Research on Hassle Corpus Cells in Thymus
Research on Hassle Corpus Cells in Thymus
Kunal Joon*1
*Correspondence to: Kunal Joon, Department of Anatomy, NIIMS greater Noida, Plot no 17a str.no: sector 17, greater Noida, India, 203201.
Copyright
© 2023 Kunal Joon. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 September 2023
Published: 30 October 2023
Abstract
Hassle corpus cells are located in the thymus and constitute of type 6 epidermal. Reticular cells and the research describe about the function and significance of Hassel corpus cells and its significance of these cells in thymus and what it secretes:
1. Structure of hassle corpus cells. These are formed of the type 6 epidermal reticulocyte and look like the pink gap structure in the microscopes (reference from thymus structure in microscopes).
2. Function of the hassle corpus cells in the thymus.
These cells basically secrete the immunosuppressive secretions and even.
Suppressive T cells which controls the functioning of the immune system.
3. These secetion can be used in the treatment of autoimmune disorders and will act on the immune cells and control them.
How auto immune disorders act
Due to non functioning of Hassel corpus cells excess of immune cells are formed and then thymus releases them due to which the immune cells released in excess can destroy their on body cells due to immaturation of cells.
How immune cells get mature
The immune cells mature through antigen recogination in the.
Thymus and immature immune cells are suppressed by the Hassel corpus cells in thymus.
And through this control and recombination mechanism immune cells are matured.
Significance of Hassel corpus cells
These cells are basically help in maturation of immune cells.
Helps in controlling auto immune disorders.
Helps in controlling leukemia.
How Hassel corpus cells help in controlling leukemia.
The WBC cell count can be controlled through the secretion of the.
Hassel corpus cells as they will secrete immunosuppressive t cells and immunosuppressive secretions. And is a cure of blood cancer.
Keywords: hassle corpus cells, immunopositive, immunonegative, immunoselective, autoimmune diseases, thymoma, myasthenia gravis.
Research on Hassle Corpus Cells in Thymus
Introduction
Hassle corpus cells are located in the thymus and constitute of type 6 epidermal. Reticular cells and the research describe about the function and significance of Hassel corpus cells and its significance of these cells in thymus and what it secretes.
1. Structure of hassle corpus cells.
These are formed of the type 6 epidermal reticulocyte and look like the pink gap structure in the microscopes (reference from thymus structure in microscopes).
2. Function of the hassle corpus cells in the thymus.
These cells basically secrete the immunosuppressive secretions and even
Suppressive T cells which controls the functioning of the immune system.
3. These secetion can be used in the treatment of autoimmune disorders and will act on the immune cells and control them.
How auto immune disorders act.
Due to non functioning of Hassel corpus cells excess of immune cells are formed and then thymus releases them due to which the immune cells released in excess can destroy their on body cells due to immaturation of cells.
How immune cells get mature.
The immune cells mature through antigen recogination in the.
Thymus and immature immune cells are suppressed by the Hassel corpus cells in thymus.
And through this control and recombination mechanism immune cells are matured.
Significance of Hassel corpus cells.
These cells are basically help in maturation of immune cells.
Helps in controlling auto immune disorders.
Helps in controlling leukemia.
How Hassel corpus cells help in controlling leukemia.
The WBC cell count can be controlled through the secretion of the.
Hassel corpus cells as they will secrete immunosuppressive t cells and immunosuppressive secretions. And is a cure leukemia
Experiment 1.
Aim: to see the live brain and functioning of the brain.
Materials and Methods
Materials required: brain mapping instrument and an demo person
Procedure
- Put the the brain mapping instruments on the demo person.
- Focus on thymus.
- And then take the slide of thymus and look on the thymus.
Observation
You will Observe the functioning of the thymus and immunosuppressive secretions are secreted from the thymus.
Result
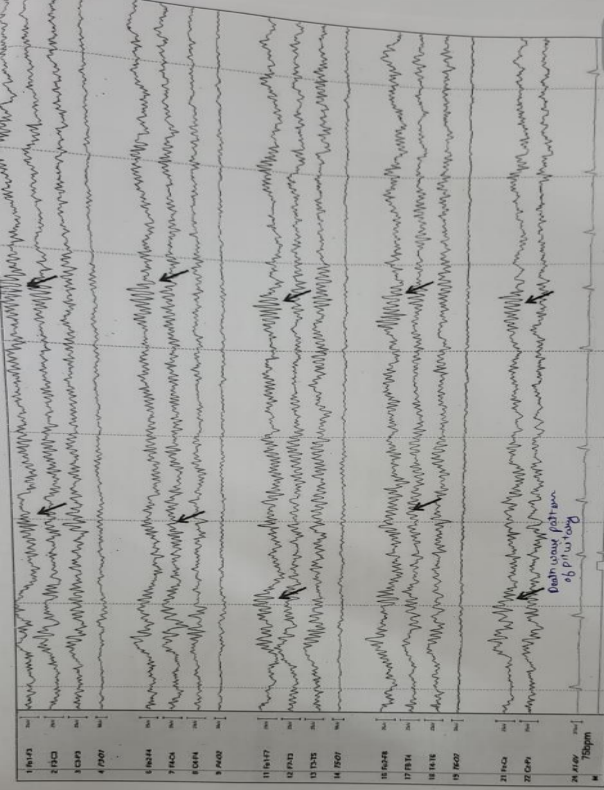
Fig. 1 shows an eeg of autoimmune diseased person with death wave pattern shown by an arrow.
Hassel corpus cells function and significance are known. Fig. 1 this chart is of autoimmune diseasesfrom science beam.
Fig 1 Autoimmune diseases electronic encephalon graph. (science beam qeeg graph)
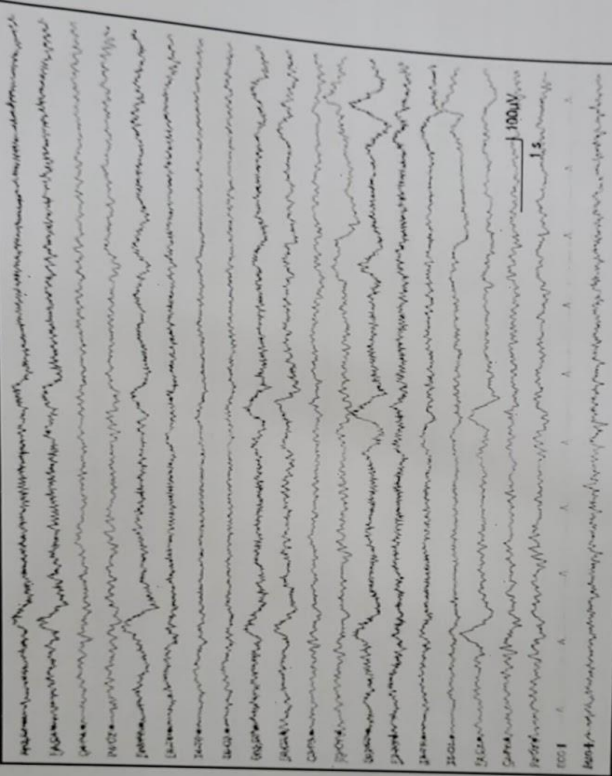
Fig. 2 shows normal eeg of a person with waves clearance.
Fig. 2. Normal electronic eceaphnoal grap.(science beam qeeg graph)
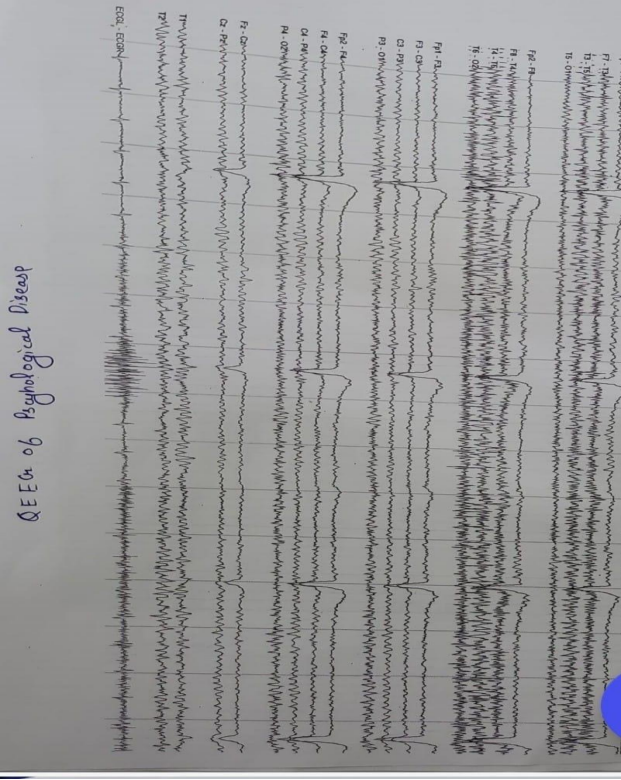
Fig. 3 shows an Pschyological diseased person eeg with wave disturbances.
Fig. 3. Mental disordered encephalograph graph. (Science beam qeeg graph)
Functions and fate of hassle corpus cells:
1. Thymus carcinoma vs Thymus hassles corpus cells.
Absence of hassle corpus cells in the cancer of thymus and the autoimmune diseases any autoimmune diseases can cause thymus cancer.their is decrease or no or Absence of hassle corpus cells in the autoimmune diseases [1].
2. Surrounding of B cells in auto immune diseases.
In the autoimmune diseases their is the presence irregular b cells around the hassle corpus cells which are stopping the secretion of the Hassel corpus cells [2].
3. Linkage of histology of brain and QEEG.
On studying eeg and histology of the brain of the autoimmune diseases the linkage between the eeg and histology is confirmed;
The release of the PCD ( death waves) waves in the thymus Environment Helps in the deletion of cloned T cells or irregular T cells. This PCD ( death waves ) signal coming from the thymus and pituitary gland in eeg indicates about the secretion of any hormones from the hassle corpus cells.
4. Hassle corpus cells formation
Components included in the formation of hassle corpus cells. In the foetus life in 17 th week the hassle corpus cells start developing. these are observed of different types. These are develped from the type 6 epidermal Reticular cells and these are definitely as graveyard of thymic cells and basically increases in the adults and defines difference between medullary and cortex area formed of macrophages , type6 epidermal Reticular cells , lymphocytes , interdigiating dendritic cells , mast cells , epithelial cells ( forms kerato hyaline boundaries) [3].
All sources of information used should be cited in the text of the article, in order, for example 1 to 10
5. Cortisol level of patients with autoimmune diseases.
In a general trend the patients with any thymus cancer and autoimmune diseases the cortisol level is low due to increase in the secretion of the of T cells
6. Genetherapy for treatment of autoimmune diseases and thymus cancer.
1st treatment
According to concept of DNA forward rolling.If the gene Is interested to the monoclonal antibody of thymus it can leaf to the treatment of the autoimmune diseases.
2 treatment is that
Activation of T cells by inserting the receptor recognizing gene (PRRs recognize specific pathogen-associated molecular patterns and) in the thymic T cells.
Permanent treatment of immune cells.
7. Link with immunological aging [4]
Development of hassle corpus cells starts from 17 th week and become prominent in the adults ages and start dissolving cloned cells and act as immunological clock of the all humans and slowly start developing and becoming prominent and start dissolving thymic cells and degeneration of thymus initiated and completed by them [5]
Formation of these hassle corpus cells increase by the increase in the age.
Types of hassle corpus cells
1) immunopositive hassle corpus cells.
2) lmmunonegative hassle corpus cells.
1. Immunopositive hassle corpus cells. these cells basically select the receptors for T cells and regulates them and generate the thymosin protein to generate more T lymphocytes and decrease with the increase in the age.
Mechanism of generation of thymosin in immunopositive hassle corpus cells.
Step 1: dissolving of the thymic or lymphocytes cells by macrophages.
Step 2: taking of protein and breaking it down into peptide by type 6 epidermal Reticular cells and conversion it into thymopoeitin and thymosin.
Step3: realising of thymopoeitin and thymosin by the mast cells.
These cell combine and work as triad unit.
2. Immunoinegative hassle corpus cells These cells basically produce immunosuppressive agents for cleaning of clones of T cells.
Steps of production of immunosuppressive secretions.
Step 1: first lymphocytes reacts with the lymphocytes component present in the hassle corpus cells.
Step2: starts a immune reaction and leads to stimulation of type 6 epidermal Reticular cells.
Leads to generation of peptide.
Step 3: conversion of peptides into cortisol and leads mast cells to production of the cortisol and elimination of the cloned cells.
Experiment 2
Aim: to observe slide of autoimmune diseased person and even QEEG of that person.
Material: slide of thymoma
Patient and QEEG of that person
Observation
8. Specfic pattern disturbance is observed in pituitary region (death wave).
9. No hassle corpus cells are observed in hassle corpus cells in the microscopes.
Result
- Linkage of eeg and histology (pathology) observed.
- Their are special reaction for autoimmune diseases.
Reference to above charts.
10. Specific condition for autoimmune diseases or autoimmune reaction.
Mechanisms
- In case of genetics the defective PRRs gene it leads to no development or less development of hassle corpus cells and lead to the the genetical autoimmune diseases.[6]
- In case of cancer the PPRs gene Is mutated which lead to thymmoma or thymic cancer and lead to autoimmune diseases.
11. Selection of T cells
In the selection T lymphocytes following steps
Step 1: the immature cells of T cells react with the type 6 epidermal Reticular cells and peptide is generated.
Step 2: monopeptide is than send to the mast cells for conversion of the peptide into receptor protein.
Step 3: receptor protein is attached to the T lymphocytes by lipase secreted by mastcells and leads to maturation of immune cells.[7]
Experiment 3
Aim: to observe the slide of fetal thymus in the high power microscopes.
Materials required: thymus slide of foetus of 15 week and 17 week Observation:
- In 15th week the cells from medullary region starts migrating downward.
- Hassle corpus cells starts developing in the 17th week Life of fetal life.
- Also observed different types of hassle corpus cells are observed.
Result
Hassle corpus cells are observed.
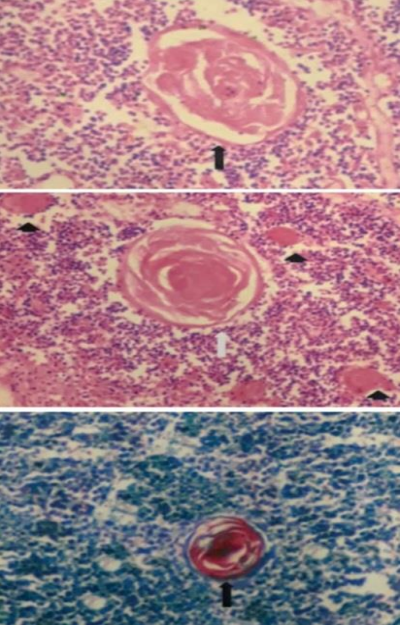
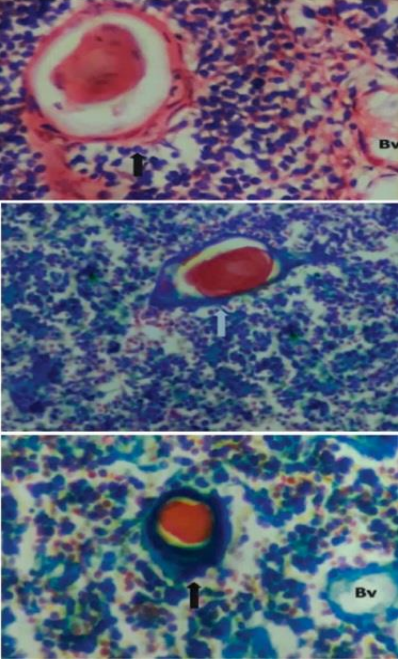
Fig. 4 hows an immuno negative Hassel corpus cells with its function that immune cell selection
Fig. 4. Immunoinegative hassle corpus cells. (vmc slide of thymus)
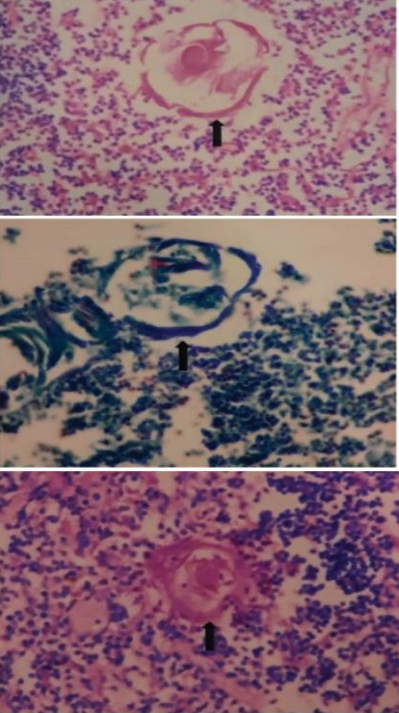
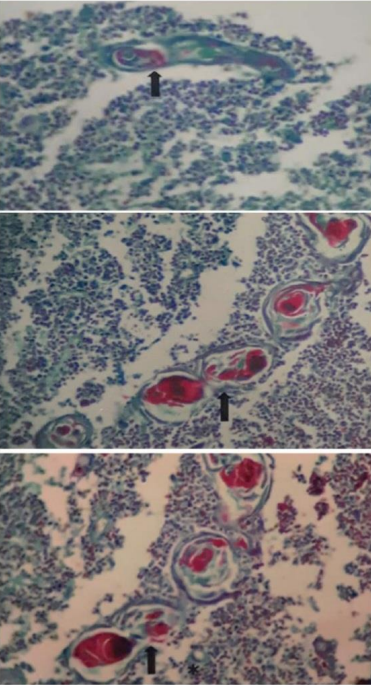
Fig. 5 foetal thymus cells are shown with lobulation showing development of hassle corpus cells.
Fig. 5. Foetal thymus cells. (vmc slide of thymus)
Fig. 6 formation of immunonegative hassle corpus cells are shown through foetal thymus cells.
Fig. 6. Formation of hassle corpus cells.(vmc slide of thymus).
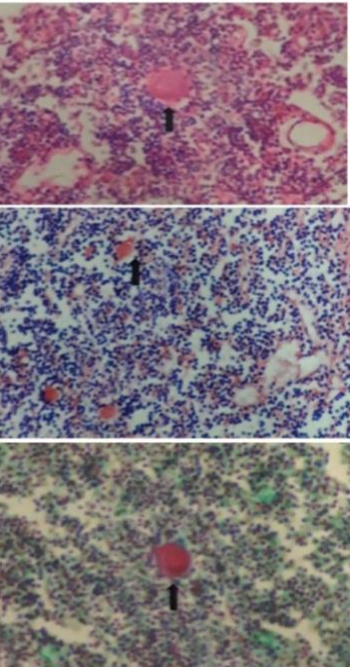
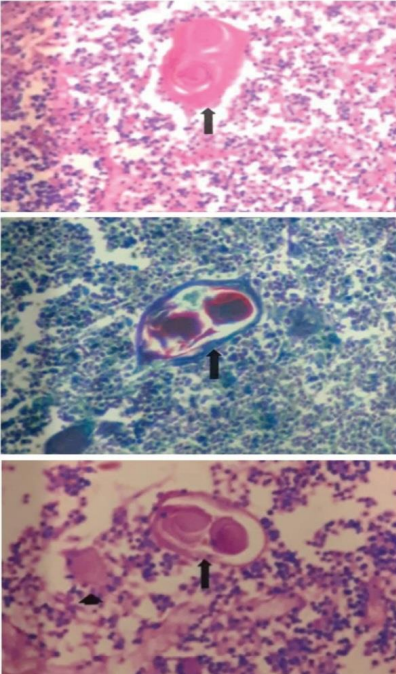
Fig. 7–9 show of essay of thymmoma patient (Fig. 9) and normal patient (7,8) these slide shows the importance of immunonegative Hassel corpus cells like in Fig. 7, 8 immunonegative hassle corpus cells present but in Fig. 9 no immunonegative hassle corpus cells are observed.
Fig. 7. Immunopositive hassle corpus cells
Fig. 8. Immunopositive hassle corpus cells.(vmc slide of thymus)
Fig. 9. Autoimmune diseases thymus slide.(vmc slide of thymus)
12) development of hassle corpus cells
- Development of hassle corpus cells start in the 16th week as the trabeculae are develped and lobulation occurs in the thymus [8].
- some Reticular cells are mesenchymal in nature and migrate to the medullary region.
- combines with the lymphocytes antigens present in the thymus , monocytes.
- and form juvenile hassle corpus cells and later on develop a keratin lining (secreted by the Reticular cells)and form developed hassle corpus cells.
Q Why the cells present in the hassle corpus cells are called type 6 epidermal Reticular cells.[9]
As during development these cells gain the ability to modify the peptide present in T cells and also ability to secrete immunosuppressive and immunoselective hormone and even modify peptide to form the receptor for T cells.
Discussion
- On finding from the experiment.
- Development of the hassle corpus cells.
- Function of the hassle corpus cells.
- Formation of the hassle corpus cells
- Fate of hassle corpus cells.
Conclusions
Conclusion is that the hassle corpus cells Helps In selection of T cells and immunosuppressive agents are also relesed for killing of colonal hassle corpus cells.
According to previous studies the development of hassle corpus cells and found its significance.
Function on the basis of the experiment done above Function are confirmed.
So reference of eeg are taken from Science beam qeeg graph of autoimmune diseases.
Reference
8. Rita Rezzani Thymus and aging: Morphological, radiological, and functional overview