Locally Advanced Carcinoma of the Cervix Uteri in a Bicornuate Uterus with a Note on Intracavitary Brachytherapy from an Academic Cancer Centre in India: A Case Report
Locally Advanced Carcinoma of the Cervix Uteri in a Bicornuate Uterus with a Note on Intracavitary Brachytherapy from an Academic Cancer Centre in India: A Case Report
Dr Shiva Kumar Siripuram *1, Mr Habeeb Rahman 2, Dr Niharika Darasani 3, Dr Bhavya raja Gopal Yarlagadda 4
1,2,3. Viswabharathi Medical College & General Hospital, Kurnool, Andhra Pradesh, INDIA
4. MUSC Kershaw Medical Center Camden SC 29020, USA.
*Correspondence to: Dr Shiva Kumar Siripuram, Radiation oncologist from Vishwabharathi Medical College(Kurnool, Andhra Pradesh, INDIA 518467) working as an assistant professor in the department of Radiation Oncology.
Copyright
© 2023 Dr Shiva Kumar Siripuram. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 October 2023
Published: 01 November 2023
DOI:https://doi.org/10.5281/zenodo.10164480
Abstract
Introduction: Carcinoma cervix is among the leading cancers in women across the globe, especially in developing countries. A bicornuate uterus is a rare anomaly of the uterus. Limited and non-unified published literature is available on approaching or dealing with challenges faced in planning non-surgical treatment with curative intent by chemo-radiation in cervical cancer with a bifid uterus, especially brachytherapy. This report entails the detailed management of a locally advanced case of carcinoma cervix in a lady with a bicornuate uterus, with a glimpse into the literature.
Case Summary: A 63-year-old postmenopausal, multiparous lady was evaluated for vaginal bleeding admixed with white discharge and lower abdominal pain and diagnosed with carcinoma cervix stage IIIB (HUN on imaging). The presence of a complete bicornuate uterus (IVa) and a history of surgery with internal fixation for an inter-trochanteric fracture of the right neck of the femur were significant findings apart from her malignancy. She received concurrent chemo-radiation by 3D-CRT with a dose of 50Gy in 25# (23# f/b two # parametrial boost) at a peripheral centre and was referred to us for brachytherapy. She received brachytherapy with HDR, four fractions of 6Gy each over two days, one week apart, with two fractions daily with a gap of 6-8 hours between each fraction. The application was done with Fletcher’s Suit, with an extra tandem into the non-dominant cornua rather than treating each cornu in alternate fractions, as done in some reports. The planning was similar to FS but with the other tandem supplementing the non-dominant cornua. The planned treatment was completed uneventfully. She is on regular clinical follow-up and disease-free on her last clinical visit.
Conclusion: In the rare instances of cervical cancer in women with a bicornuate uterus, better dose optimisation can also be achieved by using an additional tandem in the contralateral cornua as an adjunct to the Fletchers suit unit in comparison to treating alternate cornua in different fractions, and this could predict the radiation doses to the target better in comparison to the latter.
Keywords: Bicornuate uterus, Carcinoma Cervix, intracavitary brachytherapy, case report
Locally Advanced Carcinoma of the Cervix Uteri in a Bicornuate Uterus with a Note on Intracavitary Brachytherapy from an Academic Cancer Centre in India: A Case Report
Introduction
One or two paragraphs summarising why this case is unique (may include references)
Bicornuate uterus is a type of uterine duplication anomaly and can be classified as a class IV Mullerian duct anomaly. The incidence of uterine malformations is estimated to be 3-5% in the general population (1). A bicornuate uterus is even rare, with about 0.1-0.6% incidence (2). Carcinoma of the cervix in this clinical scenario is rarer, with no data on the prevalence.
This case adds to the literature of the same. Brachytherapy is integral to managing carcinoma cervix when radiation is planned as the curative modality. It becomes challenging to optimise the dose due to the anatomical abnormality. Brachytherapy has been delivered with the tandem alternated between the cornua with each fraction (3).
Patient presentation
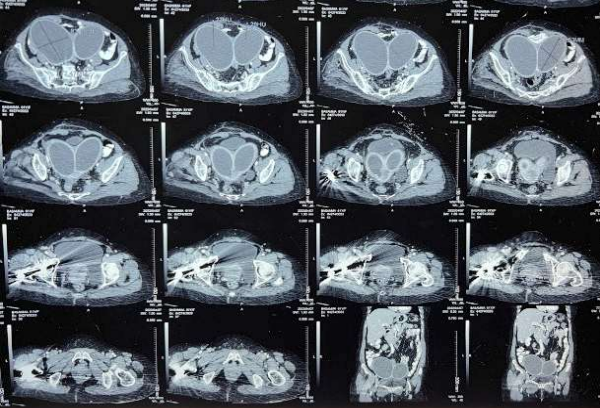
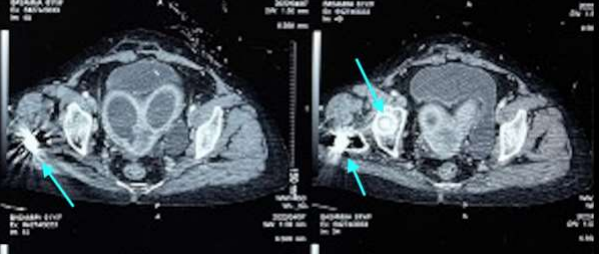
A 63-year-old, fit (ECOG 1) postmenopausal lady, G4P4A0, presented with postmenopausal bleeding with concurrent white discharge per vagina for four months and a history of lower abdominal pain for three months. She underwent surgery with internal fixation for a fracture of the right neck of her femur four years ago. She had no history suggestive of any co-morbidities. Clinically, there was an infiltrative lesion of size 3 x 3.5cm, destroying most of the cervix involving all the fornices and upper 1-1.5cm of the left lateral and posterior vaginal wall. The left parametrium was medially involved with the disease. A biopsy confirmed malignancy, and the histology was squamous cell carcinoma. Local imaging revealed left HUN, making the final diagnosis of IIIB, apart from the bicornuate uterus (Figure 1), with hydrometra in both cornua. The intramedullary nail (Figure 2) was a contraindication for MRI. Her family history was negative for miscarriages.
Figure 1: CT sections show a bicornuate uterus with hydro/pyo metra. The artefacts in the right proximal femur are due to the intramedullary implant.
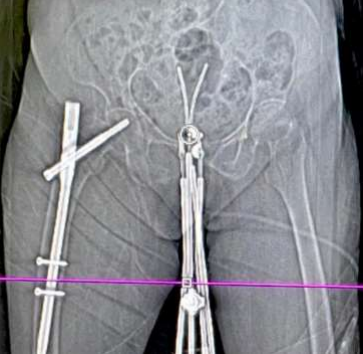
Figure 2: The implant (in the head, neck & proximal femur) is highlighted with cyan arrows.
Treatment and follow-up details
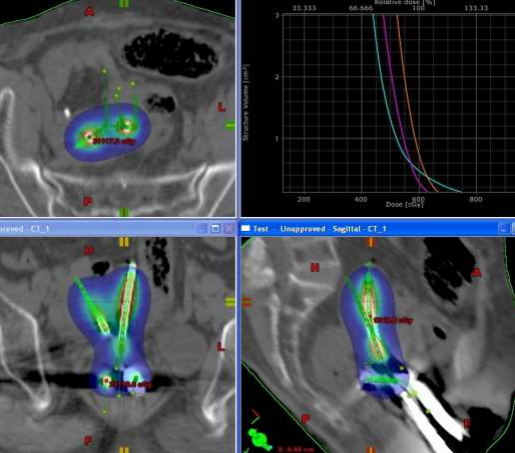
She received the planned EBRT of 50Gy/25# (23# of pelvic irradiation by four field box technique f/b two fractions parametrial boost) in April-May/2022 (last fraction of EBRT on 31/5/22) at a peripheral cancer centre with no brachytherapy facilities. She was referred to our Centre for brachytherapy to complete the treatment. Four fractions of intracavitary brachytherapy two days a week apart, two fractions each day, with a minimum of 6-8 hours between each fraction on each day of brachy delivery (on the 29th of June and the 6th of July 2022). The patient insisted on limited visits because of the long distance from her home. The dose per fraction was 6Gy, and a Fletcher suit with 2.0 cm ovoids was the applicator used for the ICBT. A free tandem(non-dominant) was used in the contralateral cornua, and the dose was optimised to maintain the target and organ at risk constraints. Source loading was done only in the free tandem's distal half to optimise the junctional region's dose. The free tandem was swapped between the cornua on the two days. Planning was done using Brachyvision Version 8.6, and treatment delivery was done with the Varisource machine (Figures 3, 4 & 5). The EQD2 to the target and OARs (in Gray) were as follows: Tumour (HRCTV)- 80, 2cc of bladder, rectum and sigmoid were 82.8, 74.2 & 78.1 respectively (ABS X-cel sheet was used for EQD2 calculation). At 15 months’ follow-up, the patient is disease-free.
Figure 3: Topogram at the time of brachytherapy simulation
Figure 4: Volume of the Bicornuate uterus with the reconstructed applicators
Figure 5: 6Gy distribution after the optimisation
Discussion
Given the rarity of the clinical scenario, there couldn’t be a single ideal way to approach brachytherapy where carcinoma cervix develops in a bicornuate uterus. Our case would be adding to the literature available on the same. Wang et al., in their recent report, have treated a similar patient with six fractions of brachy with the tandem applicator in each cornua for three applications and used volume optimisation as per the ICRU 89. (4) Fabian et al. treated a locally advanced case of carcinoma cervix in a bicornuate uterus with MRI guidance and a combined intracavitary and interstitial approach for the brachytherapy component. The tandem and the interstitial needles were swapped between the cornua for each fraction. The summary of a list of similar cases was also done well. (3) Lee et al. have used simultaneous loading of both the uterine canals during brachytherapy. They have used a newly defined prescription point midway between the two catheters and 2 cm above the mean cervical os position. (5) Loo et al. treated in a similar application but defined two Manchester A points and delivered with LDR (Caesuim-137, via a Nucletron Selectron).(6) A similar case reported by Cordoba et al. was treated with custom-made mould brachy and treatment delivered with pulsed-dose-rate (PDR).(7) A couple of cases where surgery was done as the definitive treatment have been reported.(8,9) The patients’ consent restricted us from further genetic testing. The table below summarises the cases of carcinoma cervix in the bicornuate uterus (or malformed uterus).
|
Author |
Patient specifics |
Rx Modality with detail |
|
|
Wang et al. (2023) |
25yrs, G1P0A1 |
CCRT with 6 applications of brachy (HDR), tandem in each cornua for 3 |
|
|
Gong et al. (2022) |
40yrs, G4P1A3 |
Laparoscopic Querleu-Morrow type A hysterectomy with salpingectomy (L) and partial vagina wall resection |
|
|
Fabian et al. (2019) |
30yrs, BRCA-1 positive |
CCRT with MRI guided IC/IS BT (HDR) |
|
|
Kaneyasu et al. (2019) |
61yrs, G0P0 |
CCRT with HDR brachy |
|
|
Ishibashi et al. (2018) |
|
CCRT with HDR brachy |
|
|
Guler Yavas et al. (2017) |
33yrs, Multiparous |
CCRT with HDR brachy |
|
|
Cordoba et al. (2017)
|
37yrs, Herlyn Werner-Wunderlich (HWW) syndrome; Multiparous |
CCRT with PDR brachy |
|
|
Jena et al. (2016) |
43yrs |
Surgery |
(9) |
|
Platta et al. (2014) |
34yrs, G4P3 |
CCRT with HDR brachy |
(13) |
|
Loo et al. (2010) |
45yrs, G0P0 |
CCRT with LDR brachy |
(6) |
|
Siripuram et al. (2023) |
63yrs, G4P4A0 |
CCRT with HDR brachy |
*present case |
Conclusion
Carcinoma of Cervix in a bicornuate uterus is extremely rare in consideration of uterine malformations per se. Appropriate and timely management is essential for the best clinical outcomes. Treatment principles of ICRU 89 would ensure the same. There couldn’t be a single best modality in this scenario owing to the rarity.
Reference
1. Borgohain D, Srivastava S. Pregnancy in bicornuate uterus. Int J Reprod Contracept Obstet Gynecol. 2018 Jan 1;7(1):346–9.
3. Fabian D, LaRocco A, Olsen M, Quick A. Treatment of locally advanced cervical cancer in a patient with a bicornuate uterus with MRI-guided intracavitary/interstitial brachytherapy. J Contemp Brachytherapy. 2019 Jun;11(3):285–91.
4. Wang L, Liu Z. Bilateral cervical cancer in a complete septate uterus with a double cervix and vagina: a case report. J Int Med Res. 2023 Mar;51(3):030006052311543.
5. Lee CD, Churn M, Haddad N, Davies-Humphries J, Kingston RK, Jones B. Bilateral radical radiotherapy in a patient with uterus didelphys. Br J Radiol. 2000 May;73(869):553–6.
6. Loo HW, Locks SM. Squamous cell carcinoma of the cervix: report of an unusual case of bicornuate bicollis uterus treated with bilateral intracavity brachytherapy. Br J Radiol. 2010 Jul;83(991):e143–6.
7. Cordoba A, Escande A, Comte P, Fumagalli I, Bresson L, Mubiayi N, et al. Locally advanced adenocarcinoma of the cervixon uterus didelphys: a case report. J Contemp Brachytherapy. 2017;1:71–6.
8. Gong Y, Xie Y, Chen L, Sui L. Cervical Cancer in a Septate Uterus with Double Cervix and Double Vagina: A Case Report and Review of the Literature. Int J Womens Health. 2022 Mar;Volume 14:345–51.
9. Jena A, Patnayak R. Rare case of cervical cancer arising in bicornuate uterus. J Dr NTR Univ Health Sci. 2016;5(3):241.
10. Kaneyasu Y, Koh I, Fujiwara H, Hirata E, Kudo Y, Arihiro K, et al. Concurrent chemoradiotherapy for locally advanced squamous cell carcinoma of the cervix in a uterus didelphys with vaginal septum. J Contemp Brachytherapy. 2019;11(2):180–8.
12. Yavas G, Yavas C, Inan G. Locally advanced squamous cell cervical cancer in a patient with septate uterus. J Contemp Brachytherapy. 2017 Oct;9(5):487–9.
13. Platta CS, Wallace C, Gondi V, Das R, Straub M, Al-Niaimi A, et al. Cervical brachytherapy technique for locally advanced carcinoma of the cervix in a patient with septate uterus. J Contemp Brachytherapy. 2014 Mar;6(1):76–81.