The Hidden Face of Beauty: Facial Asymmetry and Left-Side Preference in Art, Anthropology, and Aesthetics.
The Hidden Face of Beauty: Facial Asymmetry and Left-Side Preference in Art, Anthropology, and Aesthetics.
Marc Divaris. *
*Correspondence to: Marc Divaris, France.
Copyright.
© 2025 Marc Divaris., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 Sep 2025
Published: 04 Oct 2025
DOI: https://doi.org/10.5281/zenodo.17301777
Abstract
For centuries, painters and sculptors have instinctively favored the left side of the face, portraying it as softer, fuller, and more expressive. Classical neuropsychological theories attribute this preference to right-hemisphere dominance in emotion processing (2,5,9). However, recent morphometric research shows that in over 80% of cases, the left hemiface is structurally wider, with a slightly more open mandibular angle and a laterally displaced malar projection (12). This finding suggests that left-side preference is rooted in anatomy rather than being solely a perceptual or cultural bias. This article explores the anatomical, sociological, and artistic dimensions of facial asymmetry, tracing its embryologic origins (11), its influence on portraiture from Leonardo da Vinci to Vigée Le Brun (1,4), and its persistence in contemporary photography and facial aesthetics.
The Hidden Face of Beauty: Facial Asymmetry and Left-Side Preference in Art, Anthropology, and Aesthetics.
Introduction
Perfect facial symmetry does not exist. Since the Renaissance, painters have preferentially depicted the left hemiface of their sitters—a phenomenon first highlighted by McManus and Humphrey in the 1970s (1). Several neuropsychological studies attempted to explain this by right-hemisphere dominance for emotion processing and the greater expressiveness of the left hemiface (2,3,5). Tsao and Livingstone (9) described the neural mechanisms underlying face perception, reinforcing the view that this bias might have a neurocognitive origin.
However, these approaches, while insightful, do not fully explain the remarkable historical and cross-cultural consistency of this preference. The purpose of this article is to show that left-side preference also relies on a morphologic reality (11,12) and to explore its artistic, sociological, and clinical implications.
Materials and Methods
A retrospective morphometric analysis was conducted on 615 patients (99 men, 516 women, mean age: 59 years, range: 26–78) who underwent standardized 3D facial imaging between 2003 and 2024. Craniometric landmarks (NASP, malar points, planes P1–P6, Me– Mal angle) were used to measure relative hemifacial width and height. In parallel, 189 human skulls from museum collections (Musée de l’Homme, Paris) were examined to confirm the presence of directional asymmetry in an anthropological sample. Morphometric results were correlated with an iconographic review of historical portraits and masterpieces (Leonardo da Vinci, Vermeer, Vigée Le Brun) to link observed morphology to centuries-old artistic preferences.
Discussion
For centuries, left-side preference in facial representation has been explained through neuropsychology: right-hemisphere dominance for emotional processing, greater expressiveness of the left hemiface, gaze orientation biases, and cultural familiarity effects (2,3,5,8). These approaches—ranging from McManus to Malaspina—objectively documented a robust perceptual phenomenon, and recent studies have shown that this bias may attenuate when viewing “unfamiliar” or other-race faces (7,8). Yet none of these theories fully explain why this preference is so consistent across centuries, cultures, and even in the age of digital photography. What was missing was a solid morphological foundation: a material cause that precedes and partly constrains perceptual interpretation.
Divaris’ recent morphometric research (12) fills this gap. By combining 615 standardized 3D facial scans with craniometric measurements from 189 skulls, he demonstrated that the vast majority of individuals show a directional asymmetry: the left side is structurally wider—with a slightly more open mandibular angle, a more lateralized maxillo-malar block, and a malar point farther from the midline—while the right side is narrower and subtly higher on the vertical axis (Figure 1). In other words, what the eye perceives as “softer, fuller, better lit” on the left is not just a brain trick: it is first an osseous effect. Light reflects more favorably, convex–concave transitions appear smoother, and the whole produces a more “adult” and replete appearance. Conversely, the right side—narrower and higher— reads as the “child” side: slimmer, more elevated, more juvenile.
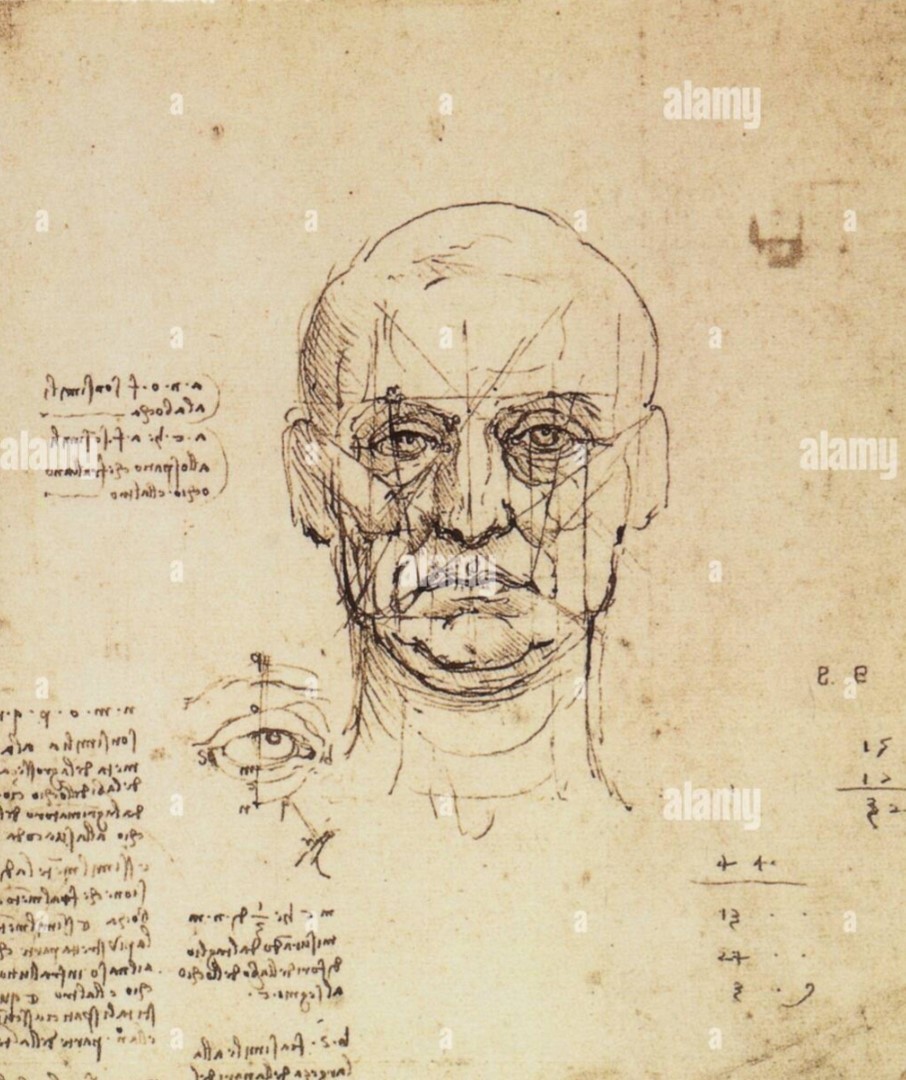
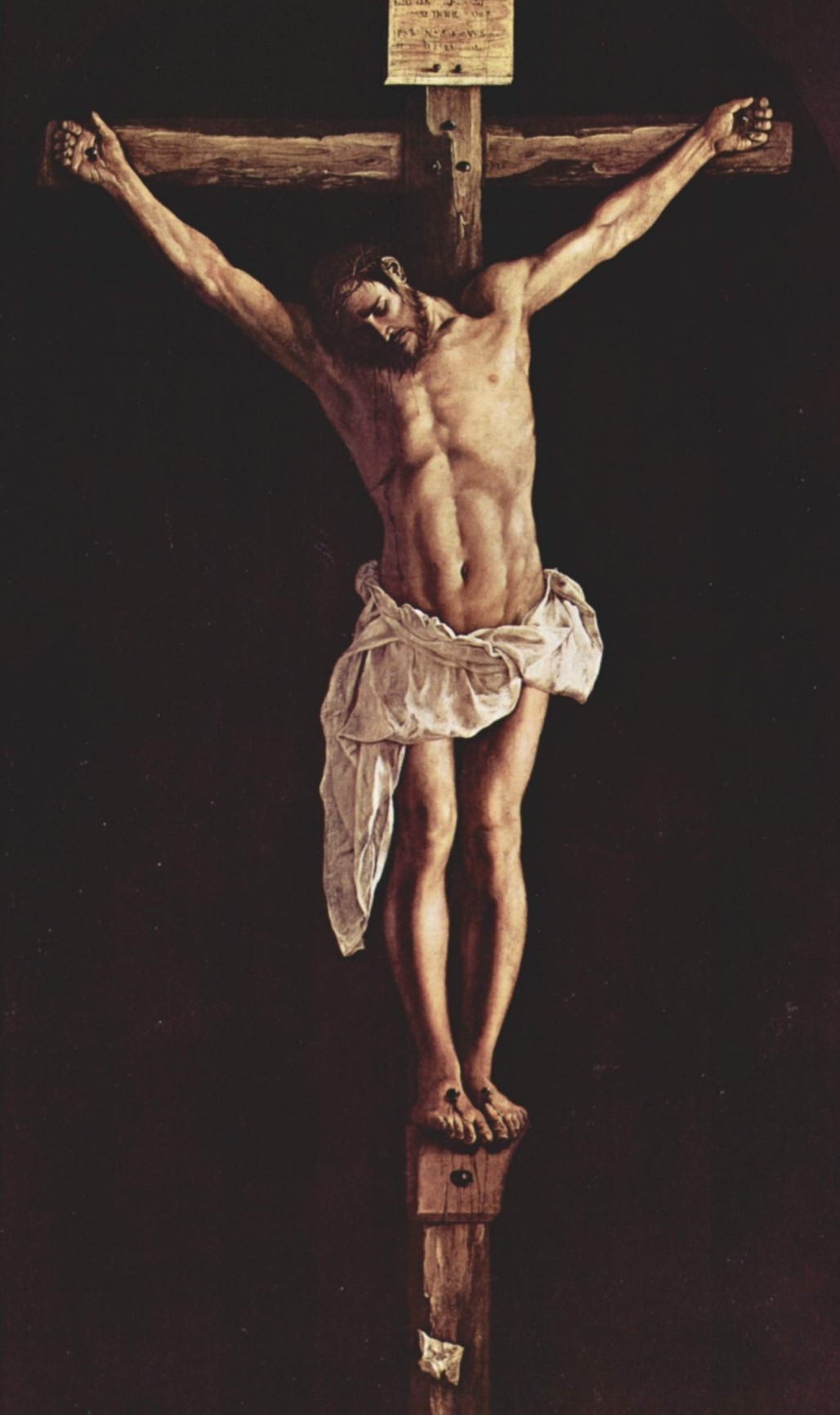
This anatomical foundation retrospectively illuminates the history of portraiture. A meta- analysis published in Nature demonstrated that more than 65% of portraits and busts produced between the 14th and 19th centuries show the sitter’s left hemiface (1). Leonardo da Vinci, obsessed with anatomical truth before becoming a geometer of beauty, painted the Mona Lisa in a left three-quarter view that became the archetype of Western portraiture (Figure 2). In his notebooks, he drew full-face studies where asymmetry is clearly visible— proof that he observed it with precision (Figure 3). Vermeer, in Girl with a Pearl Earring, chose the same orientation, exploiting light on the convex cheek to enhance luminosity and softness (Figure 4). Vigée Le Brun, in her portraits of Marie-Antoinette, consistently chose angles that exploited this fullness, conferring grace and majesty to the queen (Video 1, supplementary material). Even religious iconography reflects this principle: Christ is frequently depicted on the cross with his head tilted to the right, exposing the left hemiface—as if artists sought to reveal the most expressive and most human side of his face (Figure 5).
Figure 1. Composite morphometric schema and averaged facial “robot portrait” — directional asymmetry: wider and more convex left hemiface; narrower, slightly higher right hemiface.
Figure 2. Mona Lisa (La Joconde), Leonardo da Vinci — canonical left three-quarter portrait.
Figure 3. Anatomical sketch, Leonardo da Vinci — full-face study revealing subtle asymmetries between hemifaces.
Figure 4. Girl with a Pearl Earring, Johannes Vermeer — lateral light enhancing the convexity of the left cheek.
Video 1. Rotating bust of Marie-Antoinette (Vigée Le Brun) — dynamic demonstration of left-side fullness (supplementary material).
Figure 5. Depiction of Christ on the Cross — head tilted right, exposing the left hemiface.
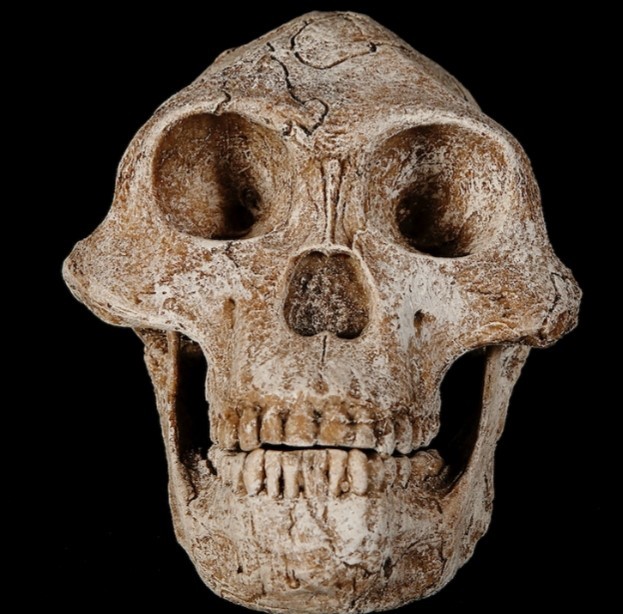
The origin of this asymmetry is embryologic and early. By the fifth gestational week, when nasal and maxillary processes fuse, minute three-dimensional displacements create a cascade of peripheral differences (11). The maxillo-malar block on one side is positioned slightly more antero-laterally, while the contralateral block is closer to the midline and slightly higher. This asymmetry, imprinted early, is amplified by growth mechanics and, later, by gravity’s effect on soft tissues. Aging does not create asymmetry—it reveals the asymmetry already drawn by bone, as can be appreciated on the skull of Lucy (Australopithecus afarensis), evidence that directional asymmetry has been present since early hominins (Figure 6).
Figure 6. Skull of Lucy (Australopithecus afarensis) — directional asymmetry present in early hominins.
This anatomical key also reconciles neuropsychological results with artistic practice. If the left hemiface appears more expressive, it is partly because it offers better visual capture— more favorable receiving surfaces, gradients of light and shadow, and more readable transitions (3,9). The brain prefers what structure makes preferable. Visual field effects, cross-racial familiarity, or recognition strategies in atypical populations modulate the phenomenon (7,8), but they do not originate it. The origin lies in those extra degrees of openness, those few millimeters of malar displacement, those lines of force that, from the orbits to the zygoma to the mandible, create a coherent three-dimensional asymmetry (11,12). This also explains the ambivalence between strict profile and three-quarter view: strict profile magnifies the higher malar point on the narrower side, producing a youthful, elongated effect; three-quarter view displays the fullness of the wider side, making the face appear warmer, more welcoming, more “full of light.”
The aesthetic and clinical implications are direct. The “triangle of youth”—high cheekbones, full midface, and a clean jawline—is not a Platonic ideal to be restored symmetrically; it is a tendency to be restored while respecting constitutive asymmetry. Striving for perfect symmetry erases what makes a face truthful and paradoxically produces artificiality.
Modern surgical approaches—detailed preoperative analysis of skeletal and soft-tissue asymmetry, differential traction vectors, tailored management of superficial and deep compartments—embrace this reality. The result is more natural because it respects the patient’s intimate geometry (12). Where art intuitively chose the angle and side, surgery now personalizes correction: treating the wide side to restore coherence and control excess fullness; treating the narrow side to restore support and continuity of curves, with vertical correction vectors that respect the deep framework.
In sum, the historical preference for the left side is neither an artistic whim nor a mere perceptual myth—it reflects a universal anatomical dissymmetry, imprinted during embryogenesis (11), confirmed by anthropology, and empirically validated by artists (1,4). These data provide the missing link between painterly intuition and measurable reality: they shift aesthetics from a paradigm of imposed symmetry to one of orchestrated asymmetry, where light, guided by bone, naturally finds the path to beauty.
Conclusion
The predominance of the left side in art and visual perception is not a simple cultural convention but the reflection of a fundamental anatomical architecture. By quantifying this reality (11,12), recent work provides an integrative model linking biology, art history, and contemporary aesthetics. Rather than erasing asymmetry, the modern approach should orchestrate and magnify it, restoring the face’s living balance and natural ability to capture light.
References
1. McManus IC, Humphrey NK. Turning the left cheek: The biases of portrait painters. Nature. 1973;243:271–272.
2. Sackeim HA, Gur RC, Saucy MC. Emotions are expressed more intensely on the left side of the face. Science. 1978;202(4366):434–436.
3. Zaidel DW, Fitzgerald P. Sex of viewer and complexity of art influence lateral biases in esthetic preferences for faces and objects. Neuropsychologia. 1994;32(9):893–900.
4. Nicholls MER, Clode D, Wood SJ, Wood AG. Laterality of expression in portraiture: Putting your best cheek forward. Proc R Soc B. 1999;266:1517–1522.
5. Malaspina M, Albonico A, Daini R. Right perceptual bias and self-face recognition in individuals with congenital prosopagnosia. Laterality. 2016;21(2):118–142.
6. Hills PJ, Lewis MB. The development of the left visual field bias for faces during childhood. Laterality. 2011;16(4):354–367.
7. Li C, Wang Z, Bao H, et al. The left-side bias is not unique to own-race face processing. Atten Percept Psychophys. 2021;83:1562–1570.
8. Kang J, Li C, Sommer W, Cao X. The left-side bias is reduced to other-race faces in Caucasian individuals. Front Psychol. 2022;13:855413.
9. Tsao DY, Livingstone MS. Mechanisms of face perception. Annu Rev Neurosci. 2008;31:411–437.
10. Rotshtein P, Henson RN, Treves A, Driver J, Dolan RJ. Morphing Marilyn into Maggie dissociates physical and identity face representations in the brain. Nat Neurosci. 2005;8(1):107–113.
11. Helms JA, Schneider RA. Cranial skeletal biology: Developmental and evolutionary origins of craniofacial asymmetry. Nature. 2003;421:321–328.
12. Divaris M. Decoding Facial Dissymmetry: A Comparative Morphological Study on Human Skulls and Facial Structures. PRS Global Open. 2025;13(2):e5678.