Infantile Small Bowel Obstruction due to Congenital Adhesion Bands: A Case Report
Infantile Small Bowel Obstruction due to Congenital Adhesion Bands: A Case Report
S Adefarakan1*, W Miranda2, A Fredua-Agyeman3, W Asman4, S Osei-Nketiah5
1. Department of Paediatric Surgery, University of Ghana Medical Centre (UGMC), Accra, Ghana
Department of Paediatrics, 37 Military Hospital.
*Correspondence to: Shina Adefarakan, Department of Paediatric Surgery, University of Ghana Medical Centre (UGMC), Accra, Ghana.
Copyright
© 2025: Shina Adefarakan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 Sep 2025
Published: 01 Oct 2025
Abstract
Congenital adhesion bands is a rare cause of intestinal obstruction. We report a case of a 6 week old boy who presented with signs and symptoms of intestinal obstruction. The child presented with irritability, bilous vomiting and abdominal distension. There was no history of previous surgery. Exploratory laparotomy was done and patient recovery was uneventful after the procedure. It is important to keep in mind congenital bands as a differential diagnosis of intestinal obstruction in paediatric patients.
Infantile Small Bowel Obstruction due to Congenital Adhesion Bands: A Case Report
Case Presentation
A 6 week old male was presented to hospital with a history of irritability and non-bilous vomiting for 3 days. On the 4th day, the vomiting became bilous with abdominal distension. Mother also noticed small amounts of blood in his stools. He was born by caesarian section at term on account of multiple uterine fibroids and elderly primigravida mother. His birth weight was 3.1kg. Child was fed breast milk from birth up until his presentation. On physical examination, child looked ill and was dehydrated evidenced by dried mucosa and sunken eyes. His vital signs were heart rate 140 beats per minute, respiratory rate 46 cycles per minute, temperature 37.3 degrees and oxygen saturation of 99% on room air. On abdominal examination, the patient had a grossly distended abdomen, hypertympanitic on percussion with no signs of peritoneal tenderness. On rectal examination child had mucous stools with streaks of blood in diaper. No palpable mass was found in rectum. Nasogastric tube contained bilous content which was draining copiously. Laboratory investigations showed Hb 10.4g/dL, white cell count 10.50x103, platelets 516. Blood urea and creatinine results were normal. Abdominal X-ray showed multiple dilated loops of bowel (Fig. 1). Ultrasound showed multiple distended non peristalsing loops of bowel with no target sign suggestive of intussusception. Patient was resuscitated and was taken for exploratory laparotomy which showed fibrous adhesion band in the terminal ileum about 25cm from the ileocaecal valve causing partial bowel obstruction. There was no sign of ischaemia. The portion of ileum was resected about 1cm on both ends and primary anastomosis done. Patient recovered well, tolerated full feeds and was discharged home on postoperative day five.
Fig. 1 : Plain abdominal radiograph showing dilated loops of bowel.
Figure 2 : Arrow showing congenital adhesion band
Discussion
Anomalous congenital bands were first described by Touloukian in 1979 [1]. There are four types of the congenital peritoneal band according to Wayne and Burrington [2,3]:
Intestinal bands and adhesions are usually caused from inflammatory processes and in patients exposed to previous surgery. In congenital bands, there is no association with previous laparotomy or peritonitis. These bands are thought to be congenital in nature. Most congenital bands occur in the small intestine, and very rarely seen in the large intestine [4,5 ].
Although not fully understood, the etiology is said to have no identifiable embryonic cause. Reports have shown that these anomalous congenital bands are commoner in males with a mean of 2 year s[6]
Clinical presentation of congenital bands vary according to patients with the common symptoms being vomiting, abdominal pain, abdominal distension and constipation. Intraabdominal hemorrhage has also been reported as our patient in this case report presented similarly[7].
A plain abdominal x-ray is useful to confirm the diagnosis of intestinal obstruction it must be emphazised that the diagnosis of anomalous congenital bands is difficult to make preoperatively.
Management of these patients is usually surgical either by laparotomy or laparoscopy to prevent the risk of bowel ischaemia and perforation. Kwang et al reported that laparotomy band excision is needed in 3 out of 10 patients, and 7 patient was laparotomy segmental resection [8]. The options of resection of the adhesion band alone, resection and anastomosis, diverting ileostomy have all been reported with the choice of procedure depending on the clinical stability of the child as well as the extent of obstruction caused by the anomalous congenital band.
Conclusion
Although a rare condition, the presence of anomalous congenital band should be always be kept in mind in a paediatric patient presenting with intestinal obstruction with no prior surgical procedure.
Proper history and investigations should be done and surgical treatment should be offered as quickly as possible to prevent ischaemia and reduce morbidity and mortality from this condition.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient’s mother has given her consent for the patient’s images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
None
Conflicts of interest
There are no conflicts of interest
References
1. B. Erginel, F.G. Soysal, H. Ozbey, et al. Small bowel obstruction due to anomalous congenital bands in children. Gastroenterol Res Pract, 2016 (2016), pp. 6-8
2. S.J. Crankson, K.A. Al-Mane, A. Al-Zaben, et al. Extrinsic duodenal obstruction from anomalous congenital band. Ann Saudi Med, 20 (2000), pp. 443-444
3. E.R. Wayne, J.D. Burrington. Extrinsic duodenal obstruction in children Surg Gynecol Obstet, 136 (1973), pp. 87-93
4. A.C. Fang, J. Carnell, J.C. Stein. Constipation in a 7-year-old boy: Congenital band causing a strangulated small bowel and pulseless electrical activity. J Emerg Med, 42 (2012), pp. 283-287
5. B. Jonatan, N. Mariana, F. Nurmantu , M. Faruk. Small bowel obstruction due to anomalous congenital bands in children: A case report and literature review. Journal of Pediatric Surgery Case Reports. Volume 54. March 2020, 101383
6. B. Etensel, S. Ozkisacik, F. Döger, M. Yacizi, H. Gürsoy. Anomalous congenital band: a rare cause of intestinal obstruction and failure to thrive. Pediatr Surg Int, 21 (2005), pp. 1018-1020
7. K. Tsukuda, K. Watanabe, S. Nakahara, et al. A case of a pediatric intraabdominal hemorrhage caused by anomalous congenital band. Jpn J Gastroenterol Surg, 42 (2009), pp. 1626-1630
8. K.H. Yang, T.B. Lee, S.H. Lee, et al. Congenital adhesion band causing small bowel obstruction: what's the difference in various age groups, pediatric and adult patients. BMC Surg, 16 (2016), pp. 1-6.
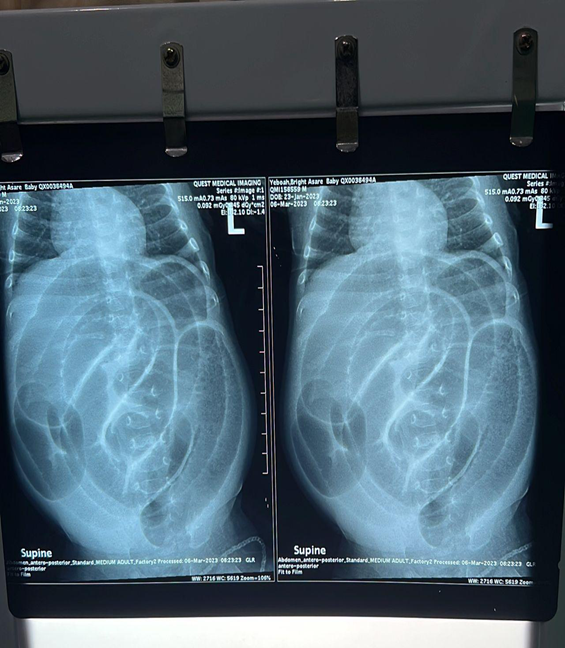
Figure 1
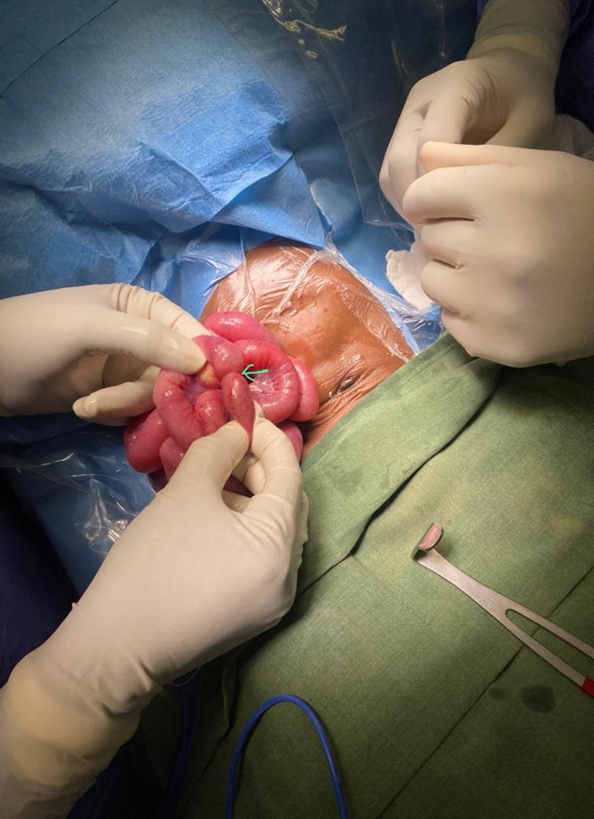
Figure 2