A Rare Type of Postoperative Intussusception : Ileoileal Intussusception After Ileocolic Intussusception in a 10 Month Old
A Rare Type of Postoperative Intussusception : Ileoileal Intussusception After Ileocolic Intussusception in a 10 Month Old
S Adefarakan1*, S Abdullai2, C Akwei3, W Asman4, S Osei-Nketiah5
1. Department of Paediatric Surgery, University of Ghana Medical Centre (UGMC), Accra, Ghana
Department of Paediatrics, 37 Military Hospital.
*Correspondence to: Shina Adefarakan, Department of Paediatric Surgery, University of Ghana Medical Centre (UGMC), Accra, Ghana.
Copyright
© 2025: Shina Adefarakan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 Sep 2025
Published: 01 Oct 2025
Abstract
Postoperative Intussusception has been described in literature after surgical procedures such as Nephectomy for Wilm’s tumor and Ladd’s procedure for Malrotation [1] However, the finding of postoperative ileoileal intussusception after manual reduction of ileocolic intussusception is a very rare occurrence. Very few reports have been found in literature. In this case report, we describe the clinical management of a 10 month old female who presented with ileoileal intussusception within 1 week of laparotomy for a previous manual reduction of ileocolic intussusception
A Rare Type of Postoperative Intussusception : Ileoileal Intussusception After Ileocolic Intussusception in a 10 Month Old
Introduction
Intussusception is the most frequent cause of bowel obstruction in infants and toddlers. It is an acquired invagination of a segment of bowel (intussusceptum) into an adjoining segment (intussuscipiens). The classic presentation is an infant or a young child with intermittent, cramping abdominal pain associated with “currant jelly” stools and a palpable mass on physical examination, although this triad is seen in less than a fourth of children[1].
Management of intussusception is usually by radiologic reduction (Hydrostatic or Pneumatic reduction) or by surgical intervention. However there are a number of situations in which any attempt at radiologic reduction should be bypassed and surgical intervention provided as primary therapy[2].
The entity of postoperative intussusception is quite unique and rare to the paediatric population and should be considered in the differential diagnoses of early postoperative bowel obstruction. The intussusception is typically in the small bowel but does not have a lead point. It can occur after any retroperitoneal, abdominal, or extra-abdominal procedure[2].
Case Report
A 10 month old female presented to hospital with a 4 day history of bilious vomiting, mild abdominal distension and passage of bloody mucoid stools. She had had an antecedent episode of flu about 3 weeks prior to presentation. On examination, she appeared ill, dehydrated but not in obvious respiratory distress. On abdominal examination, her abdomen was mildly distended and a mass was palpable in the abdomen. On digital rectal examination, bloody mucoid stools was seen on the examining finger. Ultrasound was done which showed the presence of a target sign hereby confirming the diagnosis of intussusception. Her laboratory investigations were done. Her haemoglobin level was 9.8g/dL and other parameters were normal. Her Blood urea and creatinine levels were also normal. IV fluid resuscitation and antibiotics were started and she was taken to theatre for laparotomy.
On laparotomy, there was an ileocolic intussusception. The bowel appeared dusky but was still viable. The bowel was manually reduced successfully and the abdomen was closed. Child recovered and was discharged home on post operative day 3.
On post operative day 4, the mother complained that the child had been vomiting. Vomiting was however non-bilous. She was counselled to observe the vomiting and report back to hospital if it persisted. On post operative day 5, mother complained that the child had been irritable, crying a lot and had 3 episodes of non-bilious vomiting.
On post operative day 6, mother represented the hospital with complaints of persistent non-bilous vomiting more than 5 times during the day, irritability and abdominal distension. The child was then re-admitted. Laboratory investigations done showed an Hb of 10.5, normal white cell count, neutrophils and platelets. The Blood urea and creatine showed hyponatraemia of 128mmol/L. However the other parameters were normal. An abdominal X-ray was also done; and it showed signs of small bowel obstruction. The child was immediately resuscitated, a nasogastric tube was passed which drained bilious aspirates and she was taken in for a relook laparotomy. On laparotomy, an ileo-ileal intussusception was found. The bowel was viable and was again manually reduced successfully and abdomen closed. The patient did well post operatively and was subsequently discharged on post operative day 4. She was seen on clinic review and is currently in good health.
Figure 1 : Abdominal distension after 1st laparotomy
Figure 2 : showing ileoileal intussusception on laparotomy
Figure 3: X- ray showing intestinal obstruction
Discussion
Postoperative intussusception is indeed a rare clinical entity. It requires a high index of suspicion to make the diagnosis of this condition. Postoperative intussusception has been described after ileocolic intussusception reduction and resection, retroperitoneal dissections, long intra-abdominal procedures, a Ladd procedure, nephrectomy for wilm’stumor or extra-abdominal operations.[3,4]
Post operative Intussusception accounts for 3–10% of cases of postoperative bowel obstruction and most often occurs in the initial 10 days following a procedure [5,6]
In one report of postoperative ileoileal intussusception after manual reduction of ileocolic intussusception, Celiac disease (CD) was found to be the underlying cause. It was therefore proposed that celiac disease may be responsible for these special types of intussusceptions that may be considered idiopathic, and further investigations, such as endoscopy, should be considered in such children [7].
Another report which seems to have the highest number of postoperative ileocolic intussusception after operative reduction of ileocolic intussusception over a 12 year period showed that all 6 cases of postoperative ileoileal intussusception after surgery for ileocolic intussusception occurred within 1 week after the initial operation. The clinical manifestation was small intestinal obstruction without abdominal palpable mass or bloody stool. Abdominal ultrasound examination revealed the target sign in 5 cases [8].
Ileus and adhesive obstruction are more frequently encountered as a cause for intestinal obstruction in the postoperative patient. Thus, an index of suspicion is needed, and ultrasound is a useful diagnostic tool in diagnosing postoperative intussusception particularly because the clinical symptoms of postoperative ileoileal intussusception after operations for ileocolic intussusception are not typical [8]
Conclusion
The presentation of patients with postoperative ileoileal intussusception after manual reduction of ileocolic intussusception can usually be misleading. The clinical presentation occurring within a week after the initial operation and the manifestation of small intestinal obstruction occurring without bilious vomiting, palpable abdominal mass or bloody mucoid stools should raise suspicion. A second post operative (ileoileal) intussusception should always be kept in mind in this kind of presentation after previous surgical reduction and surgical management should be offered immediately.
Consent
Informed consent was sought from the mother of the child
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
1. Holcomb G III, Murphy J, St. Peter S. Holcomb and AshcraftPaediatricSurgery , Seventh Edition. Intussusception.Chapter 38, 621-627
2. Emil S. Clinical Paediatric Surgery -A case based interactive approach.Chapter 31 Intussusception 304-313
3. Holcomb III GW, Ross III AJ, O’Neill Jr JA. Post-operative intussusception: increasing frequency or increasing awareness? South Med J. 1991;84:1334–1339.
4. Bai YZ, Chen H, Wang WL. A special type of postoperative intussusception: ileoileal intussusception after surgical reduction of ileocolic intussusception in infants and children. J Pediatr Surg. 2009;44:755– 758.
5. Linke F, Eble F, Berger S. Postoperative intussusception in childhood. PediatrSurg Int. 1998;14:175–177.
6. Laje P, Stanley CA, Adzick NS. Intussusception after pancreatic surgery in children: a case series. J Pediatr Surg. 2010;45:1496–149
7. GawriehB, Salhab N, Omran A , Alshehabi Z, Taishori N, AliW .Celiac disease: a rare cause of 'postoperative' ileoileal intussusception after surgical reduction of ileocolic intussusception in a toddler.
J Surg Case Rep. 2020 Jun 1;2020(5):rjaa073. doi: 10.1093/jscr/rjaa073.
8. Bai YZ, Chen H, Wang WL. A special type of postoperative intussusception: ileoileal intussusception after surgical reduction of ileocolic intussusception in infants and children. J Pediatr Surg. 2009 Apr;44(4):755-8 doi: 10.1016/j.jpedsurg.2008.08.011.

Figure 1

Figure 2
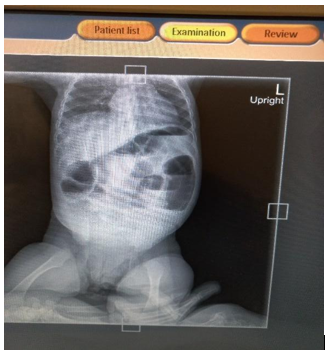
Figure 3