused by vancomycin-resistant Enterococcus faecium. In addition to their high resistance in the external environment, Enterococci are resistant to numerous antibiotics from different groups, so the treatment of enterococcal infections is a major challenge for neonatologists (27,28).
In neonates, GBS is well-known cause of early-onset meningitis, community-acquired and hospital-acquired late-onset meningitis. Group B Streptococcus (Streptococcus agalactiae) is a commensal microorganism of the normal vaginal and gut microbiome of healthy adults. It is estimated that GBS is present in the vagina and/or rectum, of up to 40% of healthy pregnant women, but maternal GBS colonization is the most important risk factor for neonatal infection (29,30). Similary, in our study, one extremely preterm neonate born from prenancy complicated with maternal GBS colonization, had late-onset sepsis and meningitis caused by GBS, presented with status epilepticus. In some developed countries, GBS has become the common cause of late-onset neonatal disease. Other risk factors for neonatal GBS infection are prematurity, young maternal age, African ethnicity and exposure to Human Immunodeficiency Virus (31). Ueda NK, et al. (32) reported a case of neonatal GBS meningitis and recurrent bacteremia transmitted via the contaminated breast milk caused by maternal mastitis. However, the breastfeeding as a risk factor for GBS infection in neonates has been reported only in case reports and case series, but its role has not yet been confirmed by evidence-based data. It is similar with the twin delivery as a risk factor for GBS infection in neonatal age (31,33). In contrast to early-onset infection, which is acquired predominantly by vertical transmission, late-onset neonatal GBS infection is acquired both vertically and horizontally (31,34,35). Neonatal GBS meningitis can cause significant neurological morbidity and mortality, and because of that, prevention is very important. The most important preventive strategy is universal screening for maternal GBS colonization to 360/7 to 376/7 GW and receiving appropriate intrapartum antibiotic prophylaxis in positive cases (36).
Despite advances in neonatal intensive therapy and the decrease in mortality, it remains significantly high in developing countries, of up to 60%. In contrast, mortality in developed countries is 10-15%, with a significantly higher rate in preterm neonates (5,37,38). In our analysis, there was one extremely preterm neonate with a fatal outcome.
Conclusion
Prematurity and prolonged hospitalization in NICU are the main risk factors for late-onset neonatal sepsis and meningitis caused by GPB. Neonates with PHVD are at strong risk for ventriculitis. Gram-positive bacteria from genus Staphylococcus was the most common cause of neonatal CNS infections. Early diagnosis and appropriate causal and symptomatic therapy reduce complications and neurological sequelae in later life.
Funding information
The author did not receive any funding for this publication.
Financial Disclosure
The author have no financial relationships relevant to this article to disclose.
Conflict of Interest
The author declare that there is no conflict of interest.
References
1. Ellika SK, Desai SV. Neonatal Central Nervous System Infection. J Pediatr Neurol: 2017; 15(05): 201-20.
2. Schneider, J.F. Neonatal brain infections. Pediatr Radiol: 2011; 41(Suppl 1):143–48.
3. de Vries LS, Volpe JJ. Bacterial and Fungal Intracranial Infections. In: Volpe JJ, Inder TE, Darras BT, de Vries LS, du Plessis AJ, Ferriero DM, et al. editors. Volpe’s Neurology of the Newborn. 7th ed. Philadelphia: Elsevier; 2024. p.1209-49.
4. Berardi A, Lugli L, Rossi C, China MC, Vellani G, Contiero R, et al. Neonatal bacterial meningitis. Minerva Pediatr. 2010;62(3 Suppl 1):51-4.
5. Ku LC, Boggess KA, Cohen-Wolkowiez M. Bacterial meningitis in infants. Clin Perinatol. 2015;42(1):29-45, vii-viii.
6. Zhai Q, Li S, Zhang L, Yang Y, Jiang S, Cao Y. Changes in pathogens of neo¬natal bacterial meningitis over the past 12 years: a single-center retrospective¬study. Transl Pediatr. 2022;11(10):1595-1603.
7. Biset S, Benti A, Molla L, Yimer S, Cherkos T, Eyayu Y, et al. Etiology of Neonatal Bacterial Meningitis and Their Antibiotic Susceptibility Pattern at the University of Gondar Comprehensive Specialized Hospital, Ethiopia: A Seven-Year Retrospective Study. Infect Drug Resist. 2021;14:1703-11.
8. Smith PB, Garges HP, Cotton CM, Walsh TJ, Clark RH, Benjamin DK Jr. Meningitis in preterm neonates: importance of cerebrospinal fluid parameters. Am J Perinatol. 2008;25(7):421-6.
9. Aleem S, Greenberg RG. When to Include a Lumbar Puncture in the Evalua¬tion for Neonatal Sepsis. Neoreviews. 2019;20(3):e124-e134.
10.Parlakay G, Çak?r SÇ, Dorum BA, Özkan H, Çelebi S, Hac?mustafao?lu M, et al. Evaluation of Risk and Prognostic Factors in Neonatal Meningitis. J Curr Pediatr. 2023;21(1):16-22.
11.Khalessi N, Afsharkhas L. Neonatal meningitis: risk factors, causes, and neu¬rologic complications. Iran J Child Neurol. 2014;8(4):46-50.
12.Swanson D. Meningitis. Pediatr Rev. 2015; 36(12): 514–26.
13.Hasbun R. Progress and Challenges in Bacterial Meningitis: A Review. JAMA. 2022;328(21):2147-54.
14. Nash C, Chu A, Bhatti M, Alexander K, Schreiber M, Hageman JR. Coagulase Negative Staphylococci in the Neonatal Intensive Care Unit: Are We Any Smarter?. Neoreviews. 2013; 14(6): e284–e293.
15. Marchant EA, Boyce GK, Sadarangani M, Lavoie PM. Neonatal sepsis due to coagulase-negative staphylococci. Clin Dev Immunol. 2013;2013:586076.
16. Erickson TA, Munoz FM, Troisi CL, Nolan MS, Hasbun R, Brown EL, et al. The Epidemiology of Meningitis in Infants under 90 Days of Age in a Large Pediatric Hospital. Microorganisms. 2021;9(3):526.
17. Ouchenir L, Renaud C, Khan S, Bitnun A, Boisvert AA, McDonald J, et al. The Epidemiology, Management, and Outcomes of Bacterial Meningitis in Infants. Pediatrics. 2017;140(1):e20170476.
18. Wong CH, Duque JR, Wong JSC, Chan CV, Lam CSI, Fu YM, et al. Epidemiology and Trends of Infective Meningitis in Neonates and Infants Less than 3 Months Old in Hong Kong. Int J Infect Dis. 2021;111:288-294.
19. Jean-Baptiste N, Benjamin DK Jr, Cohen-Wolkowiez M, Fowler VG Jr, Laughon M, Clark RH, et al. Coagulase-negative staphylococcal infections in the neonatal intensive care unit. Infect Control Hosp Epidemiol. 2011;32(7):679-86.
20. Drinkovic D, Pottumarthy S, Knight D, Morris AJ. Neonatal coagulase-negative staphylococcal meningitis: a report of two cases. Pathology 2002;34(6):586-88.
21. Gruskay J, Harris MC, Costarino AT, Polin RA, Baumgart S. Neonatal Staphylococcus epidermidis meningitis with unremarkable CSF examination results. Am J Dis Child. 1989;143(5):580-2.
22. Ongun H, Kihtir Z, Zarif Ozkan N, Koyuncu Ozyurt O, Kara Tural T, Celik K, et al. Challenges in Diagnosis and Treatment of Neonatal Ventriculitis: A Case Report and Systematic Review of Difficult-to-Treat Central Nervous System Infection Resistant to Conventional Therapy. J Pediatr Infect Dis. 2024;19(03):127-39.
23. Giannoni E, Agyeman PKA, Stocker M, Posfay-Barbe KM, Heininger U, Spycher BD, et al. Neonatal Sepsis of Early Onset, and Hospital-Acquired and Community-Acquired Late Onset: A Prospective Population-Based Cohort Study. J Pediatr. 2018;201:106-114.e4.
24. Kim JH, van der Horst C, Mulrow CD, Corey GR. Staphylococcus aureus meningitis: review of 28 cases. Rev Infect Dis. 1989;11(5):698-706.
25. Furtado I, Xavier PC, Tavares LV, Alves F, Martins SF, Martins Ade S, et al. Enterococcus faecium and Enterococcus faecalis in blood of newborns with suspected nosocomial infection. Rev Inst Med Trop Sao Paulo. 2014;56(1):77-80.
26. Bretón JR, Peset V, Morcillo F, Cano J, Sarrión A, Pérez-Belles C, et al. Meningitis neonatal por Enterococcus spp.: presentación de cuatro casos [Neonatal meningitis due to Enterococcus spp.: presentation of four cases]. Enferm Infecc Microbiol Clin. 2002;20(9):443-7.
27. Marom R, Mandel D, Haham A, Berger I, Ovental A, Raskind C, et al. A silent outbreak of vancomycin-resistant Enterococcus faecium in a neonatal intensive care unit. Antimicrob Resist Infect Control. 2020;9(1):87.
28. Said MS, Tirthani E, Lesho E. Enterococcus Infections. 2025. In: StatPearls [Internet]. Available at: https://pubmed.ncbi.nlm.nih.gov/33620836/ (Accessed on March 20, 2025).
29. Tavares T, Pinho L, Bonifácio Andrade E. Group B Streptococcal Neonatal Meningitis. Clin Microbiol Rev. 2022;35(2):e0007921.
30. Bundy LM, Rajnik M, Noor A. Neonatal meningitis. 2025. In: StartPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK532264/ (Accessed on March 20, 2025)
31. Miselli F, Frabboni I, Di Martino M, Zinani I, Buttera M, Insalaco A, et al. Transmission of Group B Streptococcus in late-onset neonatal disease: a narrative review of current evidence. Ther Adv Infect Dis. 2022;9:20499361221142732.
32. Ueda NK, Nakamura K, Go H, Takehara H, Kashiwabara N, Arai K, et al. Neonatal meningitis and recurrent bacteremia with group B Streptococcus transmitted by own mother's milk: A case report and review of previous cases. Int J Infect Dis. 2018;74:13-15.
33. Berardi A, Trevisani V, Di Caprio A, Bua J, China M, Perrone B, et al. Understanding Factors in Group B Streptococcus Late-Onset Disease. Infect Drug Resist. 2021;14:3207-18.
34. Lin FY, Weisman LE, Troendle J, Adams K. Prematurity is the major risk factor for late-onset group B streptococcus disease. J Infect Dis. 2003;188(2):267-71.
35. Morgan K, Baca N. Late-Onset Group B Streptococcal Meningitis in Infants. Pediatr Neurol. 2015;53(2):175-6.
36. Dhudasia MB, Flannery DD, Pfeifer MR, Puopolo KM. Updated Guidance: Prevention and Management of Perinatal Group B Streptococcus Infection. Neoreviews. 2021;22(3):e177–e188.
37. van der Flier M. Neonatal meningitis: small babies, big problem. Lancet Child Adolesc Health. 2021;5(6):386-87.
38. Nakwa FL, Lala SG, Madhi SA, Dangor Z. Neurodevelopmental Impairment at 1 Year of Age in Infants With Previous Invasive Group B Streptococcal Sepsis and Meningitis. Pediatr Infect Dis J. 2020;39(9):794-98.