A Rare-Case: Association of Rapid height gain in an 11 years old child treated with Growth hormone complicated by Superior Mesenteric Artery Syndrome
A Rare-Case: Association of Rapid height gain in an 11 years old child treated with Growth hormone complicated by Superior Mesenteric Artery Syndrome
Aida Al Jabri1*, Muhammed Ibrahim2, Rawan Sakir2, Ahmed Amodi3, Mohammed M. Alqahtani4, Ahmed M. Almuslim5
1. Pediatric Endocrinologist, Al Moosa Specialist Hospital, Ahsaa, Saudi Arabia.
2. Pediatric department, Al Moosa Specialist Hospital, Ahsaa, Saudi Arabia.
3. Pediatric Endocrinologist, Al Moosa Specialist Hospital, Ahsaa, Saudi Arabia.
4. Pediatric Endocrinologist, King Khalid University, Abha, Saudi Arabia.
5. Pediatric Radiologist, Al Moosa Specialist Hospital, Ahsaa, Saudi Arabia.
*Correspondence to: Aida Al Jabri, Pediatric Endocrinologist, Al Moosa Specialist Hospital, Ahsaa, Saudi Arabia.
Copyright
© 2025 Aida Al Jabri, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 Sep 2025
Published: 07 Oct 2025
ABSTRACT:
An uncommon cause of proximal intestinal blockage is superior mesenteric artery syndrome (SMA). Numerous other names for it have been proposed, such as arteriomesenteric duodenal blockage, Wilkie syndrome, Cast syndrome, and chronic duodenal ileus. The loss of the intervening mesenteric fat pad is the primary cause of the condition, which is characterized by compression of the third section of the duodenum as a result of narrowing of the space between the superior mesenteric artery and aorta. Research suggests that experiencing a growth spurt increases the likelihood of developing SMA syndrome, and each incident that worsens the aortomesenteric space constriction increases the likelihood of a SMA syndrome manifestation.
In this case, an 11-year-old known to have short stature who was receiving growth hormone therapy had linear growth without gaining weight and was ultimately diagnosed with SMA syndrome, a rare correlation between the two conditions. Rapid growth spurt is a risk factor for superior mesenteric artery (SMA) syndrome, but in pediatric population, the syndrome does not always emerge as a result of weight loss.
History of recurrent abdominal pain and spontaneous resolution of the symptoms, draws attention to the fact that SMA syndrome with such presentation may be missed or misdiagnosed as functional disorders. These imply that SMA syndrome may be responsible for some of the unexplained abdominal symptoms among the pubertal group. Therefore, SMA syndrome should be considered in adolescents with recurrent abdominal symptoms.
Keywords: short stature; growth hormone; superior mesenteric artery syndrome; case report.
A Rare-Case: Association of Rapid height gain in an 11 years old child treated with Growth hormone complicated by Superior Mesenteric Artery Syndrome
Introduction
The narrow angle between the SMA and the Aorta compresses the third part of the duodenum in superior mesenteric artery (SMA) syndrome, which is believed to be an uncommon condition. (1) The following categories describe the typical causes of acute angulation between the SMA and the aorta: (1) marked weight loss resulting in the loss or depletion of retroperitoneal fatty tissues;
(2) external compression using belts or Spica casts; and (3) anatomical defects and congenital anomalies, such as intestinal malrotation, a high insertion of the duodenum at the ligament of Treitz, and corrective spinal surgery for scoliosis.
Postprandial epigastric discomfort, bilious vomiting, nausea, and early satiety are the symptoms. (3) Patients with SMA syndrome typically show up following spinal surgery or abrupt weight loss. (4) As a result, in young people without traditional risk factors including substantial weight loss, psychological issues, or spinal surgery, SMA syndrome is typically unexpected.
Case Illustration
Clinical Presentation
A 11 years old male patient, diagnosed at our hospital with a growth hormone deficiency and severe short stature. He had been receiving growth hormone (GH) replacement therapy for over a year. After a year from starting GH treatment, he was complaining of persistent vomiting after every oral intake and abdominal pain when he was first seen. For a month, there was intermittent pain in the umbilical region that was exacerbated by food intake and subsided by fasting or vomiting. There was no past history of eating from outside, abdominal trauma, or interaction with sick individuals. Neither constipation nor diarrhea. He has never shown up with these symptoms before. No history of previous admissions. He was taking growth hormone till two months back, and during that time, his height climbed by more than 15 cm (from 122 to 137 cm) over 16 months. His weight remained constant at 29 kg, and his BMI was 15.5 kg/m2, which is below average.
There was no noteworthy family history of gastrointestinal disorders. Upon evaluation, he has bradycardia with heart rate down to 47 beats per mint, but he was not in distress, and his oxygen saturation and respiratory rate were both maintained on room air. The patient's underweight of 29 kg at the fifth percentile was a clear sign of failure to thrive. The abdomen was soft and lax with no organomegaly, the capillary refill time and peripheral pulsation were within normal limits, and the results of the other systemic exams were ordinary.
Investigations & Diagnostic workup
Urine analysis, liver function, electrolytes, CBC, CRP, and other basic lab tests were performed. All of the results were within normal limits. Multiple reactive mesenteric lymph nodes with preserved echogenic hilum were shown on an abdominal ultrasonography. CT scan was done which showed reduced aortomesenteric angle and aortomesenteric distance measured 20 degree and 6 mm respectively with relatively distended stomach and first 2 parts of duodenum. Impression was superior mesenteric artery syndrome.
|
WBC |
6.8 (10*3 u/L) |
|
HB |
12.1 (g/dl) |
|
Platelet |
317 (10*3 u/L) |
|
CRP |
<1 (mg/dl) |
|
Na |
135 (mmol/l) |
|
K |
4.3 (mmol/l) |
|
Ca |
2.24 (mmol/l) |
|
Urea |
3.2 (mmol/l) |
|
Creatinine |
47 (umol/l) |
|
AST |
18 (U/l) |
|
ALT |
8 (U/l) |
|
Amylase |
92 (U/l) |
|
Lipase |
19 (U/l) |
Fig 1: Axial image of IV contrast enhanced CT scan of the abdomen demonstrates gastric dilatation.
Fig 2 :Axial image of IV contrast enhanced CT scan of the abdomen demonstrates aortomesenteric narrowing (4 mm) (Normal range > 10 mm).
Fig 3: Axial image of IV contrast enhanced CT scan of the abdomen demonstrates duodenal dilatation with transitional zone at the aortomesenteric window.
Fig 4: Sagittal image of IV contrast enhanced CT scan of the abdomen demonstrates aortomesenteric sharp angle ( 9°) (Normal range > 22°).
The tight and sharp aortomesenteric distance and angle respectively along with the gastric and duodenal dilatation are in favour of superior mesenteric artery syndrome.
Therapeutic Interventions
The patient condition necessitated a multidisciplinary approach, involving several sub- specialties. Pediatrics surgery team suggested no intervention from their side; in the meantime, gastrointestinal team recommended to do endoscopy with biopsy, to start high caloric formula through naso-jejunal NJ tube for feeding along with TPN. Pediatric intensive care unit inserted the PICC line and started the TPN. Endoscopy revealed esophagus with mild erythema, no hiatal hernia in fundus, moderate erythema in gastric body, erythema and nodularity in antrum, biopsies were taken and NJ tube was inserted. Furthermore, urea breath test done and was positive, indicating positive H-pylori pathogen so started triple regiment on amoxicillin, metronidazole, and omeprazole. Celiac profile was negative. Biopsy results was suggestive for H pillory, chronic duodenitis and chronic active follicular gastritis. Next day patient not tolerating the Naso jejunal tube as he developed episodes of vomiting, so tube removed. He gradually tolerated oral feeds and kept on TPN for a total of 3 weeks. Eventually he reached his targeted weight i.e. 35 kg so discharged home with close follow up. Growth hormone was resumed with caution.
Discussion
In early puberty, boys experience a significant increase in lean body mass and a concomitant loss of adipose tissues. These pubertal changes in body composition often lead to a narrowing of the aortomesenteric space due to a depletion of the mesenteric fat pad. Therefore, as previous studies indicate, a growth spurt is a risk factor for SMA syndrome, and any event that further exacerbates the narrowing of the aortomesenteric space is likely to result in a manifestation of SMA syndrome. Potential triggers identified thus far for such exacerbation include extra weight loss due to infection and overeating after dieting. In the present case, considering his linear growth without weight gain, the patient’s mesenteric fat tissue had already been depleted. The abdominal CT also revealed the significant decrease in his adipose tissue. Therefore, the retarded passage of the ingested food at the duodenum and the acute consumption of a large volume of water caused a transient obstruction that spontaneously resolved with postural changes.
This case supports the previous findings that weight loss is not necessary for the development of SMA syndrome in the pediatric population. For example, Biank and Werlin(3) reported no weight loss was observed in 50% of the 22 pediatric cases of SMA syndrome. The reason for the development of SMA syndrome in children without weight loss is currently unexplained. However, the present case speculates that insufficient weight gain relative to height growth causes a decrease in visceral fat and predisposes children to SMA syndrome.
SMA syndrome can be managed initially with conservative therapy such as gastric decompression, electrolyte correction, and nutritional support which is an important component of conservative treatment. Psychiatric assessment is necessary for those with eating disorders. When oral feeding is not tolerated, enteral feeding can be performed through a naso-jejunal tube placed distal to the obstruction.
Parenteral nutrition may be required in order to provide sufficient nutrition. Pediatric patients with acute presentation are likely to benefit from conservative management alone. However, if conservative management fails, surgical options, including Strong’s procedure, gastrojejunostomy and duodenojejunostomy, are indicated.
A pediatric patient presenting with bilious vomiting should be presumed to have an intestinal obstruction that is a surgical emergency. An upper gastrointestinal series should be performed when intestinal malrotation is suspected. In the present case, the patient have been kept hospitalized until malrotation was ruled out and the underlying causes were identified.
Recurrent abdominal pain that resolves spontaneously within several hours, as observed in this patient, is frequently encountered in pediatric emergency care. Our case provides insight into the clinical observation. As stated above, a growth spurt is a predisposing condition for SMA syndrome, and acute consumption of food and water, which is often observed among adolescents, is identified as a trigger for the manifestation of the syndrome. These suggest that SMA syndrome might occur more frequently in such population than previously thought. In addition, the present case describes a case of SMA syndrome with a history of recurrent abdominal pain and spontaneous resolution of the symptoms, and draws attention to the fact that SMA syndrome with such presentation may be missed or misdiagnosed as functional disorders. These imply that SMA syndrome may be responsible for some of the unexplained abdominal symptoms among the pubertal group. Therefore, SMA syndrome should be considered in adolescents with recurrent abdominal symptoms.
Conclusion
- Rapid growth spurt is a risk factor for superior mesenteric artery (SMA) syndrome, and weight loss is not necessary for the development of the syndrome in the pediatric population.
- Acute and excessive ingestion of water and food can trigger a manifestation of SMA syndrome in adolescents whose visceral adipose tissue has already been depleted.
- A pediatric patient presenting with persistent abdominal pain and vomiting should be presumed to have an intestinal obstruction.
- Patients should not be sent home without ruling out surgical emergencies.
- It is important to consider SMA syndrome in the differential diagnosis of adolescents with recurrent abdominal symptoms.
Institutional Review Board Statement: Ethical review and approval were waived for this study as per the requirements of the Institutional Review Board (IRB) of Al Moosa Research Center.
Informed Consent Statement: Signed informed consent for participation and the publication of medical details was obtained from the parents of this child.
Data Availability Statement: Not Applicable.
Conflicts of Interest: The authors declare no conflict of interest.
References
1) Salehzadeh, F., Samadi, A., & Mirzarahimi, M. (2019). Superior Mesenteric Artery Syndrome in a 6-Year-Old Girl with Final Diagnosis of Celiac Disease. Case reports in gastrointestinal medicine, 2019, 3458601. https://doi.org/10.1155/2019/3458601
2) Mosalli, R., El-Bizre, B., Farooqui, M., & Paes, B. (2011). Superior mesenteric artery syndrome: a rare cause of complete intestinal obstruction in neonates. Journal of pediatric surgery, 46(12), e29–e31. https://doi.org/10.1016/j.jpedsurg.2011.08.021
3) Biank, V., & Werlin, S. (2006). Superior mesenteric artery syndrome in children: a 20- year experience. Journal of pediatric gastroenterology and nutrition, 42(5), 522–525. https://doi.org/10.1097/01.mpg.0000221888.36501.f2
4) Okamoto, T., Sato, T., & Sasaki, Y. (2019). Superior mesenteric artery syndrome in a healthy active adolescent. BMJ case reports, 12(8), e228758. https://doi.org/10.1136/bcr- 2018-228758
5) Welsch, T., Büchler, M. W., & Kienle, P. (2007). Recalling superior mesenteric artery syndrome. Digestive surgery, 24(3), 149–156. https://doi.org/10.1159/000102097.

Figure 1
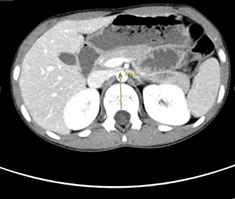
Figure 2
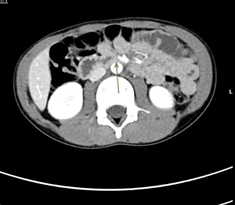
Figure 3

Figure 4