Bilateral Middle Cerebral Artery Occlusion (A Case Report)
Bilateral Middle Cerebral Artery Occlusion (A Case Report)
Dr. Abdulrahim Zwayed 1*, Dr Sreenivas A.V.2, Dr. Balola Miraghani 3,Dr. Amir M. Shabana 4, Khalood Al Mammari 5, Dr. Yasser Abdul Raziek 6, Dr. Mohammed Mahmoud Nassar 7, Dr. Atif Osman 8, Dr. Alaa Yasin Hasan 9, Dr Hilal Al Shibli 10, Dr. Mohammed Elghounim 11
1, 2 ,3: Department of Neurosurgery, Sohar Hospital, Sultanate of Oman.
4, 5: Anaesthesia: Sohar Hospital, Sultanate of Oman
6, 7, 8: Radiology: Sohar Hospital, Sultanate of Oman.
9, 10, 11: Intensive care unit: Sohar Hospital, Sultanate of Oman.
*Correspondence to: Dr. Abdulrahim H. Zwayed (Ph.D.) Department of Neurosurgery, Sohar Hospital, Sultanate of Oman.
Copyright
© 2024 Dr. Abdulrahim H. Zwayed, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 May 2024
Published: 03 June 2024
Abstract
Unilateral Malignant middle cerebral artery (MCA) infarction characterized by total occlusion of the MCA. They represent 8–15% of all cerebrovascular strokes. But bilateral Malignant MCA infarction is something unique.
We reported here a case of left MCA infarction managed surgically and patient improved then to be followed after 4 months with a new attack of MCA infarction of the right side which was managed conservatively.
Keywords: Middle cerebral artery MCA infarction, unilateral, bilateral.
Bilateral Middle Cerebral Artery Occlusion (A Case Report)
The case
This patient was a male of 72-years old, woke with right-sided weakness and found to have a left middle cerebral artery stroke on arrival to the emergency unit
He had no past history of transient ischemic attacks or stroke. He had no other cardiovascular risk factors or past medical apart from controlled hypertension with diet and medication and he was well before bed at midnight.
On examination: unconscious with responding to deep painful stimuli with flexion and eye opening to painful stimuli with right sided hemiplegia.
The CT brain, performed on arrival and showed acute left -sided distal MCA occlusion with a small core and large surrounding penumbra (Fig. 1.). The cause was thought to be cardioembolic in nature.
CT Angio-gram reported as: left MCA M1 is not opacifies by contrast with minimal opacification of M2 and distal branches that consisted with acute left MCA M1 thrombosis
The patient first underwent emergent mechanical thrombectomy but was of no benefit where repeated Head CT showed more infarction area with midline shift more than 5mm, so an urgent operation done as decompressive craniectomy with removal of the bone flap and embedded in the abdominal wall for further cranioplasty after a while.
The patient then shifted to the intensive care unit ICU for further management.
In the ICU and after few days, he was weaned from ventilator with tracheostomy at room air.
Fig. 1. Computer generated map showing a left -sided MCA infarction with midline shift of about 8 mm.
Fig 2: Decompressive craniectomy
Then he was shifted to the neurosurgical ward for further management.
He stayed in the ward for a while then discharged on advice for intensive physiotherapy
The patient was improved, whereafter 3 months he got cranioplasty (as replacement of the bone flap which was embedded in the abdominal wall) and replaced to close the cranial defect of the previous decompressive craniectomy.
Then the patient and after 4 months from the first attack he developed left sided hemiparesis.
CT showed infarction of the right side which progressed to paresis whilst on transfer to stroke unit for further management
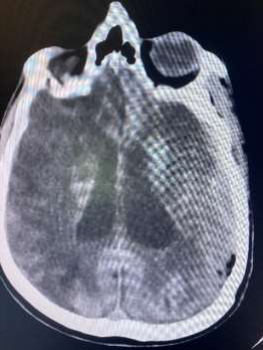
Fig 3: CT Brain showed a new right Middle cerebral artery MCA infarction.
The patient stayed in the stroke unit under neuro conservative treatment till discharge and advice for intensive physiotherapy in a specialized physiotherapy centre
The tracheostomy was closed after a while.
Frequent follow up for about 6 months and in the last visit he was conscious, on wheel chair with bilateral limb weakness (power of right side 4/5 and left sided 3/5) and his breathing at room air.
This patient with bilateral middle cerebral artery occlusions and made a recovery, first was with left sided MCA infarction which treated surgically and then after 4 months he developed another attack of MCA infarction of the other side and treated conservatively is something unique.
This case emphasises the importance of the early recognition of the middle cerebral artery occlusions and demonstrates that timely and effective treatment can have favourable outcomes for patients.
Discussion
In patients with an acute ischemic stroke, bilateral occlusion of the middle cerebral artery (MCA) is an extremely rare with an incidence of less than 1% (1,2,14) especially when occur at the same time but one side followed after a period of another side is also rare.
By another pathology There are few literature reports of bilateral M1 segment occlusion of the MCAs, which carries a poor prognosis often leading to coma, or death (12).
We present the case of a 72 -year-old male with acute left MCA M1 occlusion, detected on computed tomography (CT), then after a while he developed another attack of right MCA M1 occlusion on arrival from an external hospital. The patient underwent emergent endovascular mechanical thrombectomy with no benefit then urgent operation for the first attack and conservative for the second successful treatment and remarkable recovery. The purpose of this case report is to illustrate that timely management from arrival to intervention leads to favourable outcomes, and demonstrates the effectiveness of early management. (16,18)
Bilateral occlusion of both MCAs is usually due to cardiac disease, such as atrial fibrillation AF although dissection, cardiac embolism, and atherothrombosis are other possible causes (12,15)
Endovascular treatment with mechanical thrombectomy devices are usually the preferred treatment for patients with ischemic stroke, compared with thrombolytic drugs, which were previously used (6,8,13), but the last choice is for decompressive craniectomy after failure of the conservative management and if the patient deteriorates (5,7,9,10) .
Conclusion
Although rare, bilateral MCA needs to be considered in patients presenting with unilateral stroke like symptoms that acutely worsen to bilateral symptoms. (7,9,13)
Imaging is imperative for the diagnosis and therefore radiologists need to be familiar with the diagnosis.
This case report illustrates that importance of early recognition of MCA occlusion and that immediate endovascular treatment can lead to a favourable outcome and to prepar the patient for decompressive craniectomy once failure of the endovascular treatment (3,5,7,9,10)
Without time-efficient mechanical thrombectomy, patients with bilateral occlusion of their MCAs have a poor prognosis with likely catastrophic consequences. (1,5,11)
Bilateral middle cerebral artery (MCA) infarction stroke is a rare entity and is usually caused by inherent vasculature anomaly with superadded traditional risk factors of stroke. (8,13,16)
The spectrum of the presentation of bilateral MCA stroke is wide, including lower limb motor weakness, urinary incontinence, transcortical aphasia, extrapyramidal symptoms and an array of frontal cognitive impairments. In this report, we report a case of bilateral MCA infarct which occur within only 4 months starting with one side and treated then to be followed by the other side which carry a heavy burden on the patient giving hint of bad prognosis but fortunately our patient here survives with acceptable life style for such a big catastrophe. (4,11,17)
Reference
1. A. Consoli, A. Rosi, O. Coskun, et al.Thrombectomy for M1 - middle cerebral artery occlusion ,Stroke, 49 (2018), pp. 1286-1289 .
2 Ardutzky J, Schwab S. Antioedema therapy in ischemic stroke. Stoke. 2007;38:3084–94.
3 Bansal H, Chaudhary A, Singh A, et al. Decompressive craniectomy in malignant middle cerebral artery infarct: an institutional experience. Asian J Neurosurg. 2015;10(3):203–6.
4 Cho SY, Oh CW, Bae HJ, et al. The prognostic factors that influence long-term survival in acute large cerebral infarction. J Korean Neurosurg Soc. 2011;49(2):92–6.
5. Fandino J, Keller E, Barth A, et al. Decompressive craniotomy after middle cerebral artery infarction. Retrospective analysis of patients treated in three centers in Switzerland.Swiss Med Wkly. 2004;134:423–9.
6 Gwyn JC, Veenith T. Management of malignant middle cerebral artery infarction. EMJ Neurol. 2015;3(1):57–62.
7 Hofmijer J. Hamlet investigators. Surgical decompression for space-occupying cerebral infarction (Hemicraniectomy after Middle Cerebral Artery infarction with Life-Threatening Edema Trail [HAMLET]): a multicenter, open, randomized trial. Lancet Neurol. 2009;8:326–33.
8 Huttner HB, Schwab S. Malignant middle cerebral artery infarction: clinical characteristics, treatment strategies, and future perspectives. Lancet Neurol. 2009;8:949–58.
9 Jae Won YU, Choi J-H, Kim D-H, et al. Outcome following decompressive craniectomy for malignant middle cerebral artery infarction in patients older than 70 years old. J Endovasc Neurosurg. 2012;14(2):65–74.
10.Juttler E, DESTINY study group. Decompressive surgery for the treatment of malignant infarction of the middle cerebral artery: a randomized, controlled trial. Stroke. 2007; 38:2518–25.
11 Raffiq MA, Haspani MS, Kandasamy R, Abdullah JM. Decompressive craniectomy for malignant middle cerebral artery infarction: impact on mortality and functional outcome. Surg Neurol Int. 2014;26(5):102.
12. Ramos C., Aguirre C., Trillo S., et al. Bilateral middle cerebral artery stroke treated with double thrombectomy. Eur Stroke Org Conf. Online at: https://jounals.sagepub.com/doi/10.1177/2396987318770127 [last Accessed 01.12.19).
13.S. Pavabvash, S. Taleb, S. Majidi, et al. Correlation of acute M1 middle cerebral artery thrombus location with endovascular treatment success and clinical outcome, J Vasc Interv Neurol, 9 (2017), pp. 17-22.
14 S. Ueda, K. Fujitsu, S. Inomori, et al. Thrombotic occlusion of the middle cerebral artery Stroke, 23. (1992) pp. 1761-1766, .
15 U. Dietrich, T. Graf, W. Schabitz. Sudden coma from acute bilateral M1 occlusion: successful treatment with mechanical thrombectomy, Case Rep Neurol, 6 (2014), pp. 144-148 13
16 Vahedi K, Vicaut MJ, et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECEMIAL Trial). Stoke. 2007;38(9):2506–17.
17 Zaater AM, Refaat MI. Temporalis-based hinge craniotomy: technical modification of decompressive craniectomy in head injury. EJNS. 2014;29(2):49–52.
18 W. Hu, E. Wijdicks,Sudden coma due to acute bilateral M1 occlusion Mayo Clin Proc, 82 (2007), p. 1155