Cardiac Amyloidosis, Something More Common than we Think. Review of the State of the Art.
Cardiac Amyloidosis, Something More Common than we Think. Review of the State of the Art.
Dr. Geordan Goire Guevara, MD. FACC.*1
*Correspondence to: Dr. Geordan Goire Guevara, Department of Internal Medicine of Spanish Town Public Hospital, Jamaica. Consultant General and Interventional Cardiologist at Partner Interventional Centre of Jamaica and Heartdent Center Limited.
Copyright
© 2025 Dr. Geordan Goire Guevara. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 Dec 2024
Published: 02 Jan 2025
Abstract
Cardiac amyloidosis is a condition caused by extracellular deposits of amyloid proteins in the heart muscle. Until a few years ago, it was considered a rare entity. However, the advent of new diagnostic methods and the increasing clinical suspicion have shown that this disease is more common than previously suspected. Its diagnosis and treatment depend on the clinical history, immunohistochemical, imaging and genetic studies, and histopathological identification of amyloid deposits. Risk stratification and identification of the type of circulating or tissue-deposited amyloid protein will determine the appropriate treatment method for each patient. Genetic screening should also be performed on relatives of patients with hereditary forms of the disease. The following review provides a context for the current state of the art of this disease.
Keywords: cardiac amyloidosis, amyloid protein, immunohistochemical studies.
Cardiac Amyloidosis, Something More Common than we Think. Review of the State of the Art.
Introduction
Amyloidosis is the general term used to refer to the extracellular tissue deposition of highly ordered fibrils composed of low molecular weight subunits of a variety of proteins, many of which, in their native form, circulate as normal constituents of plasma. Amyloid deposits may result in a wide range of clinical manifestations depending upon their type, location, and amount.
At least 38 different human protein precursors of amyloid fibrils are known. Some are produced at the site of amyloid formation (localized amyloid) and some circulate in the blood to deposit in a variety of tissues and organs (systemic amyloidosis)1,2.
Amyloidosis results from the predominantly extracellular tissue deposition of fibrils composed of low molecular weight subunits of a variety of proteins, typically in the range of 5 to 25 kD. Genetic factors play an important role in many forms of amyloidosis. Point mutations, deletions, and premature stop codons may result in structural changes predisposing to fibril formation (fibrillogenesis) by these proteins and the development of amyloid. Depending upon the type of amyloidosis, factors affecting protein folding and stability, including molecular chaperones and failure of disaggregating pathways, may be operative3.
These low molecular weight subunits are derived from soluble precursors and undergo conformational changes that lead to the adoption of a predominantly antiparallel beta-pleated sheet configuration in which state they auto-aggregate in highly ordered fibrils4-7. Oligomeric intermediates that are pre-fibrillar may contribute to tissue toxicity and disease pathogenesis in certain amyloid related disorders8.
Several types of amyloidosis are clearly hereditary, and clinical disease has been linked in most familial forms to missense mutations of the precursor proteins. In some instances, deletions or premature stop codon mutations have been described4,9.
Virtually all heredofamilial amyloidoses associated with nephropathic, neuropathic, or cardiopathic disease are dominantly inherited heterozygous disorders, and both the wild-type and mutant molecules can be identified in the amyloid deposits. In some instances (eg, transthyretin [TTR], apolipoprotein A-I [ApoAI], Alzheimer APP, and prion protein [PRP]), both the wild-type and mutant molecules are able to form amyloid fibrils under different circumstances, with the wild-type protein implicated in aging-associated diseases. As an example, wild-type TTR; ApoAI; and the beta protein, A-beta, a cleavage product of APPs, may form deposits in association with organ-specific pathology in the aging heart, aorta, and brain, respectively9-11.
Types of amyloidosis
There are 18 different types of systemic and 22 localized forms of amyloidosis12. The principal systemic types seen in tertiary referral centers and inpatient medical services are the primary (immunoglobulin light chain [AL]) and transthyretin (ATTR) types. However, other types of amyloid (eg, secondary [AA]) are clinically important, some of which are common and others rare. A review of more than 11,000 patients seen at a single center from 1987 through 2019 showed that systemic AL amyloidosis accounted for 56 percent, ATTR 21 percent, and AA 8 percent of typed cases13; in particular, there has been a substantial increase in the recognition of systemic amyloid due to ATTR in major referral centers. Nomenclature for amyloid subunit proteins includes the letter "A," followed by the abbreviation of the name of the precursor protein. Major forms include:
- AL amyloid: AL amyloid, caused by a plasma cell dyscrasia, is due to deposition of protein derived from immunoglobulin light chain fragments.
- ATTR amyloid: ATTR amyloid may occur as a "wild-type" (ATTRwt) associated with aging or as mutant proteins (ATTRv or hATTR [where v indicates a variant and h indicates hereditary; these were formerly termed ATTRm, to indicate a mutant protein]) associated with familial neuropathy and/or cardiomyopathy13.
- AA amyloidosis: AA amyloidosis is a potential complication of chronic diseases in which there is ongoing or recurring inflammation that results in sustained high-level production of serum amyloid A protein, an acute phase reactant, which can form amyloid deposits.
- Other types of amyloidosis: Additional forms of amyloid seen clinically include dialysis-related amyloidosis, heritable amyloidosis, organ-specific amyloid, leukocyte cell-derived chemotaxin-2 (LECT2) amyloid, insulin amyloid14, and others.
In this review, it will be just made reference to AL amyloidosis, ATTRwt, and (ATTRv or hATTR) since these types are the commonest found causing affectation of the cardiovascular system.
AL amyloid cardiomyopathy (AL-CM)
Clinical features
AL amyloidosis is a rare condition associated with plasma cell dyscrasias that has an annual incidence of approximately 1 per 100,000 people in the United States15.
Patients with AL amyloidosis typically present at age ≥40 years. Systemic AL amyloidosis is a multisystem disorder which commonly affects the liver, kidneys, spleen, the autonomic and peripheral nervous systems, lungs, and heart. Cardiac amyloid infiltration is present in most patients with AL amyloidosis (50 to 70 percent) and it is the main determinant of prognosis16,17.
Cardiac amyloidosis typically presents with symptoms and signs such as dyspnea, lower extremity edema, elevated jugular venous pressure, hepatic congestion, and ascites, which are caused by restrictive cardiomyopathy with predominantly right ventricular failure; symptoms and signs of low cardiac output (eg, diminished pulse pressure and diminished capillary refill) are features of advanced disease. Angina is uncommon, although microvascular dysfunction is a frequent finding. Amyloidogenic light chains may be toxic to myocardial cells as suggested by in vitro studies18,19 as well as clinical observation of worse symptoms in patients with AL amyloidosis compared with patients with ATTR amyloidosis with similar degrees of cardiac involvement.
Patients with cardiac amyloidosis also frequently present with syncope or presyncope20. Syncope is frequently caused by bradyarrhythmias or advanced atrioventricular block and is infrequently caused by ventricular arrhythmia.
Other conditions may contribute to the risk of syncope in patients with amyloid cardiomyopathy including postural or exertional hypotension caused by excessive diuresis or autonomic neuropathy.
Patients with AL amyloidosis or atrial fibrillation, are at risk for cardiac thromboembolism. Amyloid deposits in atrial as well as ventricular walls and thus causes atrial dysfunction including atrial electromechanical dissociation during sinus rhythm with associated risk of atrial thrombus formation21-23.
ATTR amyloid cardiomyopathy (ATTR-CM)
Clinical features
The spectrum of clinical presentations in patients with ATTR amyloidosis obliges all clinicians to be aware of common disease patterns, additional clues, and commonly affected populations.
Patients with ATTR-CM typically present at age ≥60 years, and most commonly >70 years. Various transthyretin mutations are associated with differing ages of onset (ranging from 30 to 70 years) and differing risks of cardiomyopathy. Cardiac amyloidosis is the dominant feature of wild-type ATTR amyloidosis (ATTRwt amyloidosis) and for some ATTR variants (eg, Val122Ile, Thr60Ala, Ile58Leu, and Leu111Met)15,24-26.
Suspicion of ATTR-CM should be triggered in older persons who have been hospitalized for HF, elevated troponin levels, or levels of NT-proBNP (N-terminal pro-brain natriuretic peptide) that are out of proportion to the clinical context. Other hints of ATTR-CM include hypertension that resolves over time and an intolerance of ACE (angiotensin-converting enzyme) inhibitors, angiotensin receptor blockers, or β blockers. In addition, though not infrequent in the general population, carpal tunnel syndrome occurs particularly frequently among males with ATTR-CM27. Lumbar spinal stenosis28,29, previous orthopedic procedures30, and spontaneous biceps tendon rupture31 may also be early indicators of ATTR-CM.
Patients with ATTR amyloidosis (wild-type or hereditary) often develop progressive conduction system disease and pacemaker implantation is often required. In contrast, patients with AL amyloidosis infrequently develop high-degree atrioventricular block or symptomatic sinus node dysfunction26.
Patients who develop ATTRwt amyloidosis and aortic stenosis have similar demographic features, and some patients have both cardiac ATTRwt amyloidosis and aortic stenosis18-20, 32. Cardiac ATTR amyloidosis has been identified in a substantial minority of patients with severe aortic stenosis undergoing surgical valve replacement (6 to 12 percent33,34) or transcatheter aortic valve implantation (TAVI; 16 percent35). It has been postulated that ATTR amyloidosis with associated restrictive cardiomyopathy may be a contributing cause of low-flow, low-gradient aortic stenosis32.
A study carried out by Westin O et al reported that screening for amyloid cardiomyopathy in patients with prior surgery for bilateral carpal tunnel syndrome finds approximately 5% with early-stage ATTR cardiomyopathy36.
Diagnosis
The following chart depicts some clinical, imaging and electrocardiographic clues in which cardiac amyloidosis should be suspected:
Chart 1. Diagnostic Clues to ATTR-CM
|
Clinical, Imaging and Electrocardiographic Clues: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The initial diagnostic evaluation of the patient with suspected cardiac amyloidosis includes a clinical examination to identify and assess cardiac and extracardiac symptoms and signs, laboratory tests, and an electrocardiogram, as described above.
An ECG and echocardiogram are the initial cardiac tests for patients with suspected cardiac amyloidosis.
ECG findings
A hallmark of cardiac amyloidosis is discordance between increased left ventricular wall thickness (identified by cardiac imaging such as echocardiography) and QRS voltage, which is often reduced. However, this feature of cardiac amyloidosis has low sensitivity and the prevalence of low voltage varies markedly with etiology, with higher frequency in patients with AL-CM (60 percent) than in patients with ATTR-CM (20 percent)23,37. Thus, the absence of low QRS voltage does not exclude cardiac amyloidosis, particularly in patients with ATTRwt amyloidosis.
Among patients with ATTRwt amyloidosis, 30 percent have voltage criteria for LV hypertrophy or left bundle branch block, and 70 percent have pseudo-infarction patterns; conduction abnormalities affecting the sinus node and His-Purkinje systems are also common. Thus, the presence of atrioventricular block in an older patient with left ventricle hypertrophy should prompt consideration of cardiac amyloidosis38.
Because the thickening of the ventricle in amyloidosis is due to myocardial infiltration rather than cardiomyocyte hypertrophy, the ECG limb lead voltage tends to decrease as the ventricle thickens and is often associated with extreme left axis or right-axis deviation. However, only ~50% of patients with AL-CM and about 25%-40% of patients with ATTR-CM meet true low-voltage criteria (that is, QRS amplitude <5 mm in limb leads or <10 mm in precordial leads23). Hence, the absence of low-voltage criteria does not exclude the diagnosis of cardiac amyloidosis.
Other common features present in the ECGs of patients with cardiac amyloidosis include left anterior hemiblock, ischaemic or nonspecific T wave abnormalities, and rhythm disturbances, particularly atrial fibrillation, which has been reported in up to 70% of patients with ATTRwt amyloidsis57. Ventricular arrhythmias are also common, although the first clinically apparent evidence of an abnormal ventricular rhythm might be ventricular tachycardia or fibrillation in the setting of a non-resuscitable cardiac arrest.
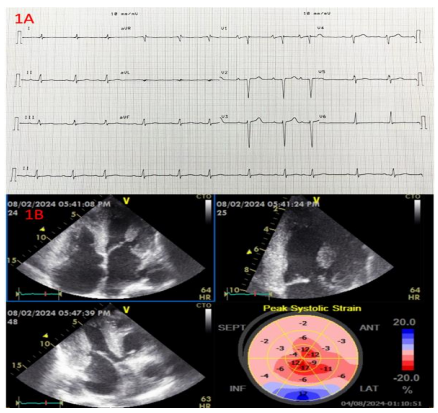
Figures 1A and 2A show two ECGs of patients with diagnosis AL and ATTRwt cardiomyopathies and the typical ECG findings.
Figure 1A. ECG performed to a 65-year-old patient with multiple myeloma and AL amyloid cardiomyopathy showing sinus rhythm with first degree atrioventricular block, low QRS voltage in most of limb leads (except lead II), and pseudo anterior infarction pattern with poor R wave progression in precordial leads. 1B. Echocardiographic apical 4 chambers, apical three chambers, apical 2 chambers views with the 2D GLS Bull’s eye display depicting left and right ventricular hypertrophy with granular sparkling pattern, biatrial enlargement, small ventricular cavities and thickening of the interatrial septum, very reduced GLS (-4.3%) and the typical relative apical sparing pattern on 2d GLS strain Bull’s eye display.
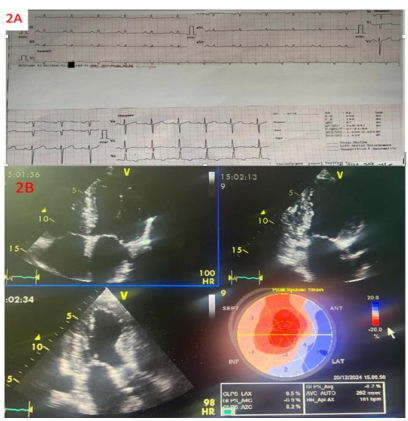
Figures 2A. ECG performed to a 59-year-old patient male with monoclonal gammopathy of unknown significance (MGUS) and ATTRwt amyloid cardiomyopathy what depicts sinus rhythm, low QRS voltage in the horizontal plane, pseudo-infarction pattern in precordial leads with non-specific T wave abnormalities in I-aVL and inferior leads and T wave inversion in V6 lead, left atrial enlargement signs and poor R wave progression in precordial leads. 2B. Echocardiographic apical 4 chambers, apical three chambers, apical 2 chambers views with the 2D GLS Bull’s eye display depicting idem findings like figure 1B.
Echocardiogram
Echocardiography is cost-effective, readily available, bedside to perform, and an excellent tool to identify systo-diastolic dysfunction. Although not always present, classic echocardiography findings of infiltrative disease include left ventricle wall thickening, small left ventricle cavity size, biatrial enlargement, thickened valves, elevated right ventricular systolic pressure and atrial septum thickness, granular sparkling appearance of the myocardial wall, pericardial effusion, restrictive transmitral Doppler filling pattern, and reduced ventricular strain, apical-to-basal strain ratio >2.1, left ventricle ejection fraction-to-strain ratio >439-41. (Table 1; Figure 1B and 2B).
The pulmonary artery systolic pressure, as estimated from the peak velocity of the tricuspid valve regurgitant jet, may indicate moderate pulmonary hypertension (estimated pulmonary artery pressure of 40 to 50 mmHg). This is almost invariably secondary to the markedly elevated left ventricle diastolic pressure and does not indicate primary pulmonary hypertension or cor pulmonale. Pericardial and pleural effusions are common findings, especially in AL-CM.
Reduction in global longitudinal strain (a measure of systolic function) is one of the earliest markers of cardiac amyloidosis and presents with a characteristic pattern of relative apical sparing of longitudinal strain (ie, the ratio of apical longitudinal strain/average of mid and basal longitudinal strain >1.0)41. This pattern of longitudinal strain alteration has high sensitivity (93 percent) and specificity (82 percent) for cardiac amyloidosis with proven utility in differentiating cardiac amyloidosis from other hypertrophic phenocopies41,42.
Cardiovascular magnetic resonance (CMR)
CMR is a key test in the diagnosis of cardiac amyloidosis and is generally performed with contrast43. CMR provides a detailed assessment of cardiac structure (including identification and quantification of left ventricle hypertrophy) and function as well as unique information on the characteristics of the myocardial tissue. CMR can detect early cardiac amyloidosis before the development of left ventricle hypertrophy. However, CMR cannot distinguish cardiac AL from ATTR cardiac amyloidosis44,45.
Cardiac amyloidosis has a highly characteristic appearance on CMR imaging performed with late gadolinium enhancement (LGE): Initially, there may be diffuse subendocardial LGE, while later in the course of disease, there is a transmural myocardial LGE pattern46. The three progressive LGE patterns identified in cardiac amyloidosis (none, subendocardial, and transmural) correlate with the degree of myocardial infiltration47. In a systematic review of studies comparing LGE with endomyocardial biopsy and/or echocardiography and other clinical features, the pooled sensitivity of LGE for cardiac amyloidosis was 85 percent (95% CI 77-91 percent) and the pooled specificity was 92 percent (95% CI 83-97 percent)48.
Limitations of LGE include lack of quantitative results (which limits the ability to track changes over time) and limited applicability since gadolinium-based contrast agents are relatively contraindicated in patients with a severe reduction in renal function (which is relatively common in patients with AL-CM).
T1 mapping can overcome some of the limitations of LGE but center-specific reference ranges are required for early disease detection49. T1 mapping provides quantitative measures of myocardial T1 relaxation time (precontrast [native] or postcontrast). Native myocardial T1 increases with cardiac amyloid infiltration and correlated with markers of systolic and diastolic dysfunction50.
Native myocardial T1 elevation is an early disease marker with high diagnostic accuracy for cardiac amyloidosis when the pretest probability is high51. In a study of 868 patients with suspected cardiac amyloidosis (222 with cardiac AL-CM, 214 patients with cardiac ATTR-CM, and 427 with no cardiac involvement), T1 mapping diagnosed cardiac amyloidosis with a sensitivity of 85 percent and specificity of 87 percent52. T1 mapping may be particularly helpful in patients with severely impaired kidney function, in whom gadolinium contrast is contraindicated. However, native T1 is a composite myocardial signal from both interstitium and myocytes that does not distinguish among the underlying processes (fibrosis, edema, amyloid, myocyte volume) and while the T1 elevation is marked with advanced disease, the lower elevations in early disease can be accurately identified only by referencing the center-specific normal range.
Extracellular volume (ECV) fraction measurement using intravenous gadolinium-based contrast agent is an ancillary method for identification and assessment of cardiac amyloidosis that helps to quantify the amount of cardiac amyloid. ECV elevation may be detected early before the development of left ventricle hypertrophy, LGE or elevation in serum biomarkers53. ECV elevation correlates with markers of disease activity, including cardiac function, serum biomarkers, patient functional performance54, and prognosis42, 55. Native T2 mapping is another technique that may be helpful; T2 elevations demonstrate that edema is part of cardiac amyloidosis (particularly AL-CM) and is linked to prognosis56.
Bone tracer cardiac scintigraphy
Bone tracer cardiac scintigraphy (using 99m technetium [Tc]-labeled 3,3-diphosphono-1,2-propanodicarboxylic acid [DPD], 99mTc-labeled pyrophosphate [PYP], or 99mTc-labeled hydroxymethylene diphosphonate [HMDP]) is an essential test for identifying ATTR amyloidosis.
The intensity of retention of bone-avid radiotracers in the heart can be interpreted by semi-quantitative visual analysis, by grading myocardial uptake to rib uptake on planar or single-photon emission computerized tomography (SPECT) imaging, and by quantifying radiotracer uptake using a heart-to-contralateral lung (H/CL) ratio58. The current diagnostic criteria for patients with ATTR-CM include visual myocardial uptake equal or greater than that in bone (specifically in the ribs) or a H/CL ratio ≥1.559. An H/CL ratio of ≥1.6 is associated with poor survival60.
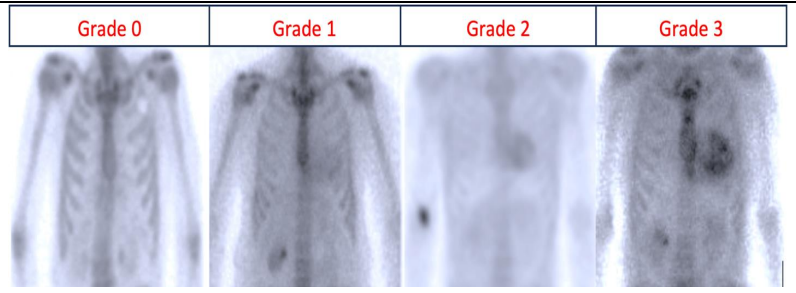
Perugini et al classified cardiac amyloid uptake based on a simple visual scoring system of the delayed (3 h) planar image, in which grade of 0 means no cardiac uptake, a grade of 1 means mild cardiac uptake (less than in bone), a grade of 2 means cardiac uptake greater than bone (but uptake in bone remains clearly visible) and a grade of 3 is indicative of substantial cardiac uptake with a weak or no signal evident in bone61. Figure 3.
A subsequent multicenter study showed that ATTR-CM is particularly avid for bone tracers (the mechanism is not understood); in contrast, in cardiac AL amyloidosis, there is either absent or only grade 1 uptake (grade 1 being present in approximately 40 percent of patients)35. As illustrated by a systematic review, the presence of grade 1, 2, or 3 scintigraphy had high sensitivity (pooled value of 82 percent) and specificity (98.8 percent) for cardiac amyloidosis as compared with tissue biopsy in studies evaluating the diagnostic performance of scintigraphy for cardiac amyloidosis44. Presence of grade 2 or 3 positive bone tracer cardiac scintigraphy in a patient without monoclonal protein (ie, free light chain ratio is normal and serum and urine immunofixation results are both normal) is highly specific for ATTR-CM and thus sufficient for diagnosis of this condition without tissue biopsy35.
Figure 3. 99mTc-DPD scintigraphy and Perugini visual scoring of cardiac uptake: Grade 0 represents no cardiac uptake, grade 1 represents mild cardiac uptake (less than that in bone), grade 2 represents cardiac uptake greater than that in bone (but bone uptake still remains visible), and grade 3 represents substantial cardiac uptake with only a weak or no signal evident in bone.
Positron emission tomography
Positron emission tomography (PET) is emerging as a useful diagnostic tool for cardiac amyloidosis. Several PET tracers such as 18F-florbetapir, 18F-florbetaben, 18F-flutemetamol and 11C-Pittsburgh B (C-PiB) have been used successfully to diagnose cardiac amyloidosis62. These tracers have been shown to bind specifically to brain β-amyloid plaques, allowing diagnosis and follow-up of patients with Alzheimer’s disease63. These tracers likely bind to the β-pleated structure of amyloid fibril, which facilitates the identification of amyloid deposits independently of the precursor protein.
PET tracers are quantitative tools, permitting the measurement of amyloid burden. Small studies have demonstrated that 18F-florbetapir is taken up in the heart of patients with cardiac amyloidosis, with a trend towards a higher myocardial retention index in patients with AL-CM versus those ATTR-CM, and no significant uptake in the healthy controls64, 65. Similar findings have been observed with 11C-PiB66, 67 and 18F-florbetaben68. In another small study 18F-florbetaben was evaluated in patients with AL-CM (n = 5) or ATTR-CM (n = 5) and compared with control patients with hypertension (n = 4).
Myocardial retention was higher in patients with AL-CM and ATTRCM compared with controls, and myocardial retention inversely correlated with LV global and RV free wall longitudinal strain68. However, an onsite cyclotron is required for the production of 11C tracers, given their short half-life of 20 mins. The longer half-life of 18F tracers (110 min) means that it can be distributed and used for research and clinical applications at sites without a cyclotron, making its use more practical compared with 11C-PiB tracers.
Dietemann et al. showed that 18F-flutemetamol target to background ratio (TBR) was significantly higher in amyloid subjects compared with control subjects69. They suggested that 18F-flutemetamol could be a promising tool in diagnosing and in therapy response assessment for patients with CA69.
Also, 18F-florbetaben is feasible for diagnosis of CA and might be useful in differentiating CA subtypes70. Kircher et al. showed that using semi-quantitative analysis, tracer retention was highest in patients suffering from AL, followed by patients with AA and ATTR, respectively70.
Monoclonal protein
Identification of monoclonal protein (by serum protein immunofixation, urine protein immunofixation, or serum free light chain ratio analysis) along with echocardiographic or CMR findings consistent with cardiac amyloidosis is suggestive of AL amyloidosis but may also be caused by ATTR amyloidosis (or a rarer cause of cardiac amyloidosis) with an unrelated monoclonal gammopathy of undetermined significance (MGUS)71.
The M protein in AL amyloidosis is IgG in approximately 35 percent, IgA in 10 percent, IgM in 5 percent, IgD in 1 percent, and light chain (lambda or kappa) in the remaining patients72. Most patients with AL amyloidosis have little or no intact monoclonal immunoglobulin, but are characterized by the presence of monoclonal free light chain. The monoclonal light chain type is lambda in approximately 70 percent of cases, kappa in 25 percent, and biclonal in 5 percent73.
Tissue biopsy
Tissue biopsy is not required when other findings are diagnostic for the presence and type of cardiac amyloidosis. As described above, the presence of grade 2 or 3 positive bone tracer cardiac scintigraphy in the absence of monoclonal protein is diagnostic for cardiac ATTR-CM, and thus no tissue biopsy is required. The presence of CMR findings consistent with cardiac amyloidosis in a patient with previously confirmed systemic AL amyloidosis is diagnostic for AL-CM, so endomyocardial biopsy is not indicated.
Endomyocardial biopsy is invasive, carries a small risk for serious complications, and requires technical expertise, whereas fat pad biopsy is less invasive and poses little risk but has varying sensitivity in ATTR-CM (with roughly 45% sensitivity for ATTRv and roughly 15% sensitivity for ATTRwt).74 Given the high false-negative rate from biopsies of nonclinically involved sites (eg, fat pad, bone marrow), further evaluation is warranted even in the presence of a negative biopsy from such sites if clinical suspicion remains elevated. In such cases, biopsy of a clinically affected organ (eg, endomyocardial biopsy) is imperative. Endomyocardial biopsy assessment with Congo red staining has ≈100% specificity and sensitivity for detecting amyloid deposits and is still considered the gold standard in situations with equivocal noninvasive findings.75
Diagnostic characteristics of extracellular amyloid deposits include typical apple-green birefringence with Congo red dye under polarized light microscopy and unique cross–β-pleated sheets under electron microscopy. The fibrils also bind thioflavine T (producing an intense yellow-green fluorescence), and sulfated Alcian blue (producing a green color). The type of amyloid fibril may be identified using immunohistochemistry, immunofluorescence or immunoelectron microscopy but laser microdissection with mass spectrometry is considered the gold standard for identifying the precursor protein and amyloidosis type.76
Genetic sequencing of the TTR gene
In the context of ATTR-CM is identified, then genetic sequencing of the TTR gene will determine if the patient has a pathological variant (ATTRv) or wild-type (ATTRwt) disease77.
Differentiating ATTRv from ATTRwt is important because confirmation of ATTRv would trigger genetic counseling and potential screening of family members and some presently approved therapies like inotersen and patisiran can be used only for ATTRv with polyneuropathy78, 79.
ATTRv is considered rare and is transmitted in an autosomal dominant manner and with variable penetrance. Certain variants typically result in cardiomyopathy, whereas others typically result in polyneuropathy, although cardiomyopathy and polyneuropathy manifestations may overlap. The prevalence of cardiomyopathy among persons with ATTRv is estimated at approximately 40 000 of the 50 000 persons with ATTRv globally80, but this may be an underestimate.
The most common worldwide TTR variant, Val122Ile (or pV142I), occurs in approximately 3% to 4% of black Americans, with undefined phenotypic penetrance81, 82. This Val122Ile TTR variant manifests predominantly as cardiomyopathy,83 and one estimatation shows 10% of black Americans with HF who are older than 60 are carriers of the Val122Ile TTR variant84. Thr60Ala, another common TTR variant, often manifests as a mixed phenotype, including cardiomyopathy, polyneuropathy, and gastrointestinal dysfunction and is present in approximately 1% of persons in northwest Ireland85. The Val30Met variant is the most common cause of ATTRv with polyneuropathy; however, late-onset ATTRv in patients of the Val30Met variant typically manifests as cardiomyopathy. Phenotypic penetrance of ATTRv is clearly age dependent; thus, ascertainment of population prevalence varies depending on age.
Laboratory tests
Laboratory test abnormalities in patients with cardiac amyloidosis include proteinuria which may or may not be accompanied by elevations of serum BUN and creatinine in patients with kidney disease and liver biochemical abnormalities (eg, elevation in serum bilirubin) in patients with congestive hepatopathy.
Natriuretic peptides and troponin T and I levels are commonly elevated in patients with cardiac amyloidosis21,22.
During the clinical assessment, the combination of very high plasma levels of NT-proBNP (disproportionate compared with the degree of HF) and elevated troponin levels in a patient with echocardiographic hypertrophic phenotype is strongly suggestive of amyloid cardiomyopathy and can prompt the diagnostic workup. NT-proBNP is a biomarker that is elevated early in ATTRv amyloidosis before cardiac symptoms appear, especially among asymptomatic carriers of a TTR gene mutation or patients with neurological symptoms only86. In addition, the usefulness of circulating retinol binding protein 4 in conjunction with electrocardiographic and echocardiographic measures to identify patients with HF who have ATTR-CM from the Val122Ile mutation has recently been reported87.
Staging
The Revised Mayo Stage system is the most acceptable use to staging AL amyloid cardiomyopathy and it is based on serum levels of N-terminal pro-B-type natriuretic peptide (NT-proBNP), cardiac troponin T, and free light chains88. The scoring system assigns 1 point for NT-pro-BNP ≥1800 pg/mL, troponin T ≥0.025 ng/mL, and difference between the kappa and lambda free light chains ≥18 mg/dL. Median survival for stage III patients was 14 months and for stage IV patients was 5.8 months88. Within stage III, NT-proBNP >8500 pg/mL combined with a systolic blood pressure <100 mmHg identifies a group of patients with the highest mortality (IIIb). Chart 2.
Chart 2. Prognostic staging systems for AL amyloidosis.
|
Prognosis Model |
Risk Groups |
Survival in patients not undergoing stem cell transplantation |
Survival in patients undergoing stem cell transplantation |
|||
|
Average in Months |
5-year Survival rate in (%) |
Average in Months |
4-year Survival rate (%) |
|||
|
Revised Mayo Stage System |
Stage I
|
NT-pro BNP <1800 ng/L, cardiac troponin T<0.025 mcg/L, and difference between involved and uninvolved serum free light chains <18 mg/dL |
55 |
50 |
Not reached |
87 |
|
Stage II
|
Presence of an elevated marker |
19 |
35 |
97 |
72 |
|
|
Stage III
|
Presence of two elevated markers |
12 |
20 |
58 |
56 |
|
|
Stage IV
|
NT-pro BNP ≥1800 ng/L, cardiac troponin T ≥0.025 mcg/L, and difference between involved and uninvolved serum free light chains ≥18 mg/dL |
5 |
15 |
22 |
46 |
|
ATTR amyloidosis
Two staging systems have been proposed in patients with ATTR amyloidosis:
The first published staging system for ATTRwt is based on serum levels of NT-proBNP and cardiac troponin T89. Thresholds of troponin T (0.05 ng/ml) and NT-proBNP (3000 pg/ml) were used. The respective four-year overall survival estimates were 57, 42, and 18 percent for stage I (both values below cutoff), stage II (one above), and stage III (both above), respectively.
The second staging system, validated in both ATTRwt and ATTRv, is based on serum levels of NT-proBNP and estimated glomerular filtration rate (eGFR)21. Stage I is defined as NT-proBNP ≤3000 ng/L and eGFR ≥45 mL/min, Stage III is defined as NT-proBNP >3000 ng/L and eGFR <45 mL/min, and the remainder were Stage II. Median survival among Stage I patients was 69.2 months, Stage II patients 46.7 months, and Stage III patients 24.1 months21.
Please click here to view complete article