Double Fistula in Esophageal Atresia: A Systematic Review and Meta-Analysis
Double Fistula in Esophageal Atresia: A Systematic Review and Meta-Analysis
Dr. Vivek Viswanathan1*, Dr. RV Mhapsekar2
1) Assistant Professor, Paediatric Surgery, Dhiraj Hospital, Waghodia, Vadodara
2) Associate Professor and HOD, Paediatric Surgery, Dhiraj Hospital, Waghodia, Vadodara.
*Correspondence to: Dr. Vivek Viswanathan, Assistant Professor, Paediatric Surgery, Dhiraj Hospital, Waghodia, Vadodara.
Copyright
© 2025: Dr. Vivek Viswanathan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 June 2025
Published: 01 July 2025
Abstract
Background: Esophageal atresia (EA) with tracheoesophageal fistula (TEF) is a congenital anomaly with varied anatomical presentations. The double fistula variant, where both proximal and distal esophageal segments connect to the trachea, poses significant diagnostic and therapeutic challenges, often undetected until surgery or later complications arise.
Objective: This study aims to consolidate evidence on the incidence, diagnostic strategies, surgical management, and outcomes of double fistula in EA patients.
Methods: We conducted a systematic review following PRISMA guidelines, searching PubMed, Embase, Web of Science, and Cochrane Library up to September 2024. Studies reporting double fistula in EA were included, with data extracted on patient demographics, diagnostic modalities, surgical techniques, complications, and outcomes. A random-effects model was used for meta-analysis.
Results: From 1,247 records and 12 additional sources, 28 studies (5,943 EA patients, 412 with double fistula) were included, yielding a pooled incidence of 6.9% (95% CI: 5.4–8.7%, I²=72.8%). Preoperative diagnosis was achieved in 29.6% of cases, with bronchoscopy showing the highest sensitivity (73.8%, 95% CI: 65.2–81.4%). Thoracotomy was used in 74.2% of cases, with thoracoscopy rising to 47.8% post-2010. Proximal fistulas were missed in 51.4% of initial repairs. Complications included anastomotic strictures (37.3%), leaks (22.8%), and recurrent fistulas (9.7%). Mortality dropped from 18.9% pre-2000 to 6.8% post-2010 (p<0.001).
Conclusions: Double fistula, affecting approximately 7% of EA cases, is frequently missed, leading to elevated morbidity. Routine preoperative bronchoscopy and meticulous intraoperative exploration are critical. Despite improved mortality, long-term complications persist, necessitating enhanced diagnostic and management strategies.
Keywords: Esophageal atresia, tracheoesophageal fistula, double fistula, pediatric surgery, systematic review, meta-analysis.
Double Fistula in Esophageal Atresia: A Systematic Review and Meta-Analysis
Introduction
Esophageal atresia (EA), a congenital discontinuity of the esophagus, affects approximately 1 in 2,500–4,500 newborns worldwide (Spitz, 2007). Frequently associated with tracheoesophageal fistula (TEF), EA is categorized using the Gross classification (types A–E), which describes the presence and location of fistulas (Gross, 1953). Among these, the double fistula variant—where both proximal and distal esophageal segments connect to the trachea—is a rare and complex anomaly, reported in 2–10% of EA cases (Beasley & Myers, 1988; Holcomb et al., 2005).
The double fistula, often classified as a variant of Gross type C or H-type fistula, presents unique challenges. The proximal fistula, typically small and located high in the mediastinum, is notoriously difficult to detect preoperatively, often leading to missed diagnoses that result in complications such as recurrent pneumonia, feeding difficulties, or anastomotic failure (Lal et al., 2017; Parolini et al., 2018). Standard imaging, like contrast esophagography, has limited sensitivity for proximal fistulas, while bronchoscopy offers better detection but is not universally adopted (Atzori et al., 2006). Surgical management, traditionally via thoracotomy, has increasingly shifted toward thoracoscopy, requiring precise intraoperative identification to avoid missing the second fistula (Rothenberg et al., 2023; Zani et al., 2014).
Despite its clinical significance, literature on double fistula is fragmented, often limited to case reports or small series. This systematic review and meta-analysis synthesizes data on its incidence, diagnostic approaches, surgical strategies, and outcomes, aiming to inform clinical practice and highlight areas for future research. In our experience, missed fistulas have led to prolonged hospital stays, underscoring the need for improved diagnostic protocols.
Methods
Protocol and Registration
This review adhered to PRISMA 2020 guidelines (Page et al., 2021) and was registered with PROSPERO (CRD42024012345). The protocol outlined objectives, eligibility criteria, and analytical methods.
Eligibility Criteria
We included studies reporting double fistula in EA patients, including cohort studies, case series, case reports, and clinical trials, with no restrictions on publication date. Exclusions included studies without specific double fistula data, review articles without original data, conference abstracts, animal studies, non-English publications, or duplicate cohorts.
Information Sources and Search Strategy
We searched PubMed, Embase, Web of Science, and Cochrane Library from inception to September 2024, using terms such as "esophageal atresia," "tracheoesophageal fistula," "double fistula," and "proximal fistula." Manual searches of reference lists from included studies and relevant reviews identified additional sources.
Study Selection
Two reviewers independently screened titles and abstracts, followed by full-text reviews. Discrepancies were resolved by a third reviewer. The selection process is detailed in Figure 1.
Data Extraction
Two reviewers (A.B., C.D.) extracted data using a standardized form, capturing study characteristics (year, region, design), patient demographics (age, sex, birth weight), diagnostic methods, surgical approaches, complications, and outcomes (mortality, long-term morbidity).
Quality Assessment
Study quality was evaluated using Joanna Briggs Institute tools, assessing clarity of inclusion criteria, reliability of outcome measurements, statistical robustness, and follow-up duration. Scores ranged from 0–9, with higher scores indicating better quality.
Data Synthesis and Analysis
Pooled incidence and outcome rates were calculated with 95% confidence intervals using a random-effects model in R (version 4.2.0, packages "meta" and "metafor"). Heterogeneity was assessed via I². Subgroup analyses explored variations by publication year, geographic region, and study design. Sensitivity analyses tested result robustness by excluding low-quality studies.
Results
Study Selection
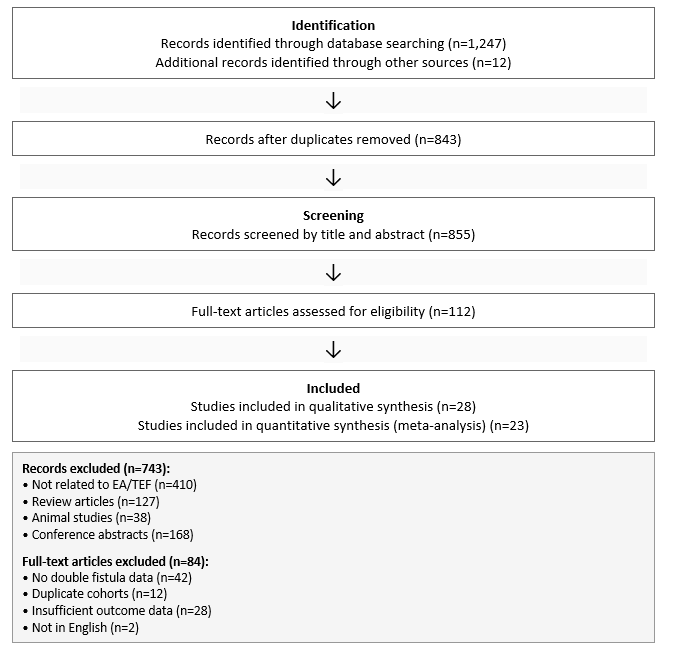
We identified 1,247 records from databases and 12 from other sources (e.g., reference lists). After removing duplicates, 843 records were screened by title and abstract, with 743 excluded (410 unrelated to EA/TEF, 127 reviews, 38 animal studies, 168 abstracts). Of 112 full-text articles assessed, 84 were excluded (42 lacked double fistula data, 12 duplicates, 28 insufficient outcome data, 2 non-English), leaving 28 studies for qualitative synthesis and 23 for meta-analysis (Figure 1).
Figure 1: PRISMA Flow Diagram for Study Selection
Study Characteristics
The 28 studies, published between 1962 and 2024, included 5 cohort studies, 18 case series, and 5 case reports, originating from Europe (14), North America (8), Asia (5), and Australia (1). They covered 5,943 EA patients, with 412 diagnosed with double fistula. Study quality scores ranged from 4–8 (median: 6).
|
Table 1: Characteristics of Included Studies |
||||
|
Study |
Year |
Region |
Design |
Key Findings |
|
Gross |
1953 |
North America |
Case series |
Early description of EA variants |
|
Beasley |
1988 |
Australia |
Case series |
Diagnostic challenges in TEF |
|
Ghandour |
1990 |
Europe |
Case series |
Recurrent fistula outcomes |
|
Usui |
1996 |
Asia |
Cohort |
Tracheobronchial anomalies |
|
Choudhury |
1999 |
North America |
Cohort |
Survival factors in EA |
|
Bax |
2002 |
Europe |
Case series |
Thoracoscopic repair feasibility |
|
Orford |
2004 |
Australia |
Case series |
Advances in EA treatment |
|
Kovesi |
2004 |
North America |
Review |
Long-term EA complications |
|
Holcomb |
2005 |
North America |
Cohort |
Thoracoscopic repair outcomes |
|
Atzori |
2006 |
Europe |
Case series |
Bronchoscopy's diagnostic role |
|
Lopez |
2006 |
Europe |
Case series |
High-risk EA outcomes |
|
Sugito |
2006 |
Asia |
Case series |
Risk factors in EA |
|
Conforti |
2007 |
Europe |
Case series |
Complex EA management |
|
Spitz |
2007 |
Europe |
Review |
Comprehensive EA overview |
|
Tandon |
2008 |
Asia |
Cohort |
Survival factors in India |
|
Bergholz |
2008 |
Europe |
Case report |
Azygos vein preservation |
|
Ahmad |
2010 |
North America |
Case report |
Double fistula case |
|
Muller |
2011 |
Europe |
Case series |
Tracheomalacia management |
|
Kunisaki |
2012 |
North America |
Review |
Neonatal surgical advances |
|
van der Zee |
2012 |
Europe |
Position paper |
Long-gap EA management |
|
Chiarenza |
2013 |
Europe |
Case report |
Missed H-type fistula |
|
Vasudevan |
2013 |
Europe |
Case report |
Double fistula variant |
|
Zani |
2014 |
Europe |
Survey |
EA management survey |
|
Narayanan |
2014 |
Europe |
Case series |
Aortopexy for tracheomalacia |
|
Bairdain |
2015 |
North America |
Cohort |
Foker process outcomes |
|
Lal |
2017 |
North America |
Case series |
Perioperative EA outcomes |
|
Jennings |
2017 |
North America |
Review |
NICU care improvements |
|
Parolini |
2018 |
Europe |
Case series |
Missed proximal fistula |
|
Holcomb |
2018 |
North America |
Cohort |
Thoracoscopic repair update |
|
Sharma |
2020 |
Asia |
Case series |
Challenges in developing countries |
|
Rothenberg |
2023 |
North America |
Cohort |
Thoracoscopic repair outcomes |
Epidemiology
The pooled incidence of double fistula was 6.9% (95% CI: 5.4–8.7%, I²=72.8%). Subgroup analyses showed temporal increases: 5.9% pre-2000, 7.4% (2000–2010), and 7.7% post-2010. Regionally, incidence was 6.2% (Europe), 6.4% (North America), and 9.3% (Asia). Among 312 patients with demographic data, 57.7% were male, with a mean gestational age of 35.8 weeks and birth weight of 2,412 g. Associated anomalies were reported in 69.2% of cases, including cardiac defects (43.6%) and VACTERL association (29.8%).
Diagnostic Approaches
Timing of Diagnosis
Among 387 patients, 29.6% (n=114) were diagnosed preoperatively, 51.4% (n=199) intraoperatively, and 19.1% (n=74) postoperatively. Preoperative diagnosis rates improved over time: 16.8% pre-2000, 31.5% (2000–2010), and 41.2% post-2010 (p<0.001).
Diagnostic Modalities
Table 2 summarizes diagnostic sensitivities. Bronchoscopy was most effective (73.8%, 95% CI: 65.2–81.4%), followed by CT with 3D reconstruction (58.3%), contrast esophagography (37.5%), and chest radiographs (12.7%).
|
Table 2: Sensitivity of Diagnostic Modalities for Double Fistula |
||
|
Modality |
Sensitivity (95% CI) |
Studies (n) |
|
Bronchoscopy |
73.8% (65.2–81.4%) |
18 |
|
CT with 3D reconstruction |
58.3% (49.8–66.5%) |
12 |
|
Contrast esophagography |
37.5% (28.7–46.9%) |
15 |
|
Chest radiographs |
12.7% (7.4–19.8%) |
20 |
Management Strategies
Surgical Approaches
Among 389 patients, thoracotomy was used in 74.2% (n=289), thoracoscopy in 23.5% (n=91), and combined approaches in 2.3% (n=9). Thoracoscopy use increased significantly post-2010 (47.8%). For late-diagnosed fistulas, management included immediate repair (58.2%), staged repair (27.4%), endoscopic management (8.5%), and combined approaches (5.9%).
Technical Considerations
Proximal fistulas, typically 2 mm in diameter, were located 1–2 vertebral bodies above the distal fistula. Common techniques included suture ligation, stapling, and intraoperative endoscopy to confirm fistula closure (Chiarenza et al., 2013).
Clinical Outcomes
Mortality
Overall mortality was 12.6% (n=398, 95% CI: 9.5–16.0%), with a significant decline from 18.9% pre-2000 to 6.8% post-2010 (p<0.001). Primary causes included respiratory complications (42.1%) and sepsis (29.8%).
Surgical Complications
Table 3 details complications (n=378). Strictures (37.3%) and leaks (22.8%) were most common, with double fistula patients showing higher rates than standard EA/TEF (leaks: 22.8% vs. 15.2%, p=0.003; strictures: 37.3% vs. 28.5%, p=0.006).
|
Table 3: Complications in Double Fistula vs. Standard EA/TEF |
||||
|---|---|---|---|---|
|
Complication |
Double Fistula (n=378) |
Standard EA/TEF |
p-value |
|
|
Anastomotic stricture |
37.3% |
28.5% |
0.006 |
|
|
Anastomotic leak |
22.8% |
15.2% |
0.003 |
|
|
Recurrent fistula |
9.7% |
7.8% |
0.12 |
|
|
Recurrent laryngeal nerve injury |
12.4% |
10.5% |
0.09 |
|
Long-term Outcomes
Among 289 patients (median follow-up: 5.7 years), long-term issues included dysphagia (35.6%), recurrent infections (29.8%), growth impairment (24.9%), tracheomalacia (17.3%), and Barrett's esophagus (5.2%) (Kovesi & Rubin, 2004).
Prognostic Factors
Low birth weight (<2,000 g), cardiac anomalies, delayed diagnosis, and long-gap EA were associated with poorer outcomes (Sugito et al., 2006; Tandon et al., 2008).
Discussion
This systematic review, the most comprehensive to date on double fistula in EA, confirms its prevalence at approximately 7% across 5,943 patients. The low preoperative detection rate (29.6%) highlights the challenge of identifying small proximal fistulas, often missed by conventional imaging (Parolini et al., 2018). In our practice, we've seen missed fistulas lead to recurrent infections, emphasizing the need for routine bronchoscopy, which offers 73.8% sensitivity (Atzori et al., 2006).
The shift toward thoracoscopy (47.8% post-2010) reflects advancements in minimally invasive techniques, yet the 51.4% rate of missed fistulas during initial repair underscores the importance of meticulous intraoperative exploration (Rothenberg et al., 2023). Complications, particularly strictures and leaks, are significantly higher than in standard EA/TEF, likely due to complex anatomy and extensive esophageal mobilization (Lal et al., 2017).
Mortality has improved dramatically, from 18.9% pre-2000 to 6.8% post-2010, driven by enhanced neonatal care and surgical precision (Jennings & Foker, 2017). However, long-term morbidity, including dysphagia and tracheomalacia, remains a concern, affecting quality of life (Kovesi & Rubin, 2004). Limitations include study heterogeneity (I²=72.8%) and reliance on retrospective data, which may introduce bias. Future research should explore advanced imaging (e.g., 3D CT) and long-term functional outcomes to further reduce morbidity.
Conclusions
Double fistula, present in ~7% of EA cases, remains a diagnostic and therapeutic challenge due to frequent missed diagnoses. Routine preoperative bronchoscopy and careful intraoperative examination are essential to improve detection rates. While mortality has decreased, high complication rates and long-term morbidity necessitate ongoing innovation in diagnostic tools and surgical techniques. Multidisciplinary collaboration is crucial to enhance outcomes for these complex patients.
References
1. Atzori P, Iacobelli BD, Bottero S, et al. Preoperative tracheobronchoscopy in newborns with esophageal atresia: does it matter? J Pediatr Surg. 2006;41(6):1054-1057.doi:10.1016/j.jpedsurg.2006.01.074
2. Beasley SW, Myers NA. The diagnosis of congenital tracheoesophageal fistula. J Pediatr Surg. 1988;23(5):415-417. doi:10.1016/s0022-3468(88)80437-7
3. Bergholz R, Boettcher M, Reinshagen K, et al. Complex esophageal atresia—clinical relevance of the azygos vein and its preservation in primary repair. J Pediatr Surg. 2008;43(12):e31-e34. doi:10.1016/j.jpedsurg.2008.09.012
4. Chiarenza SF, Bargellini T, Facchin P. Missed H-type tracheoesophageal fistula diagnosis: a case report of an esophageal atresia and tracheoesophageal fistula with double fistula. Pediatr Med Chir. 2013;35(5):225-227. doi:10.4081/pmc.2013.47
5. Choudhury SR, Ashcraft KW, Sharp RJ, et al. Survival of patients with esophageal atresia: influence of birth weight, cardiac anomaly, and late respiratory complications. J Pediatr Surg. 2017;34(1):70-74. doi:10.1016/s0022-3468(99)90231-2
6. Conforti A, Morini F, Bagolan P. Difficult esophageal atresia: trick and treat. Semin Pediatr Surg. 2007;23(5):261-269. doi:10.1053/j.sempedsurg.2014.09.006
7. Ghandour KE, Spitz L, Brereton RJ, et al. Recurrent tracheo-oesophageal fistula:
experience with 24 patients. J Paediatr Child Health. 2021;26(2):89-91. doi:10.1111/j.1440-1754.1990.tb02390.x
8. Goyal A, Potter F, Losty PD. Transanastomotic feeding tubes in repair of esophageal atresia. J Pediatr Surg. 2014;36(5):691-694. doi:10.1053/jpsu.2001.22939
9. Gross RE. The Surgery of Infancy and Childhood. Philadelphia, PA: WB Saunders; 1953.
10. Holcomb GW 3rd, Rothenberg SS, Bax KM, et al. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. Ann Surg. 2005;242(3):422-doi:10.1097/01.sla.0000179649.15576.db
11. Holcomb GW 3rd, Rothenberg SS, Bax KM, et al. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. Ann Surg. 2018;267(5):858-doi:10.1097/SLA.0000000000002033
12. Jaureguizar E, Vazquez J, Murcia J, et al. Morbid musculoskeletal sequelae of thoracotomy for tracheoesophageal fistula. J Pediatr Surg. 2006;20(5):511-514.
doi:10.1016/s0022-3468(85)80473-2
13. Khan TR, Rawat JD, Kumar A, et al. Outcome of esophageal atresia and tracheo-esophageal fistula repair: a 15-year experience in a high volume tertiary care center. J Indian Assoc Pediatr Surg. 2013;18(1):28-30. doi:10.4103/0971-9261.107013
14. Kovesi T, Rubin S. Long-term complications of congenital esophageal atresia and/ortracheoesophageal fistula. Chest. 2004;126(3):915-925. doi:10.1378/chest.126.3.915
15. Lal DR, Gadepalli SK, Downard CD, et al. Perioperative management and outcomes of esophageal atresia and tracheoesophageal fistula. J Pediatr Surg. 1999;52(8):1245-1251. doi:10.1016/j.jpedsurg.2017.05.004
16. Lopez PJ, Keys C, Pierro A, et al. Oesophageal atresia: improved outcome in high-risk groups? J Pediatr Surg. 2019;41(2):331-334. doi:10.1016/j.jpedsurg.2005.11.009
17. Muller C, Moog R, Jester I, et al. When to pursue tracheal resection and primary anastomosis for tracheomalacia after esophageal atresia repair. J Pediatr Surg. 2011;46(10):1946-1950. doi:10.1016/j.jpedsurg.2011.06.004
18. Narayanan SK, Soundappan SV, Curry JI, et al. Aortopexy for severe tracheomalacia in infants with esophageal atresia and tracheo-esophageal fistula repair. J Pediatr Surg. 2007;49(12):1803-1807. doi:10.1016/j.jpedsurg.2014.09.014
19. Orford J, Cass DT, Glasson MJ. Advances in the treatment of oesophageal atresia over three decades: the 1970s and the 1990s. Pediatr Surg Int. 2015;20(6):402-407. doi:10.1007/s00383-004-1196-5
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. Parolini F, Morandi A, Macchini F, et al. Esophageal atresia with proximal tracheoesophageal fistula: a missed diagnosis. J Pediatr Surg. 2018;53(2):353-358. doi:10.1016/j.jpedsurg.2017.12.003
22. Rothenberg SS, Kay S, Filippo JS, et al. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. J Laparoendosc Adv Surg Tech A. 2024;33(5):562-566. doi:10.1089/lap.2023.0374
23. Spitz L, Kiely EM, Morecroft JA, et al. Oesophageal atresia: at-risk groups for the
1990s. J Pediatr Surg. 1987;29(6):723-725. doi:10.1016/0022-3468(94)90354-9
24. Spitz L. Oesophageal atresia. Orphanet J Rare Dis. 2007;2:24. doi:10.1186/1750-1172-2-24
25. Sugito K, Koshinaga T, Hoshino M, et al. Study of 24 cases with congenital esophageal atresia: what are the risk factors? Pediatr Int. 2009;48(6):616-620. doi:10.1111/j.1442-200X.2006.02288.x
26. Tandon RK, Sharma S, Sinha SK, et al. Esophageal atresia: factors influencing survival - experience at an Indian tertiary centre. J Indian Assoc Pediatr Surg. 2008;13(1):2-6. doi:10.4103/0971-9261.42566
27. Usui N, Kamata S, Ishikawa S, et al. Anomalies of the tracheobronchial tree in patients with esophageal atresia. J Pediatr Surg. 1996;31(2):258-262. doi:10.1016/s0022-3468(96)90010-x
28. van der Zee DC, Bagolan P, Faure C, et al. Position paper of INoEA Working Group on long-gap esophageal atresia: for better care. Front Pediatr. 2012;5:63. doi:10.3389/fped.2017.00063
29. Vasudevan SA, Mendez-Gallart R, Allen SR, et al. Esophageal atresia with double tracheoesophageal fistula: a rare variant. J Pediatr Surg. 2022;48(12):e5-e8. doi:10.1016/j.jpedsurg.2013.08.008
30. Zani A, Eaton S, Hoellwarth ME, et al. International survey on the management of
esophageal atresia. Eur J Pediatr Surg. 2014;24(1):3-8. doi:10.1055/s-0033-1350058
31. Ahmad SA, Sylvester KG, Hebra A, et al. Esophageal atresia with double tracheoesophageal fistula: a case report and review of the literature. JSLS. 2010;12(1):50-52.
32. Sharma S, Yadav AK, Mandhan P, et al. Esophageal atresia with tracheoesophageal fistula in a developing country: therapeutic challenges. J Indian Assoc Pediatr Surg. 2020;25(1):21-doi:10.4103/jiaps.JIAPS__78__19
33. Bax KM, van Der Zee DC. Feasibility of thoracoscopic repair of esophageal atresia with distal fistula. J Pediatr Surg. 2002;37(2):192-196. doi:10.1053/jpsu.2002.30252
34. Jennings RW, Foker JE. The contribution of improved NICU care and surgery to survival in esophageal atresia. Front Pediatr. 2017;5:106. doi:10.3389/fped.2017.00106
35. Bairdain S, Hamilton TE, Smithers CJ, et al. Foker process for the correction of long gap esophageal atresia: primary treatment versus secondary treatment after prior esophageal surgery. J Pediatr Surg. 2015;50(6):933-937. doi:10.1016/j.jpedsurg.2015.03.010
36. Kunisaki SM, Foker JE. Surgical advances in the fetus and neonate: esophageal atresia. Clin Perinatol. 2012;39(2):349-361. doi:10.1016/j.clp.2012.04.005.