A Case Study on Thoracoscopy
A Case Study on Thoracoscopy
Dr B Anirudh Kumar
1. Dr B Anirudh Kumar MD, Consultant Pulmonologist, Dr A&N Lung Specialty Clinic, Hyderabad, Telangana.
2. Dr Md Iliyas Khan DNB, Interventional Pulmonologist, CARE Hospitals, Banjara Hills, Hyderabad, Telangana.
Correspondence to: Dr B Anirudh Kumar MD, Consultant Pulmonologist, Dr A&N Lung Specialty Clinic, Hyderabad, Telangana.
Copyright
© 2025 Dr B Anirudh Kumar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 Nov 2024
Published: 04 Aug 2025
A Case Study on Thoracoscopy
Case History
58 year old man presented with complaints of SOB, cough and fever since 2 weeks. He reported a gradual onset of Sob which was worsened since past few days. He doesn’t have any other comorbidities. He is a non smoker and occasional alcoholic. He reported that he was losing weight since one month and his appetite has also gone down. On evaluation he has a massive left pleural effusion on Chest Xray. Diagnostic pleural fluid aspiration was done and analysis suggested a exudative fluid with predominant lymphocytes and low ADA. In view of low ADA and exudative fluid we subjected him to thoracoscopy.
Procedure Details
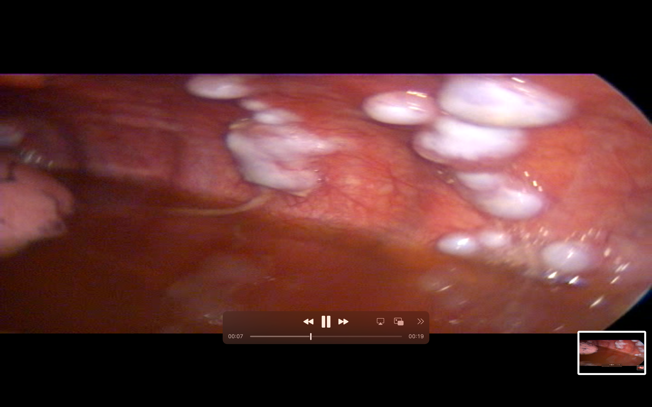
Under short GA, Diagnostic Thoracoscopy was done through left 5th ICS Mid axillary Line. Large white colored multiple pleural nodules were found deposited on the parietal pleura.
Fig 1
Fig 2
Biopsies were taken. ICD was placed and drain was secured.
Final Diagnosis – Metastatic AdenoCarcinoma