Necrotizing Fasciitis Complicated by Septic Shock: A Case Report from NMC Specialty Hospital, Abu Dhabi
Necrotizing Fasciitis Complicated by Septic Shock: A Case Report from NMC Specialty Hospital, Abu Dhabi
Rahma Abuelgasim Awad Gasim.1*
*Correspondence to: Rahma Abuelgasim Awad Gasim, Ireland.
Copyright
© 2025 Rahma Abuelgasim Awad Gasim. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 July 2025
Published: 03 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17277396
Abstract
Cellulitis is a common bacterial skin infection involving the dermis and subcutaneous tissue, usually caused by bacteria entering through breaks in the skin. It presents with redness, warmth, swelling, pain, and sometimes fever (1). It is frequently associated with diabetes mellitus, peripheral vascular disease, and chronic kidney disease. A 2020 study in BMJ Open reported a significantly higher risk of hospitalization and poor outcomes in cellulitis patients with chronic illnesses (2). A multidisciplinary team approach reduces complications, supports recovery, and lowers recurrence rates.
Necrotizing Fasciitis Complicated by Septic Shock: A Case Report from NMC Specialty Hospital, Abu Dhabi
Case Details
A 63-year-old male, a known case of coronary artery disease, hypertension, left ventricular hypertrophy, hyperlipidemia, obesity, and stage 1 chronic obstructive pulmonary disease (off medication), presented with acute symptoms of pain and ulceration on his lower limbs.
1st Presentation:
He presented with severe pain in the left lower limb, described as 7–8 out of 10, associated with erythematous, tender swelling and purulent discharge. The pain was significant enough to interfere with walking and sleeping. He also reported shortness of breath (SOB) and nausea with vomiting the night before, which resolved spontaneously. He denied chest pain or palpitations.
On examination:
- Temp: 36.6°C
- HR: 78 bpm
- BP: 120/78 mmHg
- RR: 14/min
- Chest auscultation revealed wheezing at the left lung base
Initial investigations showed:
- WBC: 21 x10?/L (elevated)
- CRP: high
- Cardiac troponin: 25/23 ng/L
- Creatinine: 83 mg/L
- High total leukocyte count
The working diagnoses included cellulitis of the left lower limb, acute kidney injury, obstructive sleep apnea with nocturnal SOB, and a possible early sepsis picture. He was also noted to have old rheumatoid arthritis with joint deformities and pre-diabetes.
He was admitted to the ICU, where he was started on IV Tazocin, Clexane, and Enoxaparin for DVT prophylaxis, with pain managed symptomatically. Fall precautions were advised, and ambulation was encouraged.
ICU Course:
On Day 2 in ICU, the patient developed respiratory distress, accompanied by chest pain, nausea, and vomiting. He required oxygen support. Clinical suspicion was raised for pneumonia and sepsis.
Vital changes and findings included:
- SpO?: 90–91% on room air, improved to 96% with 4L O?
- New diagnosis of acute type-1 hypoxic respiratory failure, hyperlactatemia, elevated procalcitonin, high CRP, and ongoing acute kidney injury
- Chest X-ray findings were consistent with pneumonia
- Debridement of the left lower leg were performed regularly, and antibiotic coverage was continued
- Inguinal lymphadenopathy noted
- Potassium and magnesium levels were closely monitored (target K? >4, Mg²? >2)
- GCS monitored regularly per shift
Fig 1: CT abdomen shows dilated small and large bowel loops with proximal ileal wall edema and kinking, likely representing reactive ileus due to bowel wall inflammation, with no evidence of mechanical obstruction
Fig 2: Findings suggest left lower lobe collapse-consolidation with air bronchograms (sparing the superior segment), associated with subsegmental atelectasis in the right basal lung and mild bilateral pleural effusion (left > right).
A multidisciplinary team was involved, including ICU specialists, internal medicine, cardiology, and surgical teams. Close hemodynamic monitoring and laboratory surveillance were continued, and the patient responded gradually to supportive care.
Outcome
The patient showed clinical improvement, with reduction in local limb inflammation and stabilization of systemic markers. Respiratory function improved with oxygen support, and infection parameters gradually trended down.
He was eventually discharged from the ICU, with follow-up arranged through internal medicine and surgical teams for wound care and chronic disease management.
Discussion and Conclusion
Severe lower limb cellulitis with sepsis is a potentially life-threatening condition, particularly in patients with multiple comorbidities such as coronary artery disease, hypertension, obesity, and chronic pulmonary disease, as seen in this case. The patient’s clinical course was complicated by acute type-1 hypoxic respiratory failure, acute kidney injury, and systemic inflammatory response syndrome (SIRS), placing him at high risk for multi-organ dysfunction.
Cellulitis, a common soft tissue infection, typically presents with pain, erythema, swelling, warmth, and tenderness, and may progress to abscess formation or deeper infections such as necrotizing fasciitis if not managed promptly. In this case, the presence of severe pain disproportionate to clinical findings, rapid progression, and systemic toxicity raised clinical suspicion for necrotizing fasciitis, aggressive soft tissue infection characterized by rapid tissue necrosis, systemic toxicity, and high mortality.
Necrotizing fasciitis may be polymicrobial (Type I) or monomicrobial (Type II), with common causative organisms including:
- Group A Streptococcus (Streptococcus pyogenes)
- Staphylococcus aureus (including MRSA)
- Clostridium species
- Gram-negative bacilli such as Escherichia coli and Klebsiella pneumoniae
- Anaerobic organisms
Risk factors include diabetes mellitus, peripheral vascular disease, obesity, immune compromise, and recent trauma or surgery — several of which were present in this patient.
Diagnostic indicators in this case included:
- Elevated white cell count and inflammatory markers (CRP, procalcitonin)
- Pain score of 7–8/10 and inability to ambulate
- Purulent discharge, local swelling, and inguinal lymphadenopathy
- Hypoxia with SpO? of 90–91% on room air
- Evidence of pneumonia and soft tissue involvement on imaging
- Acute kidney injury and elevated creatinine levels
Prompt admission to the ICU and early initiation of broad-spectrum IV antibiotics (Tazocin), along with anticoagulation (Enoxaparin) for DVT prophylaxis and surgical debridement, were crucial. Respiratory support, electrolyte management, and close monitoring of renal function and neurologic status (GCS) were also provided. The coordinated effort of a multidisciplinary team including intensivists, surgeons, internists, and cardiologists enabled comprehensive care.
Prognosis in necrotizing fasciitis or advanced cellulitis with sepsis is closely tied to the timing of diagnosis, surgical intervention, and adequacy of antimicrobial coverage. In this case, early recognition and aggressive treatment led to clinical stabilization and gradual recovery.
Delayed diagnosis in similar presentations may result in:
- Septic shock
- Disseminated intravascular coagulation (DIC)
- Acute respiratory distress syndrome (ARDS)
- Extensive tissue necrosis requiring amputation
- Multi-organ failure or death
This case highlights the importance of maintaining a high index of suspicion for necrotizing fasciitis in elderly, comorbid patients presenting with rapidly progressive cellulitis. Early ICU admission, appropriate antibiotic coverage, timely surgical intervention, and coordinated multidisciplinary management are key to improving outcomes.
References
1. Mayo Clinic Staff. Cellulitis – Symptoms and causes [Internet]. Rochester (MN): Mayo Foundation for Medical Education and Research; 2023 [cited 2025 Aug 12]. Available from: https://www.mayoclinic.org/diseases-conditions/cellulitis/symptoms-causes/syc-20370762
(2)-Thomas KS, Crook AM, Nunn AJ, Foster KA, Mason JM, Chalmers JR, et al. Risk factors, clinical features, and outcome of cellulitis: a population-based study. BMJ Open. 2020;10(1):e034028. doi:10.1136/bmjopen-2019-034028.
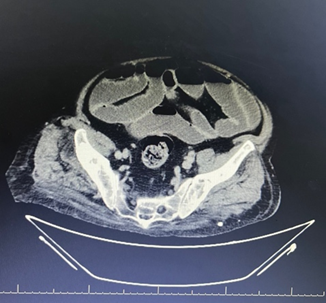
Figure 1
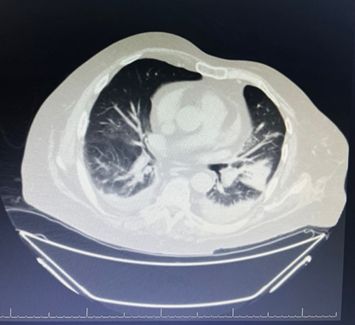
Figure 2