Pancreatic Heterotopia in the Gallbladder: A Rare Case Report
Pancreatic Heterotopia in the Gallbladder: A Rare Case Report
Dr. Murtaza Makasarwala *
*Correspondence to: Dr. Murtaza Makasarwala, Consultant Robotic Advanced Laparoscopic GI and Laser surgeon, Shalby Hospital, Adajan, near navyug college, Surat-395009, India.
Copyright
© 2025 Dr. Murtaza Makasarwala. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 12 May 2025
Published: 19 May 2025
DOI:https://doi.org/10.5281/zenodo.15686606
Abstract
Introduction: Pancreatic heterotopia is an uncommon congenital anomaly wherein pancreatic tissue is present outside its normal anatomical location and without vascular or ductal continuity. While heterotopic pancreatic tissue is often identified incidentally within the gastrointestinal tract, its presence in the gallbladder is extremely rare.
Case Presentation: We report the case of a 51-year-old Arab woman with recurrent biliary colic and chronic right upper quadrant pain.
Investigations: Laboratory analysis was largely unremarkable, except for elevated gamma-glutamyl transferase (GGT). Imaging confirmed cholelithiasis without biliary obstruction.
Intervention: Laparoscopic cholecystectomy was performed.
Results: Histopathological analysis revealed Heinrich Type II pancreatic heterotopia near the cystic duct margin.
Conclusion: Due to its asymptomatic nature, pancreatic heterotopia is frequently an incidental finding diagnosed only postoperatively via histopathology. Nevertheless, awareness of this anomaly is essential for pathologists and surgeons to ensure complete excision and rule out malignant potential.
Pancreatic Heterotopia in the Gallbladder: A Rare Case Report
Introduction
Pancreatic heterotopia is defined as the presence of pancreatic tissue in ectopic sites, isolated from the orthotopic pancreas and lacking anatomical or vascular continuity. Although rare, it has been identified in various parts of the gastrointestinal tract, most notably the stomach, duodenum, and jejunum. Its occurrence in the gallbladder is exceedingly uncommon, with fewer than 40 cases documented globally since its first report by Otschkin in 1916.
The condition is predominantly asymptomatic and is often discovered incidentally during histopathological evaluation following cholecystectomy. When symptomatic, it may mimic biliary colic, presenting with epigastric or right upper quadrant pain—often leading to a misdiagnosis of cholelithiasis or cholecystitis.
Embryologically, pancreatic heterotopia is considered a migration anomaly. During the 7th to 8th weeks of gestation, abnormal rotation of the foregut can result in pancreatic tissue embedding into ectopic regions. The misplacement theory—suggesting displacement of pancreatic tissue during embryogenesis—is the most widely accepted explanation.
Histologically, heterotopic pancreas has been classified by Heinrich into three types:
• Type I: Contains acini, ducts, and islets of Langerhans (resembling normal pancreas).
• Type II: Composed of acini and ducts, without islets.
• Type III: Contains predominantly ducts with few or absent acini and no islets.
The present case highlights a rare presentation of Heinrich Type II pancreatic heterotopia in the gallbladder of a middle-aged woman, diagnosed only postoperatively. The aim of this report is to contribute to the limited pool of literature and reinforce the importance of histopathological evaluation in cases of cholelithiasis.
Case Presentation
Patient Profile and Clinical History
A 51-year-old medically free Arab woman presented with a four-year history of chronic intermittent epigastric pain, which progressively localized to the right upper quadrant and radiated to the right subscapular area. Her symptoms were consistent with biliary colic.
Clinical Findings
Physical examination revealed no significant abnormalities. There were no signs of jaundice or peritonitis. The patient was otherwise healthy.
Investigations
Laboratory Tests
Routine blood work including complete blood count and differential were within normal limits. Liver function tests were also unremarkable except for an elevated gamma-glutamyl transferase (GGT) at 144 IU/L (normal: 5–39 IU/L).
Imaging
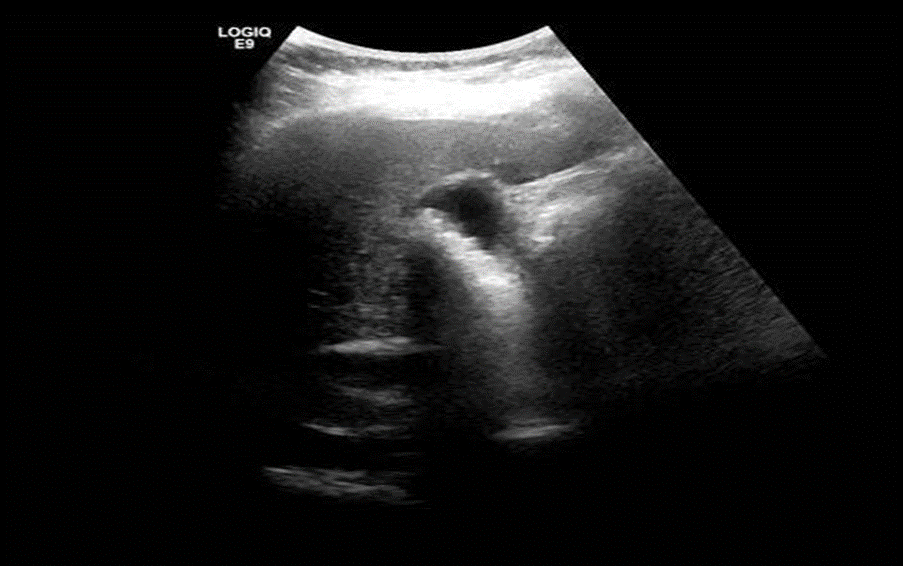
An abdominal ultrasound revealed multiple tiny gallstones within the gallbladder without any evidence of intrahepatic or extrahepatic biliary dilation. The liver was normal in size and echotexture, and no ascites were noted.
Figure 1: Ultrasound of 51-year-old female with pancreatic heterotopia in the gallbladder demonstrates innumerable tiny stones within the gallbladder but no intrahepatic or extrahepatic biliary tree dilation.
Intervention
The patient underwent an uncomplicated laparoscopic cholecystectomy. No intraoperative complications were noted.
Histopathological Findings
The resected gallbladder demonstrated multiple small pigmented stones and a whitish nodule measuring 1.3 cm near the cystic duct margin. Histological examination of the nodule confirmed heterotopic pancreatic tissue composed of acini and ducts but lacking islets of Langerhans, consistent with Heinrich Type II heterotopia.
Other findings included:
·Serosal congestion
·Denuded mucosa
·Wall thickness: 0.3 cm
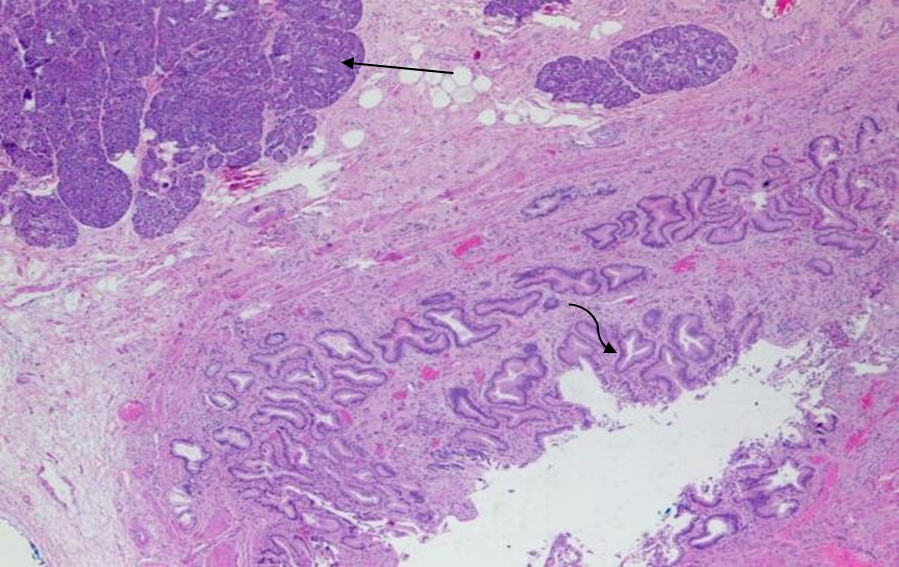
Figure 2 Histopathology of pancreatic heterotopia in the gallbladder of a 51-year-old woman using a hematoxylin and eosin stain demonstrates mucin secreting columnar epithelium lining the cystic duct (curved arrow) and pancreatic tissue (straight arrow). [100x view]
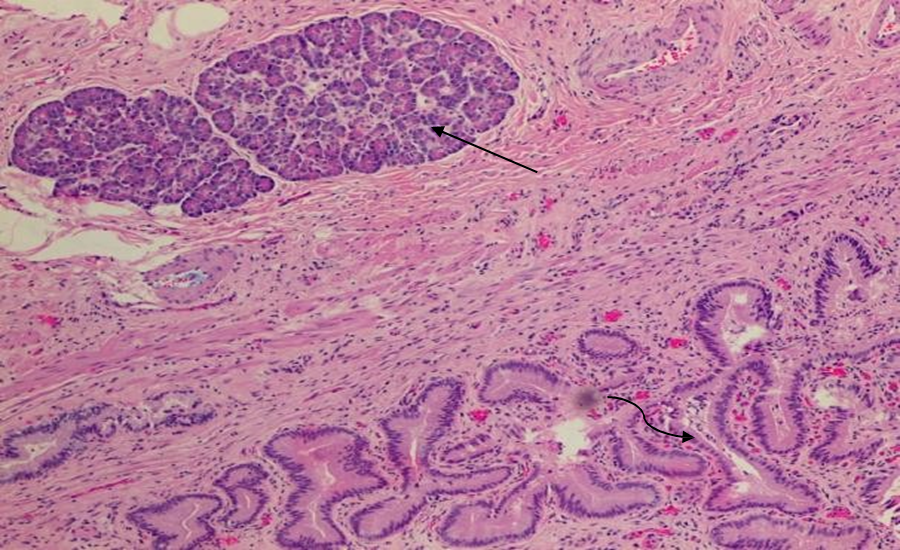
Figure 3 Histopathology of pancreatic heterotopia in the gallbladder of a 51-year-old woman using a hematoxylin and eosin stain demonstrates mucin secreting columnar epithelium lining the cystic duct (curved arrow) and pancreatic tissue (straight arrow). [100x view]
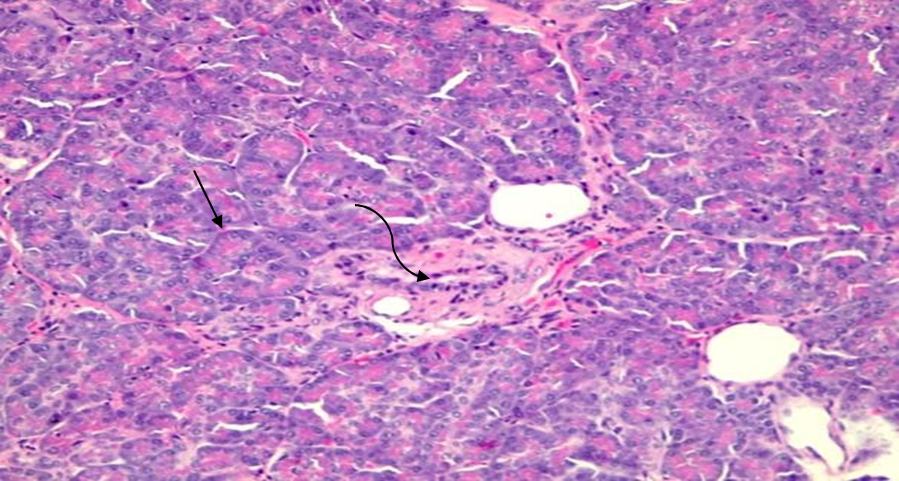
Figure 4 Histopathology of pancreatic heterotopia in the gallbladder of a 51-year-old woman using a hematoxylin and eosin stain demonstrates benign pancreatic tissue with acini (straight arrow) and ducts (curved arrow). No Langerhans islets are identified. [400x view]
Discussion
Pancreatic heterotopia, particularly in the gallbladder, remains a rare and poorly understood entity within gastrointestinal pathology. The clinical significance of this anomaly extends beyond its rarity; it presents a unique diagnostic challenge due to its asymptomatic or non-specific nature, and its potential for pathological complications. While the condition is typically benign, its presentation can closely mimic more common gallbladder diseases, leading to misdiagnosis or underreporting.
Epidemiology and Gender Disparity
Pancreatic heterotopia is reported in 0.55–13.7% of autopsy cases, with the most common ectopic sites being the stomach (especially the antrum), duodenum, and jejunum. However, its prevalence in the gallbladder is extremely rare, with less than 40 documented cases in the literature. Interestingly, although pancreatic heterotopia in general is slightly more frequent in males, heterotopia involving the gallbladder demonstrates a female predominance. This gender discrepancy may be attributable to the higher incidence of cholelithiasis and biliary diseases in women, which increases the likelihood of undergoing cholecystectomy, thereby raising the chance of incidental histopathologic detection.
Embryological Considerations
The pathogenesis of pancreatic heterotopia is rooted in embryological maldevelopment. During the 7th and 8th weeks of gestation, the pancreas forms from two separate buds—the dorsal and ventral buds. Improper rotation, migration, or sequestration of these pancreatic buds during gastrointestinal organogenesis can lead to ectopic implantation of pancreatic tissue. The misplacement theory, as proposed by Gaspar Fuentes and others, suggests that fragments of pancreatic tissue may be displaced during embryogenesis, especially in the vicinity of the biliary system, leading to anomalies like heterotopia.
Clinical Presentation and Diagnostic Challenges
Clinically, most cases of gallbladder pancreatic heterotopia are silent and discovered only upon histological examination of cholecystectomy specimens. When symptoms are present, they are indistinguishable from those of cholelithiasis or chronic cholecystitis. Patients may present with epigastric discomfort, right upper quadrant pain, nausea, or vomiting. In rare instances, complications such as cystic duct obstruction, acute pancreatitis within the heterotopic tissue, or even carcinoma arising in the ectopic site have been reported.
Our patient exhibited classical biliary colic symptoms without any signs suggestive of a heterotopic lesion. Laboratory parameters were largely unremarkable, with the exception of elevated GGT—a finding more likely associated with biliary stasis due to cholelithiasis rather than heterotopic tissue itself. Similar findings have been reported in the literature, including a case by Inceoglu et al. (2002), where a patient with heterotopic pancreas in the gallbladder neck developed acute hydrops due to ductal obstruction. Thus, while heterotopia is usually clinically silent, it may become symptomatic if it interferes with biliary dynamics.
Histopathological Classification and Implications
The diagnosis is histopathological and follows Heinrich’s classification:
·Type I: Consists of ducts, acini, and islets of Langerhans—replicating full pancreatic architecture.
·Type II: Contains only ducts and acini, without islets (as in our case).
·Type III: Comprises only pancreatic ducts.
Our case demonstrated Type II heterotopia, localized near the cystic duct, suggesting embryonic displacement during early foregut development. The absence of islets is noteworthy since it explains the lack of endocrine-related symptoms such as hypoglycemia or insulin-related manifestations. However, acinar tissue can still secrete digestive enzymes, which, if activated locally, may lead to inflammation or contribute to atypical symptoms like mucosal erosion or gallbladder wall thickening.
Potential for Malignancy
Although rare, there have been reports of malignant transformation in heterotopic pancreatic tissue, especially adenocarcinoma arising from the ductal epithelium. This potential warrants the complete excision of any ectopic pancreatic nodules encountered during surgery. Vigilant histopathological assessment is critical for distinguishing benign from potentially premalignant lesions. In this context, our case contributes to the ongoing discussion about the neoplastic potential of such tissues, albeit no atypia or malignant changes were identified in this instance.
Review of Literature and Clinical Correlation
A comprehensive review by Zhang et al. (2010), encompassing 184 cases of heterotopic pancreas, identified only one gallbladder instance—highlighting the extreme rarity. Similarly, Makhlouf et al. (1999) described five gallbladder cases in their series, all diagnosed retrospectively. These studies reinforce the importance of meticulous pathological evaluation of cholecystectomy specimens, particularly when mucosal nodularity or wall thickening is observed intraoperatively.
In our patient, the heterotopic nodule was small (1.3 cm), firm, and whitish, and would have been easily overlooked without histological scrutiny. This further underscores the need for a high index of suspicion, especially in patients presenting with chronic biliary symptoms and no identifiable intraoperative complications.
Summary of Key Points
·Pancreatic heterotopia in the gallbladder is rare and usually asymptomatic.
·Its diagnosis depends solely on histopathological examination post-cholecystectomy.
·Awareness among surgeons and pathologists is critical to avoid misdiagnosis.
·Potential complications include inflammation, obstruction, and rare malignant transformation.
Conclusion
Pancreatic heterotopia of the gallbladder is a rare congenital anomaly that poses diagnostic challenges due to its asymptomatic nature and non-specific presentation. While typically benign and discovered incidentally post-surgery, it can present with complications if left unrecognized. Surgeons and pathologists should maintain an awareness of this entity, especially in cholecystectomy specimens, to ensure accurate diagnosis and appropriate management.
References
1. Pendharkar D, Khetrapal S, Jairajpuri Z, Rana S, Jetley S. Pancreatic and gastric heterotopia in the gallbladder: A rare incidental finding. Int J Appl Basic Med Res. 2019;9(2):115. doi:10.4103/ijabmr.ijabmr_109_18
2. Pilloni L, Cois A, Uccheddu A, Ambu R, Coni P, Faa G. Complete pancreatic heterotopia of gallbladder with hypertrophic duct simulating an adenomyoma. World J Gastroenterol. 2006;12(11):1786-1787. doi:10.3748/wjg.v12.i11.1786
3. Basrur GB, Utture SK, Deshpande AA. Heterotopic Pancreas in the Gallbladder. Indian J Surg. 2016;78(5):429-430. doi:10.1007/s12262-016-1561-3
4. Elhence P, Bansal R, Agrawal N. Heterotopic pancreas in gall bladder associated with chronic cholecystolithiasis. Int J Appl Basic Med Res. 2012;2(2):142. doi:10.4103/2229- 516x.106360
5. Rezvani M, Menias C, Sandrasegaran K, Olpin JD, Elsayes KM, Shaaban AM. Heterotopic pancreas: Histopathologic features, imaging findings, and complications. Radiographics. 2017;37(2):484-499. doi:10.1148/rg.2017160091
6. Jiang K, Stephen FO, Jeong D, Pimiento JM. Pancreatic and gastric heterotopia with associated submucosal lipoma presenting as a 7-cm obstructive tumor of the ileum: Resection with double balloon enteroscopy. Case Rep Gastroenterol. 2015;9(2):233-240. doi:10.1159/000437047
7. Ferhatoglu MF, Kivilcim T, Kartal A, Filiz AI. A Rare Pathology Mimicking the Gallstone: Heterotopic Pancreas in the Gallbladder. Cureus. 2018;10(5):e2659. doi:10.7759/cureus.2659
8. Koukourakis IM, Perente Memet MS, Kouroupi M, Simopoulos K. Ectopic Pancreatic Tissue Adherent to the External Gallbladder Wall. Case Rep Gastroenterol. 2018;12(1):170-175. doi:10.1159/000488445
9. Sharma SP, Sohail SK, Makkawi S, Abdalla E. Heterotopic pancreatic tissue in the gallbladder. Saudi Med J. 2018;39(8):834-837. doi:10.15537/smj.2018.8.22602
10. Arora A, Singh P, Anand N, Husain N. Heterotopic pancreatic tissue associated with type 1 choledochal cyst, cystolithiasis and gall bladder stones: a rare entity with review of literature. BMJ Case Rep. 2017;2017:bcr-2016-218329. doi:10.1136/bcr-2016-218329
11. Inceoglu R, Dosluoglu HH, Kullu S, Ahiskali R, Doslu FA. An unusual cause of hydropic gallbladder and biliary colic - Heterotopic pancreatic tissue in the cystic duct: Report of a case and review of the literature. Surg Today. 1993;23(6):532-534. doi:10.1007/BF00730630
12. Elpek GÖ, Bozova S, Küpesiz GY, Ö?ü? M. An unusual cause of cholecystitis: Heterotopic pancreatic tissue in the gallbladder. World J Gastroenterol. 2007;13(2):313-315. doi:10.3748/wjg.v13.i2.313.