Rehabilitation of a Young Edentulous Class III Patient with Full-Arch Implant Prosthesis: A Profile Transformation without Orthognathic Surgery
Rehabilitation of a Young Edentulous Class III Patient with Full-Arch Implant Prosthesis: A Profile Transformation without Orthognathic Surgery
Jose Bruno Pannirselvam *
*Correspondence to: Jose Bruno Pannirselvam, Specialist oral and maxillofacial surgeon, Sheikh shakbout medical city, Abudhabi, UAE.
Member ITI Switzerland, Member AO trauma, DCI Member, AOMSI Member.
Orchid ID: 0009-0009-9745-5223
Copyright.
© 2025 Jose Bruno Pannirselvam This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 July 2025
Published: 01 Aug 2025
DOI: https://doi.org/10.5281/zenodo.16793850
Abstract
A 29-year-old female patient with a severe Class III skeletal profile and hypodontia presented with functional difficulties and low self-esteem. Through a multidisciplinary approach involving selective ostectomy and simultaneous implant placement in both arches, the patient was successfully rehabilitated without the need for orthognathic surgery. After 4 months of osseointegration, a permanent implant-supported prosthesis was delivered, achieving both aesthetic and functional transformation. This case highlights the potential of advanced surgical-prosthetic collaboration in resolving complex cases conservatively.
Keywords: Class III profile, edentulous, dental implants, maxillofacial ostectomy, full-arch prosthesis, implant-supported dentures, aesthetic smile rehabilitation, non-orthognathic correction
Rehabilitation of a Young Edentulous Class III Patient with Full-Arch Implant Prosthesis: A Profile Transformation without Orthognathic Surgery
Introduction
Edentulism in young adults is an uncommon but challenging clinical scenario, especially when associated with skeletal deformities such as a Class III skeletal malocclusion and hypodontia. Class III malocclusion is typically characterized by mandibular prognathism and/or maxillary deficiency, leading to poor occlusal relationships, functional impairment, and facial disharmony. In such patients, the psychosocial impact is profound, often resulting in low self-esteem, compromised dietary habits, and diminished overall quality of life.
Conventionally, orthognathic surgery is considered the gold standard for treating severe skeletal discrepancies. Procedures such as Le Fort I osteotomy or bilateral sagittal split osteotomy are used to reposition the jaws and establish favorable occlusion. However, not all patients are suitable candidates for these interventions due to factors like medical comorbidities, psychological hesitation, financial constraints, or personal preference for less invasive options.
In recent years, advancements in digital diagnostics, implantology, and prosthetic planning have made it possible to treat select Class III patients using implant-supported prostheses and strategically planned osteoplasty, thereby avoiding major jaw surgery. Moreover, understanding the patient's concerns and aligning treatment goals with their expectations has become increasingly critical. In this case, special emphasis was placed on accurate diagnosis, personalized planning, and interdisciplinary collaboration involving the oral and maxillofacial surgeon and prosthodontist.
This report presents a 29-year-old edentulous female with a Class III skeletal profile and hypodontia, successfully rehabilitated through a conservative surgical-prosthetic protocol. The treatment involved selective ostectomy and simultaneous implant placement in both jaws, with the implants carefully angled to support emergence in a prosthetic Class I occlusion. The result was a functionally stable, esthetically pleasing, and psychologically transformative outcome—achieved without orthognathic surgery.
Case Presentation
A 29-year-old female patient presented with a severe skeletal Class III profile, hypodontia, and complete edentulism, which caused difficulty in chewing and significantly impacted her self-esteem and facial aesthetics. She initially sought orthognathic surgery to correct her jaw alignment but was referred for a multidisciplinary evaluation to explore less invasive alternatives.
After thorough clinical and radiological assessment, a joint plan was developed by oral and maxillofacial surgeons and prosthodontists. The decision was made to avoid traditional orthognathic surgery and instead proceed with:
- - Selective ostectomy of the maxilla and mandible to optimize ridge form and implant angulation
- - Simultaneous placement of 6 implants in each arch (upper and lower jaws)
- - Immediate provisional prostheses to aid healing and maintain occlusal function
- - Definitive implant-supported full-arch prostheses delivered after 4 months of confirmed osseointegration
This approach allowed for functional rehabilitation and aesthetic facial improvement without the need for jaw repositioning.
Outcome:
- Patient’s skeletal profile improved from Class III to near-Class I
- Restoration of normal diet, speech, and oral function
- Remarkable boost in self-confidence and facial aesthetics
- Long-term, fixed, and stable prosthetic solution with high patient satisfaction
Diagnosis & Treatment Planning
The patient presented with:
- - Complete edentulism in both arches
- - A pronounced skeletal Class III malocclusion with mandibular prognathism
- - Hypodontia and history of early tooth loss
- - A concave facial profile and deficient upper lip support
- - Difficulty in mastication, speech, and low self-esteem
Clinical examination included:
- - Extraoral facial analysis indicating Class III skeletal relationship with midface retrusion
- - Intraoral findings confirming atrophic maxillary and mandibular ridges
- - CBCT imaging used to assess bone height, width, and angulation for implant feasibility
- - Virtual wax-up and digital prosthetic mock-ups prepared to simulate final tooth positioning and occlusal goals
Key considerations included:
- - The need for strategic ridge modification to create a favorable emergence profile for implants
- - Desire to avoid orthognathic surgery due to patient preference for a less invasive approach
- - Restoration of a functional and esthetic Class I occlusion through prosthetic design and implant alignment
Multidisciplinary Planning:
A comprehensive treatment plan was finalized through a joint consultation between the oral and maxillofacial surgeon and the prosthodontist, prioritizing prosthetically driven surgical execution. The final plan included:
- - Selective ostectomy of the maxilla and mandible to optimize ridge contour and implant positioning
- - Simultaneous placement of six implants in each arch, placed with angulation to simulate a Class I occlusion
- - Immediate load temporary prostheses for healing and psychological comfort
- - Definitive screw-retained zirconia prostheses placed four months later following confirmed osseointegration
This approach successfully aligned anatomical correction with the patient’s esthetic and functional demands, enabling Class I occlusion restoration without orthognathic surgery.
Radiographic and Digital Planning
Digital imaging played a central role in guiding the treatment protocol. Cone-Beam Computed Tomography (CBCT) was used to evaluate:
- - Residual ridge volume and bone quality
- - Relationship of anatomical landmarks (maxillary sinus, mandibular canal)
- - Feasibility of parallel implant placement
Digital mock-ups and software-based planning ensured:
- - Correct vertical dimension of occlusion (VDO)
- - Ideal anterior-posterior tooth projection
- - Harmonized smile line and lip support
This digitally guided approach helped predefine implant trajectories and prosthetic contours, minimizing intraoperative variability and supporting predictable esthetic outcomes.
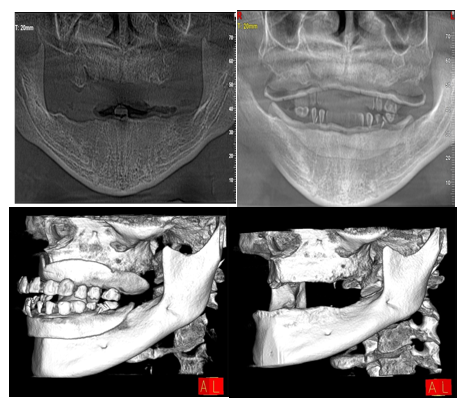
Figure 1: Preoperative treatment plan assessment and simulation xray.
Figure 2: Preoperative Panoramic Radiograph.
Figure 3: Immediate postoperative panoramic radiograph demonstrating successful placement of six maxillary and five mandibular implants following selective ostectomy. Implants are positioned with optimal alignment, ensuring appropriate distribution and support for full-arch prosthetic rehabilitation.
Figure 4: Intraoral view of the final implant-supported prostheses demonstrating excellent esthetic outcome, gingival harmony, and proper occlusal alignment. Prostheses were delivered four months post-implant placement after osseointegration.
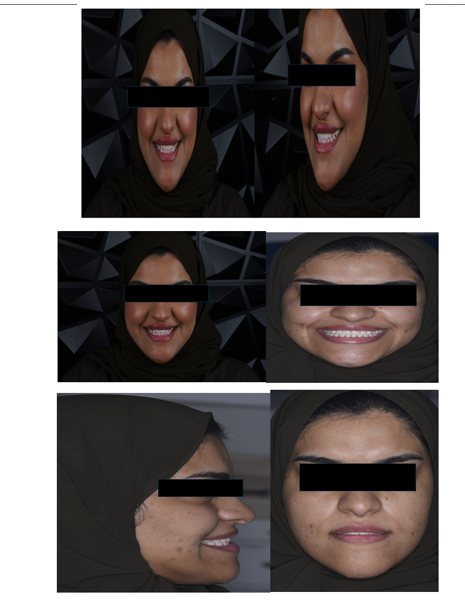
Figure 5: Extraoral frontal view showing the patient's final facial profile and confident smile after full-mouth rehabilitation. Significant aesthetic enhancement was achieved without orthognathic surgery.
Discussion
This case represents a successful, minimally invasive management of a young patient with significant skeletal and dental deficiencies, where traditional orthognathic surgery was avoided. Several critical elements contributed to the success of this case:
1. Patient-Centered Diagnostic Approach
The diagnostic process extended beyond radiographic assessment. Through detailed clinical interviews and psychological evaluation, the patient’s chief concerns—difficulty in eating and embarrassment due to facial appearance—were acknowledged and prioritized. This holistic diagnostic approach helped align the treatment strategy with her personal goals, improving both compliance and satisfaction.
2. Importance of Interdisciplinary Collaboration
The treatment was planned and executed by a highly coordinated team involving the oral and maxillofacial surgeon and the maxillofacial prosthodontist. Importantly, the prosthetic outcome guided the surgical plan, rather than the reverse. This interdisciplinary synergy allowed for accurate placement of implants, optimization of bone volume, and ensured that the prostheses would be esthetically and functionally successful.
3. Selective Ostectomy and Strategic Implant Placement
Selective reduction of both maxillary and mandibular ridges was performed to improve implant angulation and create ideal restorative space. This allowed implants to be positioned with precise emergence profiles and appropriate anteroposterior inclination. By tailoring the bone architecture around prosthetic needs, a near-Class I occlusal relationship was achieved without altering jaw position.
4. Implants in Functional Class I Occlusion
The implants were intentionally placed to support teeth that would restore a Class I occlusal scheme, despite the skeletal base being Class III. This was a critical step in both functional and esthetic rehabilitation, demonstrating how prosthetic foresight can drive surgical execution in advanced implant cases.
5. Immediate Function and Final Restoration
Immediate temporary prostheses were delivered after surgery, providing psychological relief and maintaining vertical dimension. After four months of confirmed osseointegration, full-arch screw-retained zirconia prostheses were placed. These restorations provided excellent esthetics, phonetics, and mastication, with ideal lip support and smile dynamics.
6. Psychological and Quality-of-Life Impact
Beyond the anatomical correction, the most profound transformation occurred in the patient's self-image, dietary habits, and social confidence. Her ability to smile, eat, and speak without hesitation marked a significant psychosocial rehabilitation, highlighting the broader life impact of such treatments.
This case exemplifies the potential of modern implantology and prosthetic planning to transform complex skeletal cases without major surgery. It also underscores the importance of collaboration, patient-specific planning, and restoration-driven surgical execution as pillars of successful full-mouth rehabilitation in skeletal Class III patients.
Conclusion
This case exemplifies how advanced implant-prosthetic rehabilitation combined with targeted surgical intervention can address complex skeletal and dental deficiencies without conventional orthognathic surgery. By leveraging selective ostectomy, strategic implant placement, and precision-guided prosthetics, the patient experienced complete functional and aesthetic recovery.
The transformation from a young, edentulous Class III patient with diminished confidence and chewing ability to an individual with a confident smile and proper diet highlights the life-changing potential of contemporary multidisciplinary dentistry. This approach is especially useful in cases where patients wish to avoid major jaw surgeries, offering a conservative yet effective solution.
References
1. Proffit WR, White RP, Sarver DM. Contemporary Treatment of Dentofacial Deformity. Mosby; 2002.
2. Buser D, Sennerby L, De Bruyn H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol 2000. 2017;73(1):7-21.
3. Jensen OT, Adams MW, Cottam JR, et al. The All-on-4 Shelf: Maxilla. J Oral Maxillofac Surg. 2010;68(10):2520–2527.
4. Misch CE. Contemporary Implant Dentistry. 3rd ed. Mosby Elsevier; 2007.
5. Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 2006;17(Suppl 2):136–159.
6. Papaspyridakos P, Chen CJ, Singh M, Weber HP, Gallucci GO. Success criteria in implant dentistry: A systematic review. J Dent Res. 2012;91(3):242–248.
7. Dawson A, Chen ST. The SAC Classification in Implant Dentistry. Quintessence Publishing Co, Ltd; 2009.