Prevalence of Mandibular Wisdom Tooth Impaction among Sudanese People in Khartoum- A Radiological Study
Prevalence of Mandibular Wisdom Tooth Impaction among Sudanese People in Khartoum- A Radiological Study
Mohammed Ezzedine Abdullah 1*
*Correspondence to: Mohammed Ezzedine Abdullah.
Copyright.
© 2025 Mohammed Ezzedine Abdullah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 Jan 2025
Published: 30 Jan 2025
DOI: https://doi.org/10.5281/zenodo.14880743
ABSTRACT:
Background and Aims:- Impacted tooth is a tooth that did not grow on its expected time because of an incorrect position or lack of space. The impacted third molar is usually the most common impacted tooth. In the present study, the presence of impacted third molar and their level of eruption, their relation to anterior border of the mandible and their angulations were evaluated using panoramic radiographs .
Materials and Methods:- This is retrospective study. Sample sizes of 1720
Orthopantographs of patients above 18 years were interpreted for presence or absence of mandibular third molar, its level of eruption, its relation to the anterior border of the mandibular ramus, its angulation, its side distribution and the possibility to use the integration of the two types of third molar impaction classification namely Winter and Bell and Gregory in one case of impaction
Conclusion:- Out of 1720 OPTs females represented the highest percentage 07=938) 54% and males represented (n- 782) 45.5% The study showed females have higher susceptibility to impaction (17=268) 55 8% and males have lower susceptibility to impactions (n=212) 44 2% .
Mesioangular impaction was found to be the commonest type of impaction when using Winter's classification, and class 3 position A the commonest when using Bell and Gregory classification. According to Winters classification distribution of impaction by sides was equal. However according to Bell and Gregory classification bilateral impaction (class3 position A) was most common (1 1 4%) than unilateral impaction 1%
Integration of the two classifications used to determination of third mandibular impaction types in this study showed mesioangular type and class3 position C are the most common types integrated to other types of impactions,(n= 35) 7 2% .
These results could not be generalized for Sudanese therefore a larger number or even a population based study is needed to provide.
Prevalence of Mandibular Wisdom Tooth Impaction among Sudanese People in Khartoum- A Radiological Study
Introduction
The incomplete eruption of third molars remains a serious problem in oral and maxillofacial surgery, primarily because of its high incidence, clinical consequences and removal complications.
Indication for removal of impacted lower wisdom teeth are:
• Pericoronitis prevention or treatment:
When a mandibular third molar partially erupts through the oral mucosa, the potential for the establishment of a mild to moderate inflammatory response that is similar to gingivitis and periodontitis occurs. In cretin situations the patient may actually experience a severe infection, which may require extensive medical and surgical treatment.
•Prevention of dental disease:
Dental caries can occur in mandibular third molars or in adjacent second molars, most commonly at the level of cervical margin Owing to the patient's inability to effectively cleans this area and because the third molar is inaccessible for restorative treatment their removal may be the dission of choice.
•Orthodontic consideration 2.
The impacted third molar may be responsible for several orthodontic problems such as:
1 Crowding of mandibular incisors.
2 Obstruction of orthodontic treatment.
3 Interference with orthognathic surgery
•Prevention of odontogenic cysts and tumor
In the impacted third molar that is left intact in the jaw, the follicular sac that was responsible for the formation of the crown may undergo cystic degeneration and form a dentegerous cyst The overall incidence of complications and the severity of these complications are directly associated with the depth of impaction, that is, whether it is complete bony impaction, or partial impaction related to the age of the patient Another determinant of the incidence of complications of third molar surgery is related to experience of the surgeon. The less experience surgeon will have a significantly higher incidence of complications than the experienced surgeon
These complications are:
• Trismus.
• Dry socket
• Anastheia, parasthesia, dysathesia.
• Tempromandibular joint dislocation or subluxation
• Jaw fracture
Difficulty of accessibility to the side of partially unerupted third molar cause difficulty in maintaining good hygiene to the area Thus food and debris accumulation beneath the gingiva overlying partially erupted tooth (operculum) may lead to spread of infection to the pericoronal area and spreads to the neighboring soft tissues which may extend to distant areas like the neck, mediastinum and brain .
Impacted wisdom tooth may be associated with dental crowding , skeletal deficiencies particularly in lower jaw such as hypoplasia causes less space remaining for eruption due to space being occupied already by earlier
Eruption of the rest dental set. Pressure applied by wisdom tooth eruption to the neighboring teeth may lead to anterior dental crowding.
Pain is also a consequence of wisdom tooth impaction either due to mechanical trauma (biting the operculum by the opposing erupted tooth), dental disease from accumulated food and debris and acute myofacial pain in the Tempromandibular joint area
Even in the absence of clinical evidence the third molar tooth impaction is blamed for many problems like pain 6 , particularly after exclusion of other dental causes and referred pain from other regional structures such as the maxillary sinus, the ears and eyes
The aberrant or incomplete formation and organization of the dental tissue related to wisdom tooth were found to be a cause and origin of the conditions like cysts and neoplasms
The dentigerous cyst is a developmental odontogenic cyst that arises from epithelium of the enamel organ that encloses the crowns of unerupted teeth Few cases reported the neoplastic transformation potential of the epithelium of dentegerous cyst to benign tumors such as ameloblastoma and malignant tumors such as squamous cell carcinoma.
The exact cause of the transformation is still unknown but chronic inflammation might be the main factor leading to malignant transformation of the dentegerous cyst's epithelium .
Some generalized developmental or congenital condition that affect the basic developmental tissues like the ectoderm, can cause impaction of wisdom teeth. This is found in cleidocranial dysplasia, Down's syndrome, Gorlin-Goltz syndrome 9
Also impacted wisdom teeth were linked to medical conditions such as endocrine deficiencies like hypothyroidism, hypopituitrism, because these conditions affect calcium metabolism and growth hormones
Febrile disease and irradiation were also reported as causes of wisdom tooth impaction 10
Skeletal deficiencies particularly in lower jaw such as hypoplasia were found to be cause for wisdom tooth impaction as consequence of less space remaining for eruption due to space being occupied already by earlier eruption of dental set.
Some studies postulated genetic and human evolution relationship with wisdom tooth impaction Evolution leads to the human discovery of fire and more ways to softening food and therefore a decrease of musculoskeletal activity which is linked to the process of jaws growth This lead to genetic changes that are architectural and appear as large brain as it became the main tool of the humans rather than hands and other organs, this lead to narrower lower jaw so that it could still connect to the skull
The result is smaller lower jaw, less space for normal eruption of wisdom tooth or agenesis of the wisdom tooth 12
Studies conducted in prevalence of wisdom teeth impaction in Nigeria examined the difference in nutritional materials between the rural and urban population It was found that the wisdom tooth impaction is more common in urban population due to life style and types of nutritional materials 13
Many authors have suggested various classifications of mandibular wisdom teeth impactions depending on different criteria.
Two classifications from these were being adopted
1 -Winter's classification: - depend on angulation of wisdom tooth axis to the long axis of the second molar tooth 12
2-Bell and Gregory classification: - depends on depth of wisdom tooth into the ramus bone and relation of the wisdom tooth to the Occlusal plane of the second molar.
Winter's classification:-
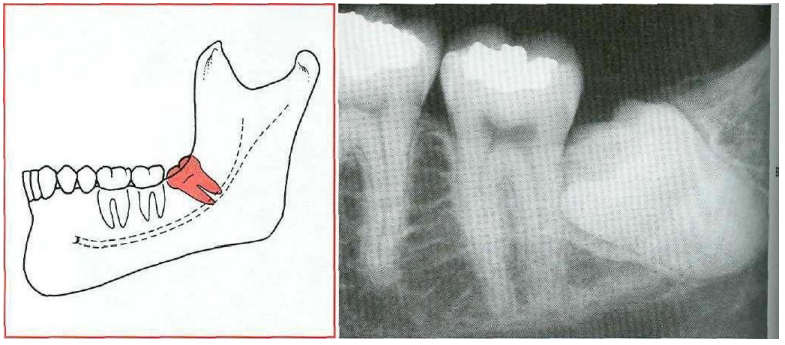
1 Mesioangular. The Mesioangular-impacted tooth is tilted toward the second molar in a mesial direction
Fig-I : Mesioangular impaction. "From Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry d. Peterson. Principles of management of impacted teeth p 194.
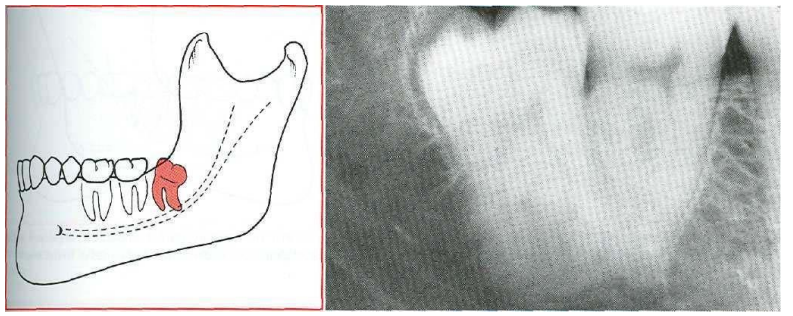
2-Distoangular 14
In the Distoangular impaction the long axis of the third molar is distally or posteriorly angled away from the second molar tooth
Fig .2: Distoangular impaction "From Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry J. Peterson. Principles of management of impacted tooth p 195 '
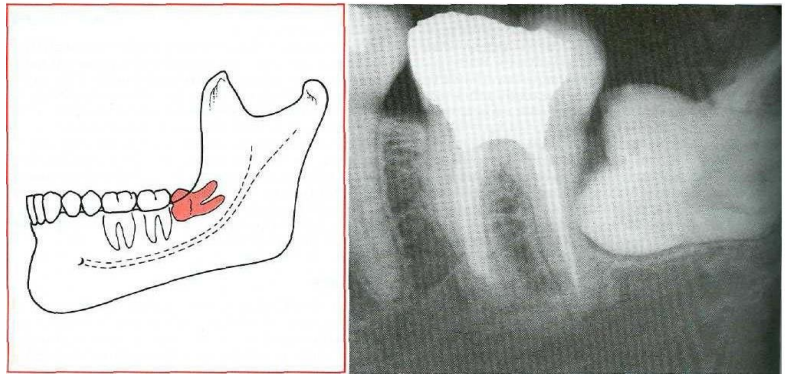
3- Horizontal 14
In a severe mesial inclination the impacted tooth is horizontal the longitudinal axis of the third molar tooth forming 90 degree angle with the longitudinal axis of the second molar tooth
Fig.3: horizontal impaction ' From Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry J. Peterson. Principles of management of impacted tooth p 194
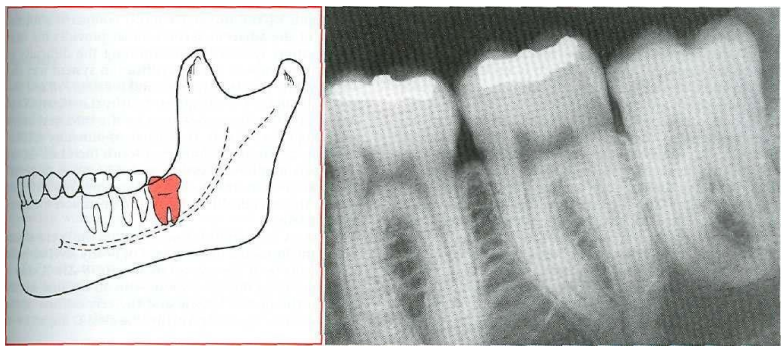
4-Vertical 14.
Vertical impaction the long axis of the impacted tooth runs in the same direction as the long axis of the second molar
Fig 4: Vertical impaction "Contemporary Oral and Maxillofacial Surgery, chapter 9.Larry J. Peterson. Principles of management of impacted tooth p 195.
Bell and Gregory's classification:
Class 1
The mandibular third molar teeth have sufficient anterioposterior room between the second molar and the ascending ramus.
Fig5: Class 1 position Contemporary Oral and Maxillofacial Surgery, chapter 9.Larry J. Peterson. Principles of management of impacted tooth p 196
2-Class 2:
Half of mandibular third molar tooth is approximately covered by anterior border of the ramus
Fig 6: Class 2 position "Contemporary Oral and Maxillofacial Surgery, chapter 9.Larry J. Peterson. Principles of management of impacted tooth p 196"
3-Class 3:
Where the mandibular third molar completely impeded in the ramus.
Fig 7: Class 3 Position: "Contemporary Oral and Maxillofacial Surgery, chapter 9.Larry J. Peterson Principles of management of impacted tooth p 196.
A further subdivision based on the level of the occlusal plane of the wisdom tooth relevant to the occlusal plane of the second mandibular molar
Position A :14
Impacted third molar tooth approximately in the same occlusal plane as the occlusal plane of the second molar tooth
Fig 8:- Position A. "Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry J Peterson Principles of management of impacted tooth p 196
5-position B: 14
Occlusal plane of the impacted third molar tooth is between the Occlusal plane of the second molar tooth and its cervical line.
Fig 9: Position B "Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry J. Peterson. Principles of management of impacted tooth p 197 '
6-position C: 14
Impacted third molar tooth below the cervical line of the second molar tooth
Fig 10: Position C "Contemporary Oral and Maxillofacial Surgery, chapter 9 Larry J Peterson Principles of management of impacted tooth p 197.
Bell and Gregory classification used by integration of its two parts, the relation of the third molar tooth to the anterior border of the ramus and its relation to cervical margin of the second molar tooth For example (class 3position A)
Sujata Byahatti, Mohammed S. H Ingafou 15 in Garyounis University studied a sample of 200 university students of Garyounis University. 100 males 100 females age 17-25 years with full complement of teeth They studied the number of wisdom teeth per person, angulation, level of eruption, available space for eruption, eruption status and presence or absence of lower wisdom teeth The most common type was Mesioangular impaction class A.
Ali A. Hassan10 in Saudi Arabia studied radiographs of 1039 Saudi patient and found Mesioangular class B impaction is the most common type .
In a cross-sectional study from Altaif Saudi Arabia by Sherifa Mustafa Sabra and Mahitab Mahmoud Soliman16 , studied prevalence of impaction of wisdom tooth, associated physical signs, medical complications and dominant microorganisms associated 113 orthopantograms of patients attending the clinic were examined and showed that Mesioangular was the commonest type, pain is the most common complain and streptococcus viridians was the commonest microorganism
Olasoji and Odusanya17 in Nigeria in a comparative study between rural and urban population regarding the food habit and its relation to wisdom tooth impaction of 2,400 subjects who were examined radiologically using orthopantographs They found that rural population has less tendency to wisdom tooth impaction compared to urban population. Most common type of impaction was mesioangular class A types This study supports the theory that suggests that muscular activity and degree of food hardness is major factor in wisdom tooth impaction. Nigeria A.E. Obiechina, J T. Arotiba, A.O. Fasola also studied the prevalence of wisdom tooth impaction. They examined 338 patients aged 16 and above with impacted mandibular third molars Method of analysis was preapical views and when necessary, oblique lateral radiographs of the mandibule were used The result showed that the most common type was mesioangular impaction19
Sunnel Kummar Punjabi, Noor Ahmed Khoso in Hyderabad University in Pakistan, studied the pattern, prevalence, symptoms and pathology associated with impacted wisdom tooth in a Descriptive prospective study of 290 patients aged 16-45 years with 500 impactions analyzed radiographically using orthopantographs, they found the vertical impaction to be the most common type
Arslan Wahid, Farrukh Imran Main in Pakistan assessed the prevalence and position of impacted third molar Orthopantographs of patients aged 18-50 years was studied. The result was that the most common type of impaction is the mesioangular type.
Mohammed Mehdizadeh, Sina Haghanifar21 in babol university, north Iran studied the presence of the impacted third molar teeth and their complications 2000 orthopantographs were examined by winter's classification and bell and Gregory classification. Results showed Mesioangular and type B depth are the commonest types and the frequency of impaction is higher in females (52 37%)
In a Malaysian study by Rosfaima Jaffar and Mon Mon Tin-Oo position of impacted mandibular third molar was examined Based on winter's and bell and Gregory classifications, 194 orthopantographs were examined. The results showed mesioangular and type Il Position A were the most common types of impaction
Sadeta Seeiae, Samir Prohiae studied the incidence of impaction of mandibular third molar in population of Bosnia and Herzegovina. 2000 orthopantographs studied and the vertical impaction was found the most common type 24
In a Brazilian study Marzola, Clovis, comparin Eliston investigated 585 orthopantographs and found that the vertical impaction and class Al impaction was the commonest types (62 66%, 16 65% respectively)
Justification:
It is important to establish base line information about Sudanese population wisdom teeth prevalence and classification Objectives:General:-
To evaluate the prevalence of mandibular wisdom tooth impaction among a sample of Sudanese population using OPTs
Specific:
1- To estimate the various types of impaction of mandibular wisdom teeth
2- To investigate the demography of mandibular wisdom teeth impaction, gender, and site.
Materials and Methods:
Study type: - This is a retrospective qualitative descriptive crosssectional study.
Materials: A total of 1720 Orthopantomographs
Study Sample & Study Duration: 1720 OPTs from 4 dental facilities in Khartoum city during the period march 2015 to June 2015
Sampling technique:
This is a total convenience coverage of all OPTs of patients who attended the minor surgery clinic in Khartoum dental teaching hospital and three private dental centers and clinics in Khartoum city. These centers are serving a general non defined population in governmental and private facilities KDHH: 390 OPTS, Dr Higzy Dental Clinic 453 OPTs, Amazin Dental Clinic: 620 OPTs, Ethetica
Dental Clinic: 257 OPTs Measurements
The angulation of the third molar tooth determined by Winter's classification. The angle measured was created by intersection of two vertical lines representing the longitudinal axis of third molar and second molar teeth
The depth of the wisdom tooth in relation to Occlusal plain of the second molar and the coverage of the ascending ramus of the mandible over the third molar tooth was determined by Bell and Gregory's classification The measurements were made using of VIX WIN PRO software version 1 5 a product of Gendex Company
2003
Inclusion criteria:
• Consecutive OPTs taken during the time of the study
• Complete root formation of mandibular wisdom teeth Excluding criteria:
•Jaw pathology or trauma.
•Congenital anomaly
•Incomplete root formation of wisdom teeth
•Previous extraction of wisdom tooth from the contralateral side of the mandible.
•Absence of second or first molar teeth
Data collection form:
Data was collected using a data collection form by the principle investigator Data was cleared and entered in an SPSS version 20 Data analysis: The data was analyzed using SPSS version 20 and presented in tables and figures.
Results
In this study there 938 Females (54.5%) and 782 Males (45.5%)
Out of the 1720 OPGS in this study there were 480 with mandibular tooth impactions (32%)
Impactions were more common among females (268) 55 8% than males (212) 44.2% as shown in Table I below.
There are a total of 480 impactions, the mesioangular impaction being the most frequent making a total of 141 impactions as a separate category, followed by the horizontal impaction
Being 120 impactions, 16 distoangular impactions, the least common being the vertical type. The mixed presentations being 83 impactions with almost equal distribution among the various types with exception of mixed presentations with the vertical type.
In some OPTs they are bilateral third molar impaction. In this case the number of impactions is counted as 2 impactions in one OPT other cases with unilateral third molar impaction counted as 1 impaction Females are more susceptible to impaction 55.8% than males 44.2%
Table 1 : Gender and side distribution of impactions among 480 patients:
|
No. of cases |
males |
|
|
females |
|
|
|
unilatera |
bilateral |
unilateral |
bilateral |
|||
|
480 |
176 |
57 |
44.20/o |
206 |
41 |
55.8 |
According to Winters classification, mesioangular impaction is the most common type as shown in table 2
Table 2:- type of impaction distribution according to Winters classification:
|
Type of impaction |
Total number |
percentage |
|
mesioangular |
141 |
29.4 |
|
horizontal |
120 |
25 |
|
distoangular |
14 |
3 |
|
vertical |
4 |
0.9 |
Table 3:- gender distribution among Winter classification:
|
Type of impaction |
|
|
female |
|
|
mesioangular |
66 |
13 |
75 |
165 |
|
horizontal |
59 |
123 |
61 |
127 |
|
distoangular |
5 |
1 |
9 |
1 9 |
|
vertical |
1 |
0.2 |
3 |
0.6 |
Table4:-shows side distribution of the each type of third molar according to Winter classification
|
Type of impaction |
unilateral |
percentag |
Bilateral |
percentag |
|
mesioangular |
61 |
12 7 |
80 |
16.6 |
|
distoangular |
6 |
1 2 |
8 |
1 6 |
|
horizontal |
26 |
|
3 |
0.6 |
|
vertical |
1 |
0 2 |
3 |
0.6 |
Table 5: Showing the gender distribution of the impactions according to bell and Gregory classification:
|
Type of impaction |
male |
% |
femal |
% |
|
Class I Position A |
|
|
|
|
|
Class I Position B |
1 |
0.2 |
0 |
0 |
|
Class I Position C |
|
|
|
0.2 |
|
Class Il Position A |
|
|
|
|
|
Class II Position B |
1 |
0.2 |
0 |
0 |
|
Class II Position C |
|
0.6 |
o |
o |
|
Class III Position A |
|
|
|
|
|
Class III Position B |
18 |
3.7 |
0 |
0 |
|
Class III |
16 |
3.3 |
0 |
0 |
Table 6:- shows side distribution of the each type of third molar impaction according to Bell and Gregory classification
|
Type of impaction |
unilateral |
|
bilateral |
|
|
Class I Position A |
0 |
0 |
0 |
|
|
Class I Position B |
o |
o |
1 |
0.2 |
|
Class I Position C |
1 |
0.2 |
0 |
|
|
Class II Position A |
0 |
0 |
0 |
|
|
Class Il Position B |
o |
o |
1 |
0.2 |
|
Class II Position C |
3 |
0.6 |
0 |
|
|
Class III Position A |
|
0.2 |
19 |
3.9 |
|
Class III Position B |
o |
o |
18 |
3.7 |
|
Class Ill Position C |
0 |
0 |
16 |
3.3 |
Table 7:- shows number of third molar impaction according to winter classification mixed with Bell and Gregory classification
|
Type of impaction |
mixed with other type |
|
No. as separate type |
|
|
Mesioangul ar |
31 |
64 |
141 |
29 4 |
|
Distoangula |
28 |
5 8 |
14 |
2 9 |
|
vertical |
|
5 |
4 |
0 8 |
|
horizontal |
|
o |
120 |
25 |
Table 8:- shows number of third molar impaction according to Bell and Gregory classification mixed with other type:
|
Type of impaction |
mixed with other type |
|
No. as separate type |
% |
|
Class I Position A |
o |
o |
o |
o |
|
Class I Position B |
2 |
0.4 |
1 |
0.2 |
|
Class I Position C |
16 |
3.3 |
|
0.2 |
|
Class Il Position A |
o |
o |
o |
o |
|
Class Il Position B |
3 |
0.6 |
1 |
0.2 |
|
Class Il Position C |
1 1 |
2.3 |
3 |
0.6 |
|
Class Ill Position A |
7 |
1.4 |
20 |
4.2 |
|
Class Ill Position B |
22 |
4.5 |
18 |
3.75 |
|
Class Ill Position C |
35 |
7.2 |
16 |
3.3 |
In cases of one side with third molar impaction and on the other side the third molar tooth was absent the pattern was less than cases with two sided third molar tooth 36% and 50% respectively In some cases Winter classification and Bell and Gregory' classifications are applicable in one case. This pattern represents 37% from the population with impaction Class 3 position C was the most common type in this Integrated Pattern with other types 72%
Discussion
Third molar tooth often develop in inappropriate location and therefore unable to erupt properly. In fact the most common impacted tooth was the third molar tooth as shown in many studies from developed countries
Genetic and ethnic background appeared to have an influence in third molar tooth impaction Sudan region has a unique ethnic diversity Negros, Caucasians, Arabs, has wide distribution in Sudan and over decades there is mating between these groups which resulted in a wide variety of physical characteristics. Also different nutritional habits which might affect the position and eruption of the third molar tooth.
The importance of such study in this field reflected from the fact that there are many problems associated with impaction of the third molar tooth The difficulty of the third molar tooth removal and in and postoperative complications can be assessed and reduced by knowing which type of impaction is being handled.
In this study of 1720 OPTs examined we found 480 cases with impaction representing 32% of the sample. The most common type was the mesioangular type of impaction which is nearly equivalent to study done by Hassan from Saudi Arabia 33.4% Our findings disagree with those from China which showed that horizontal type of impaction was the most common and similarly disagree with a report from Haiderabadl ! in which vertical impaction was the most common type.
Impactions in females are more common than males with 43% and 37% respectively. This result agrees with studies in the literature. From Saudi Arabia 10, Libya15 , Pakistan , all of these results demonstrated a tendency to an increase in female impactions compared to males.
According to Bells and Gregory classification we found class 3A was the most common type which disagrees with Altaif University findings from Saudi Arabia where class B type being the most common , however they studied the level of eruption of the third molar tooth as measured from the second molar tooth level and not from the ascending ramus. Our results agreed with results from Libya' 5 however they as well measured level of eruption based on the second molar level In Malaysia and Herzegovina they imployed the whole components of Bells and Gregory classification and found class 2A and class IA to be the most common in contradistinction to the findings of this study.
In some cases it was found that the two classifications, according to angulation and according to second molar and ascending ramus can be applied for example: I-Mesioangular, class3B
2-Vertical, class 3C
3-DistoanguIar, class3A
Generally all cases of vertical impaction can accept both Bell's and
Gregory's classification especially class 2and 3 levels B and C The most commonly represented mixed pattern was the mesioangular type with class3C 7 2%
Following and monitoring of impaction using this mixed pattern would probably give a better estimation for difficulty of third molar surgical removal and possibly predicts postoperative complications This because it gives full survey for the position of the tooth with regard to second molar, alveolar bone, and ascending ramus of the mandibule.

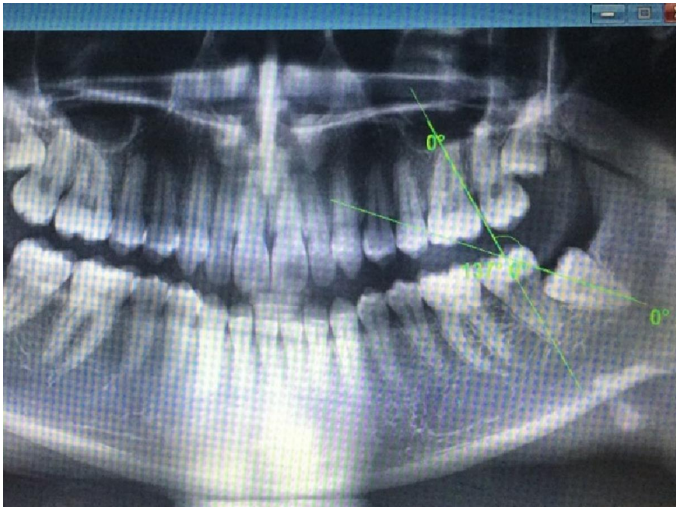
Figll Demonstrating in right side an integrated pattern of classification
(Distoangular impaction according to winter and class 3 position B according to Bell and Gregorys classification)
Impactions seen in fig. 11 are a good example of integrated pattern, reporting the type of impaction with this pattern give good estimation to the operator warn against complications like jaw bone fracture due to mass bone removal in all direction. This will help the operator to have preparedness for such mishaps and, warn the patient and get his consent for such an expected complication
Conclusions
1- This study showed that the mesioangular is the most common type of mandibular wisdom tooth impaction
2- Third molar tooth impaction is the most common in females 55.8% than males 44.2%
3- Integration of the two types of third molar tooth impaction classifications (Winters, Bell and Gregory) make the provisional surgical plan more clear and provide an idea about expected complications.
4- Limitations of this study are manifest because of using only radiographs and such results could not be generalized to population. a particular clinical situation
Recommendations:
I-We recommend a patient based study linking clinical and radiographic findings of impacted wisdom teeth in Sudanese population
2-lt is also recommended to conduct a survey involving a large sample in order to generalize any results.
Please click here to view complete article with figures