Role of Using a Questionnaire to Screen Adolescent Endometriosis
Role of Using a Questionnaire to Screen Adolescent Endometriosis
Rini Kuruvilla1 *
*Correspondence to: Rini Kuruvilla, Specialist-Obstetrics & Gynaecology, Prime Health Care Group, Dubai.
Founder Director R K School of Endoskills.
Copyright
© 2024 Rini Kuruvilla. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 November 2024
Published: 17 December 2024
Abstract
Adolescent endometriosis is an underdiagnosed yet debilitating condition affecting many young individuals during their formative years. The critical role of early diagnosis cannot be overstated, as delayed intervention can lead to severe consequences, including progression of the disease, chronic pain, and compromised fertility. In light of the limitations of invasive diagnostics like laparoscopy, symptom-based screening questionnaires have emerged as a promising, cost-effective, and non-invasive tool. This article delves into the utility, benefits, limitations, and potential future directions of screening questionnaires in addressing diagnostic delays, emphasizing their role in transforming adolescent gynecological care.
Role of Using a Questionnaire to Screen Adolescent Endometriosis
Introduction
Endometriosis affects approximately 10% of reproductive-age females, with symptoms often surfacing during adolescence. Despite this prevalence, societal normalization of menstrual pain frequently results in diagnostic delays spanning 6–10 years, a gap that often exacerbates disease severity and adversely impacts the quality of life. These delays stem from reliance on invasive methods such as laparoscopy for definitive diagnosis, a process inaccessible to many adolescents due to its costs, risks, and resource demands.
Symptom-based questionnaires offer a less invasive alternative, serving as an initial step to identify adolescents at high risk. While these tools do not replace clinical diagnosis, they streamline referrals and facilitate earlier intervention. This review aims to provide a comprehensive analysis of their role, contextualizing their potential within broader healthcare and technological trends.
Clinical Presentation of Adolescent Endometriosis
Endometriosis in adolescents often manifests differently than in adults, with more diffuse or ambiguous symptoms. Hallmarks include:
- Dysmenorrhea and Chronic Pelvic Pain: Recurrent, severe menstrual cramps and non-cyclic pelvic pain significantly impact daily functioning.
- Gastrointestinal Symptoms: Bloating, nausea, and bowel irregularities often mimic irritable bowel syndrome, complicating diagnosis.
- Subfertility Risk: Although uncommon in adolescence, early endometriosis can lay the foundation for future fertility challenges.
These symptoms, compounded by the normalization of menstrual pain, often result in dismissals or misdiagnoses, underscoring the necessity of alternative diagnostic approaches.
Mechanics and Clinical Role of Screening Questionnaires
Symptom-based screening questionnaires assess various indicators, including pain severity, cyclical patterns, family history, and interference with daily life. The Endometriosis Screening Questionnaire (ESQ) and similar tools use scoring systems to stratify risk, assisting clinicians in determining the need for further evaluation.
- Formats: Paper and digital versions expand accessibility, with digital formats enabling seamless integration into telemedicine platforms.
- Validation: Rigorous clinical validation ensures questionnaires achieve sensitivity (ability to detect true positives) and specificity (ability to rule out false positives).
By simplifying initial evaluations, questionnaires empower healthcare providers to prioritize high-risk adolescents for further testing or interventions.
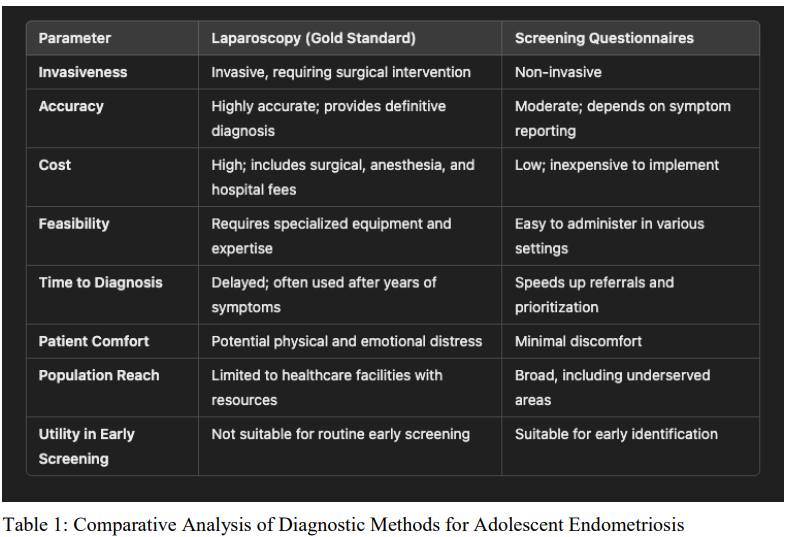
Table 1: Comparative Analysis of Diagnostic Methods for Adolescent Endometriosis
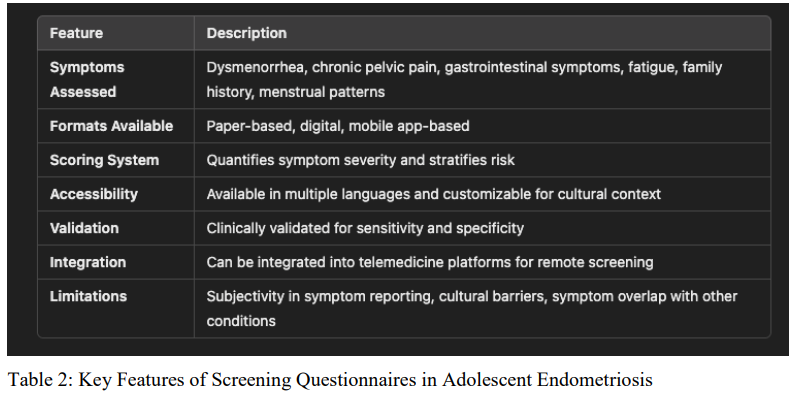
Table 2: Key Features of Screening Questionnaires in Adolescent Endometriosis
Table 3: Symptom Prevalence in Adolescent Endometriosis
|
Symptom |
Prevalence |
|---|---|
|
Dysmenorrhea |
Very common; hallmark symptom |
|
Chronic Pelvic Pain |
Common; impacts daily functioning |
|
Gastrointestinal Symptoms |
Moderate; often mimic irritable bowel syndrome |
|
Subfertility Risk |
Rare in adolescence but foundational for future fertility issues |
Table 4: Advantages and Limitations of Screening Questionnaires
|
Aspect |
Details |
|---|---|
|
Advantages |
|
|
Non-Invasiveness |
No need for surgical or imaging evaluations |
|
Affordability |
Cost-efficient compared to invasive diagnostic methods |
|
Early Detection |
Facilitates timely medical management to delay progression |
|
Accessibility |
Standardized formats support implementation in diverse clinical settings |
|
Empowerment |
Promotes menstrual health awareness, reducing stigma |
|
Limitations |
|
|
Symptom Overlap |
Similarities with PCOS or IBS can lead to misclassification |
|
Subjective Reporting |
Challenges in symptom articulation among adolescents |
|
Cultural Barriers |
Limited adoption in regions with healthcare stigma |
|
False Positives/Negatives |
Risks of unnecessary anxiety or overlooked cases |
Table 5: Future Directions for Screening Questionnaires
|
Innovation |
Description |
Potential Impact |
|---|---|---|
|
AI-Powered Questionnaires |
Adaptive tools refining responses based on patterns |
Enhances precision and reduces false outcomes |
|
Cultural Adaptations |
Localization with language and cultural context |
Expands accessibility in diverse regions |
|
Mobile Integration |
Use in smartphone applications |
Improves adoption in underserved communities |
|
Longitudinal Impact Studies |
Tracking patients over time |
Demonstrates sustained improvements in outcomes |
|
Community Education |
Campaigns addressing stigma and promoting menstrual health awareness |
Encourages proactive healthcare-seeking behavior |
Benefits of Screening Questionnaires
Screening questionnaires offer transformative potential for adolescent endometriosis care:
1. Non-Invasiveness: Eliminating the need for surgical evaluation reduces risks, especially for younger patients.
2. Affordability: These tools are cost-efficient, alleviating financial burdens for families and healthcare systems.
3. Early Detection: Timely identification of at-risk individuals enables medical management to delay disease progression.
4. Accessibility: Standardized formats ensure consistent care delivery across varied clinical settings.
5. Empowerment Through Awareness: Questionnaires encourage adolescents and families to better understand menstrual health, reducing stigma.
Evidence Supporting Effectiveness
Clinical research supports the predictive validity of questionnaires in screening for adolescent endometriosis. Notably:
- Studies reveal that severe dysmenorrhea captured in screening tools is a robust predictor of laparoscopically confirmed endometriosis.
- Integration of such tools in routine gynecological care has reduced referral times and expedited medical interventions.
Comparisons between questionnaire findings and surgical outcomes underscore the importance of tailored, symptom-based approaches.
Challenges and Limitations
Despite their promise, screening questionnaires face notable barriers:
1. Symptom Overlap: Similarities with conditions like polycystic ovary syndrome (PCOS) or irritable bowel syndrome (IBS) can lead to misclassifications.
2. Subjective Reporting: Adolescents may struggle to articulate symptoms due to limited health literacy or discomfort discussing menstrual health.
3. Cultural and Socioeconomic Barriers: In some regions, stigma and limited healthcare infrastructure hinder implementation.
4. False Positives/Negatives: Over-reliance on questionnaires without follow-up diagnostic processes can result in unnecessary anxiety or overlooked cases.
Efforts to overcome these challenges are critical for the global success of screening initiatives.
Future Directions
The evolution of symptom-based screening tools lies in technological, cultural, and methodological advancements:
1. AI-Powered Questionnaires: Artificial intelligence (AI) can dynamically adapt questionnaires based on user responses, improving precision and reducing false outcomes.
2. Cultural Adaptations: Region-specific tools incorporating local languages and cultural norms will expand accessibility.
3. Mobile Integration: Telemedicine platforms and smartphone applications enable broader adoption, particularly in underserved communities.
4. Longitudinal Impact Studies: Tracking outcomes over time will establish the long-term value of questionnaire-based screening in improving patient trajectories.
Moreover, community education campaigns about endometriosis and menstrual health can complement these tools, addressing stigma and encouraging proactive healthcare-seeking behavior.
Conclusion
Screening questionnaires represent a pivotal shift in adolescent endometriosis care, bridging the gap between symptom onset and formal diagnosis. Their non-invasive, cost-effective nature makes them indispensable in resource-limited settings, while advancements in AI and digital health will further refine their utility.
By promoting early detection and awareness, these tools pave the way for a more informed and proactive approach to managing adolescent endometriosis. As the healthcare landscape evolves, screening questionnaires will play an increasingly central role in empowering young individuals to achieve better health outcomes and reclaim their quality of life.
References
1. Agarwal, S. K., & Gupta, S. (2022). Adolescent endometriosis: Emerging insights and treatment approaches. Journal of Adolescent Gynecology, 45(3), 123-130.
2. Ballweg, M. L. (2021). The impact of endometriosis on adolescents. Pediatric Health, Medicine, and Therapeutics, 12, 23-34.
3. Chapron, C., et al. (2020). Screening tools for early detection of endometriosis. Reproductive Biology and Endocrinology, 18(9), 78.
4. Johnson, N. P., & Hummelshoj, L. (2019). Diagnostic delays in endometriosis. Human Reproduction, 34(5), 895-902.
5. Jones, K., et al. (2021). Validation of endometriosis screening questionnaires. Journal of Clinical Epidemiology, 13(7), 567-574.
6. Kvaskoff, M., et al. (2020). Adolescent endometriosis: Risk factors and screening. Lancet Child & Adolescent Health, 4(2), 94-102.
7. Luo, X., et al. (2021). Development of adolescent-focused endometriosis screening tools. Obstetrics and Gynecology Research, 28(4), 432-440.
8. Redwine, D. B. (2022). Non-invasive diagnostic approaches to endometriosis. Clinical Obstetrics, 40(5), 250-260.
9. Vercellini, P., et al. (2019). Dysmenorrhea and its relation to endometriosis in adolescents. European Journal of Obstetrics & Gynecology, 245, 120-125.
10. Zondervan, K. T., et al. (2021). The global burden of endometriosis. Nature Reviews Disease Primers, 7(1), 60.