Cetuximab Based Chemotherapy in Recurrent and Metastatic SCC of Esophagus – A Real World Short Case Series from a Tertiary Cancer Care Center
Cetuximab Based Chemotherapy in Recurrent and Metastatic SCC of Esophagus – A Real World Short Case Series from a Tertiary Cancer Care Center
Dr Siddhesh Rajendra Tryambake ¹*, Dr S S Nirni ²
1) Resident Medical Oncology, Department of Medical Oncology, Omega Hospitals, Hyderabad, India.
2) Consultant and Head, Department of Medical Oncology, Omega Hospitals, Hyderabad, India.
*Correspondence to: Dr Siddhesh Rajendra Tryambake, Resident Medical Oncology, Department of Medical Oncology, Omega Hospitals, Hyderabad, India.
Copyright.
© 2025 Dr Siddhesh Rajendra Tryambake This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 February 2025
Published: 10 February 2025
DOI: https://doi.org/10.5281/zenodo.14903662
Abstract
Background: A significant fraction of esophageal cancers has an increased amount of the epidermal growth factor receptor (EGFR). Prior studies have examined tyrosine kinase inhibitors that target EGFR, but there is currently a lack of information regarding the effects of EGFR-directed monoclonal antibody therapy in these specific cancer types. A retrospective audit was carried out at a single institution, specifically targeting patients who were diagnosed with unresectable or metastatic esophageal squamous cell carcinoma and received cetuximab-based treatment. Patients and Methods: 15 patients who previously had treatment for recurrent or metastatic esophageal squamous cell carcinoma (SCC) were included in the study and retrospectively analyzed. These patients were treated with cetuximab, a monoclonal antibody, based therapy, on a weekly basis. The treatment started with an initial dose of 400 mg/m2, followed by weekly infusions at a dose of 250 mg/m2. Some patients had received cetuximab as a single agent while others received the same with concurrent chemotherapy. Patients were monitored for adverse effects, therapy efficacy, and overall survival.
Results: A total of 15 patients (median age of 67 years at the time of analysis) were evaluated. 8th edition AJCC staging system revealed 9 (60%) patients to be having metastatic disease, 5 33.33%) recurrent stage and 1 patient having unresectable disease. The Eastern Cooperative Oncology Group (ECOG) performance score (PS) was I in 4 (26.7%) and II in 11 (73.3%). Majority of patients were males (73.3%) with only 1 patient having multiple comorbidities and the rest having single or none. 5 patients (33.33%) received cetuximab as a single agent, 3 with methotrexate and nab-paclitaxel each, while 2 patients received cetuximab with paclitaxel and paclitaxel plus carboplatin combination each. 9 patients (60%) had received cetuximab or cetuximab based chemotherapy in 1st and 2nd line, while the rest received the same in 3rd and above lines. Median OS was 34 months and 2-year OS rate in the study was 80% while median PFS was 3 months and 6-month PFS rate was 7 % only. 1 patient had complete response; 5 patients (33.33%) had partial response; 9 patients (60%) had disease progression on initial assessment. overall response rate (ORR) as well as disease control rate (DCR) was 40 % at first follow-up as there were no patients with stable disease.
Conclusion: Although well tolerated, cetuximab administered as a single agent had minimal clinical activity in patients with metastatic esophageal SCC. Ongoing studies of EGFR inhibitors in combination with other agents may define a role for these agents in the treatment of esophageal.
Key words: cetuximab, chemotherapy, advanced esophageal cancer, squamous cell carcinoma
Cetuximab Based Chemotherapy in Recurrent and Metastatic SCC of Esophagus – A Real World Short Case Series from a Tertiary Cancer Care Center
Introduction
Esophageal cancer is associated with a bleak outlook, as around 80% of patients are diagnosed with advanced disease. The most often employed initial treatment for advanced esophageal squamous cell carcinoma (ESCC) is systemic chemotherapy with cisplatin and 5-fluorouracil (5- FU). Nevertheless, the percentage of responses to treatment is quite low, ranging from 15% to 45%, and the typical duration of survival is often less than 8 months, as indicated by many studies [1–3]. Thus, there is an urgent need for new and innovative treatments to enhance results in this particular context. EGFR is highly expressed in 50%–70% of ESCCs, as indicated by research [4– 6]. This high expression has been found to be associated with prognosis [5–7]. EGFR activation stimulates the RAS, ERK1/2, PI3K/Akt, and STAT pathways, which can lead to resistance to chemotherapy, angiogenesis, and increased tumor growth [8, 9]. Furthermore, preclinical findings shown that cetuximab not only increased the effectiveness of chemotherapy but also specifically boosted the impact of cisplatin [10, 11]. Thus, it was deduced that inhibiting EGFR could be a viable approach for treatment. Cetuximab, a monoclonal antibody of the immunoglobulin G1 class that selectively targets the EGFR, has demonstrated effectiveness in treating colorectal cancer [12], non-small-cell lung cancer (NSCLC) [13], recurrent/metastatic head and neck squamous cell carcinoma (HNSCC) [14–17], and locally advanced HNSCC [18]. Given the established effectiveness of cetuximab in treating HNSCC, a kind of cancer that shares similar tumor characteristics with ESCC and has high levels of EGFR expression, we theorized that cetuximab could also be effective in treating advanced ESCC. Consequently, we examined the efficacy and safety of cetuximab as a standalone treatment or when combined with conventional chemotherapy in patients with advanced ESCC.
Materials And Methods
Study Design
This is a retrospective audit conducted at a single center. The data obtained includes information on patients, diseases, and treatment characteristics.
Patients
This study is a retrospective audit conducted at a single center. The data collected includes information on patient demographics, disease features, and treatment details. The study comprised of 15 patients, aged 18 years or older, who were diagnosed with recurrent and advanced esophageal SCC. These patients were hospitalized to our hospital between January 2015 and January 2021. The inclusion criteria were patients who were at least 18 years old, had inoperable recurrent or advanced cancer, had an ECOG performance status of 0-2, and had no contraindications to treatment. The exclusion criteria were individuals who exhibited intolerance to chemotherapy due to severe cardiac, pulmonary, hepatic, or renal conditions, as well as those with concurrent malignancies.
Objectives
The study sought to evaluate the effectiveness of Cetuximab-based chemotherapy in individuals with recurrent and metastatic esophageal squamous cell carcinomas. The study assessed the effectiveness of the treatment by analyzing the overall survival (OS), progression-free survival (PFS), overall response rate (ORR), disease control rate (DCR), and the safety of the treatment in terms of both hematological and nonhematological toxicities.
Study Methods
Staging was performed for all the patients with confirmed histopathological diagnosis based on TNM classification of the Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC 8th Edition). All patients were administered either cetuximab alone or cetuximab based chemotherapy by the investigator in the given period of time. Cetuximab was first infused at 400 mg/m2 for 120 min and then at 250 mg/m2 per week for 60 min. Combined chemotherapy regimens included concurrent cisplatin, methotrexate, paclitaxel plus carboplatin or nab-paclitaxel. Informed consent was waived off in view of retrospective nature of the study.
Study Endpoints
In addition to the standard demographic information, the effectiveness of cetuximab-based chemotherapy was evaluated by measuring overall survival (OS), progression-free survival (PFS), overall response rate (ORR), and disease control rate (DCR) of the patients. PFS was defined as the time interval between the initiation of cetuximab treatment and either the occurrence of disease progression or death from any cause, or the last follow-up date, whichever came first. The OS was determined by calculating the time from the date of diagnosis to the date of death due to any cause. ORR was characterized by patients who achieved complete response (CR) or partial response (PR) during the initial evaluation. DCR was defined as the absence of disease progression and encompassed patients with CR, PR, and stable disease (SD). The retrospective evaluation of the patient's survival was conducted across the entire length of the trial. Furthermore, the evaluation of response was conducted by employing the institutional radiological evaluation protocol at intervals of 8 weeks. Alternatively, any symptoms or signs of clinical progression were considered according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.19. The data regarding CR, PR, SD, and progressive disease (PD) were analyzed. The administration of cetuximab-based chemotherapy was maintained until the occurrence of disease progression or the development of intolerable adverse effects. The safety assessment involved evaluating the occurrence of both hematological and nonhematological toxicities, using the Common Terminology Criteria for Adverse Events (CTCAE version 5.0).
Statistical Analysis
Data was descriptively analyzed using mean and standard deviation or median and interquartile range depending upon the normality of the data. Normality of the data was checked using the Shapiro–Wilk test while categorical variables were reported using frequency and percentage. ORR (CR + PR) and DCR (CR + PR + SD) were reported using frequency and percentage and their 95% Clopper–Pearson confidence interval (CI). Predictors of PFS, and OS were compared using Mantel–Haenszel log rank test and survival curves were generated using Kaplan–Meier method. The corresponding 6-month and 2-year survival rates were reported. Median follow-up was calculated using the reverse Kaplan–Meier method. Multivariate analysis was conducted using the cox proportional hazard regression. Proportional hazard assumption was tested using Schoenfeld’s residual and did not violate in this data set. Data was analyzed using IBM SPSS version 25.0 (IBM Corp., Armonk, New York, United States) and R Studio version 1.2.1335.
Results
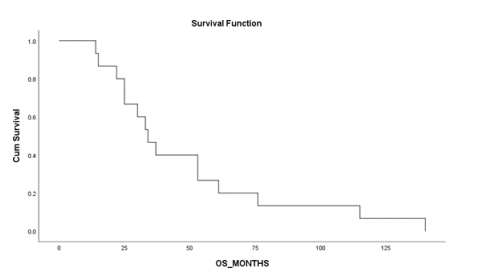
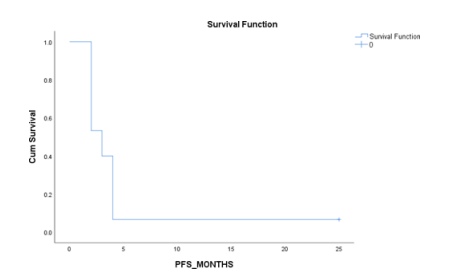
A total of 15 patients (median age of 67 years at the time of analysis) were evaluated. AJCC Staging system revealed 9 (60%) patients to be having metastatic disease, 5 (33.33%) recurrent stage and 1 patient having unresectable disease. The Eastern Cooperative Oncology Group (ECOG) performance score (PS) was 1 in 4 (26.7%) and 2 in 11 (73.3%). Majority of patients were males (73.3%) with only 1 patient having multiple comorbidities and the rest having single or none. 5 patients (33.33%) received cetuximab as a single agent, 3 with methotrexate and nab-paclitaxel each, while 2 patients received cetuximab with paclitaxel and paclitaxel plus carboplatin combination each. 9 patients (60%) had received cetuximab or cetuximab based chemotherapy in 1st and 2nd line, while the rest received the same in 3rd and above lines. Median OS was 34 months and 2-year OS rate in the study was 80% while median PFS was 3 months and 6-month PFS rate was 7 % only. 1 patient had complete response; 5 patients (33.33%) had partial response; 9 patients (60%) had disease progression on initial assessment. ORR as well as DCR was 40 % at first follow-up as there were no patients with stable disease. Kaplan Meier Survival Curves for OS and PFS are depicted in Fig 1 and Fig 2 respectively.
Figure 1 – KM curve for OS (Median OS was 34 months and 2-year OS rate in the study was 80%)
Figure 2 – KM curve showing PFS (Median PFS was 3 months and 6-month PFS rate was 7 %)
|
Gender Male Female |
11 05 |
|
Age (Median) |
67 years |
|
PS (ECOG) 1
2 |
04 11 |
|
Stage Recurrent Metastatic Unresectable |
05 09 01 |
|
Line of Treatment 1st and 2nd line 3rd and 4th line |
09 06 |
|
Concurrent Chemotherapy Paclitaxel plus carboplatin Methotrexate Nab-Paclitaxel Paclitaxel SA |
02 03 03 02 05 |
|
Comorbidities – Nil/Single Multiple |
14 01 |
Table – 1 – Patient characteristics
Toxicity Profile
No patients died of severe adverse reactions during treatment. All patients had different degrees of adverse reactions, mainly including bone marrow suppression, rash, gastrointestinal reactions, hepatic and renal function damage, and neurotoxicity, and most of them were grade I and improved after symptomatic treatment. The following adverse reactions were of grade II and above: rash (46.7%), diarrhea (26.7%), fatigue (33.3%), and 1 patient with febrile neutropenia.
Prognostic Factors
The effects of the gender, PS, stage, line of treatment and comorbidities was evaluated as far as clinical outcomes are concerned. Median OS was 61 months (15.9-106) in females, compared to 33 months (23.3-42.7) in males (p=0.08). Median OS was 25 months in patients with PS 1, compared to 34 months (26.4-41.5) in PS 2 (p=0.28). Median OS was 53 months (35.5-70.5) in patients with unresectable or recurrent disease, compared to 25 months (12.6-37.4) in metastatic stage (p=0.96). Median OS was 34 months (31-36.9) in patients with who have received cetuximab based chemotherapy in 1st or 2nd line, compared to 30 months (7.6-52.4) in patients receiving the same treatment in 3rd and above lines (p=0.96). Median OS was 34 months (26.7- 41.3) in patients with none or single comorbidity, compared to 14 months in patients with multiple comorbidities (p=0.00). Median PFS was 2 months in females, compared to 3 months in males (p=0.47). Median PFS was 2 months in patients with PS 1, compared to 3 months (3.5-4.5) in PS 2 (p=0.01). Median PFS was 4 months (3.4-4.5) in patients with recurrent disease, compared to 2 months in metastatic stage (p=0.01). Median PFS was 2 months in patients with who have received cetuximab or cetuximab based chemotherapy in 1st or 2nd line, compared to 3 months (1.8-4.2) in patients receiving the same treatment in 3rd and above lines (p=0.81). Median PFS was 3 months (1.2-4.8) in patients with none or single comorbidity, compared to 2 months in patients with multiple comorbidities (p=0.28). Baseline characteristics of this patient population are listed in Table 1.
Discussion
Considering that cisplatin in combination with 5-FU is the preferred treatment for patients with ESCC, our objective was to enhance effectiveness by incorporating cetuximab into this treatment regimen. The objective response rate (ORR) of 40% in the study group aligns with previously documented findings for the combination of cisplatin and 5-FU [1]. Thus, the outcomes have successfully achieved the main goal of showcasing a response rate of at least 40%. Nevertheless, assessing only the rates at which patients respond to treatment may fail to accurately measure the overall impact of targeted medicines. Prior research has demonstrated that inhibiting EGFR can lead to disease stability rather than tumor reduction [20]. A number of more recent chemotherapeutic drugs have demonstrated remarkable response rates of 40%–66% and survival rates ranging from 8 to 15 months in phase II trials [21–24]. However, it is important to acknowledge that a significant number of these trials were not conducted using randomization and involved diverse groups of patients. Furthermore, the bulk of these studies lack clarity regarding the consistent utilization of confirmed results in accordance with RECIST guidelines. Because the sample size is small, this study does not provide enough data to make strong statistical comparisons between the different groups in terms of PFS and OS. Therefore, no notable influence of gender on survival and PFS was detected. The effectiveness findings for the cetuximab-chemo group are promising. The incidence and categories of adverse events (AEs) observed in our patients were in line with what would be anticipated based on the specific medication used. Furthermore, there was no evidence indicating that cetuximab exacerbated the established harmful consequences of the chemotherapy. There were no recorded fatalities associated with cetuximab. Overall, considering the constraints of the trial design and the limited number of eligible patients, the results of this study suggest that the cetuximab alone or in combination treatment may be a valuable therapeutic strategy with modest clinical benefit in Indian set of patients and should be further explored. The inclusion of cetuximab into multimodal therapeutic techniques may eventually yield the greatest benefit.
Conclusion
Although well tolerated, this limited real-world data suggests that cetuximab administered as a single agent or in combination with chemotherapy had a modest clinical activity in Indian set of patients with advanced esophageal SCC. However, further studies are warranted for validation of the same.
Disclosure of Interest – None
References
1. Bleiberg H, Conroy T, Paillot B et al. Randomised phase II study of cisplatin and 5-fluorouracil (5-FU) versus cisplatin alone in advanced squamous cell oesophageal cancer. Eur J Cancer 1997; 33: 1216–1220.
2. Ilson DH, Kelsen DP. Management of esophageal cancer. Oncology (Williston Park) 1996; 10: 1385–1396, 1401–1402; discussion 1402–1408.
3. Polee MB, Kok TC, Siersema PD et al. Phase II study of the combination cisplatin, etoposide, 5- fluorouracil and folinic acid in patients with advanced squamous cell carcinoma of the esophagus. Anticancer Drugs 2001; 12: 513–517.
4. Hanawa M, Suzuki S, Dobashi Y et al. EGFR protein overexpression and gene amplification in squamous cell carcinomas of the esophagus. Int J Cancer 2006; 118: 1173–1180.
5. Gibault L, Metges JP, Conan-Charlet V et al. Diffuse EGFR staining is associated with reduced overall survival in locally advanced esophageal squamous cell cancer. Br J Cancer 2005; 93: 107– 115.
6. Wang KL, Wu TT, Choi IS et al. Expression of epidermal growth factor receptor in esophageal and esophagogastric junction adenocarcinomas: association with poor outcome. Cancer 2007; 109: 658–667.
7. Ozawa S, Ueda M, Ando N et al. Prognostic significance of epidermal growth factor receptor in esophageal squamous cell carcinomas. Cancer 1989; 63: 2169–2173.
8. Lemmon MA, Bu Z, Ladbury JE et al. Two EGF molecules contribute additively to stabilization of the EGFR dimer. EMBO J 1997; 16: 281–294.
9. Gibson AD, Lamerdin JA, Zhuang P et al. Orientation of heparin-binding sites in native vitronectin. Analyses of ligand binding to the primary glycosaminoglycan binding site indicate that putative secondary sites are not functional. J Biol Chem 1999; 274: 6432–6442.
10. Fan Z, Baselga J, Masui H, Mendelsohn J. Antitumor effect of anti-epidermal growth factor receptor monoclonal antibodies plus cis-diamminedichloroplatinum on well established A431 cell xenografts. Cancer Res 1993; 53: 4637–4642.
11. Baselga J, Norton L, Masui H et al. Antitumor effects of doxorubicin in combination with anti- epidermal growth factor receptor monoclonal antibodies. J Natl Cancer Inst 1993; 85: 1327– 1333.
12. Cunningham D, Humblet Y, Siena S et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med 2004; 351: 337– 345.
13. Butts CA, Bodkin D, Middleman EL et al. Randomized phase II study of gemcitabine plus cisplatin, with or without cetuximab, as first-line therapy for patients with advanced or metastatic non small-cell lung cancer. J Clin Oncol 2007; 25: 5777–5784.
14. Burtness B, Goldwasser MA, Flood W et al. Phase III randomized trial of cisplatin plus placebo compared with cisplatin plus cetuximab in metastatic/recurrent head and neck cancer: an Eastern Cooperative Oncology Group study. J Clin Oncol 2005; 23: 8646–8654.
15. Baselga J, Trigo JM, Bourhis J et al. Phase II multicenter study of the antiepidermal growth factor receptor monoclonal antibody cetuximab in combination with platinum-based chemotherapy in patients with platinum refractory metastatic and/or recurrent squamous cell carcinoma of the head and neck. J Clin Oncol 2005; 23: 5568–5577.
16. Herbst RS, Arquette M, Shin DM et al. Phase II multicenter study of the epidermal growth factor receptor antibody cetuximab and cisplatin for recurrent and refractory squamous cell carcinoma of the head and neck. J Clin Oncol 2005; 23: 5578–5587.
17. Vermorken JB, Trigo J, Hitt R et al. Open-label, uncontrolled, multicenter phase II
study to evaluate the efficacy and toxicity of cetuximab as a single agent in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck who failed to respond to platinum-based therapy. J Clin Oncol 2007; 25: 2171–2177.
18. Bonner JA, Harari PM, Giralt J et al. Radiotherapy plus cetuximab for squamous cell carcinoma of the head and neck. N Engl J Med 2006; 354: 567–578.
19. Brink M, de Goeij AF, Weijenberg MP et al. K-ras oncogene mutations in sporadic colorectal cancer in The Netherlands Cohort Study. Carcinogenesis 2003; 24: 703–710.
20. Xiong HQ, Rosenberg A, LoBuglio A et al. Cetuximab, a monoclonal antibody targeting the epidermal growth factor receptor, in combination with gemcitabine for advanced pancreatic cancer: a multicenter phase II trial. J Clin Oncol 2004; 22: 2610–2616.
21. Ilson DH, Saltz L, Enzinger P et al. Phase II trial of weekly irinotecan plus cisplatin in advanced esophageal cancer. J Clin Oncol 1999; 17: 3270–3275.
22. Ilson DH, Ajani J, Bhalla K et al. Phase II trial of paclitaxel, fluorouracil, and cisplatin in patients with advanced carcinoma of the esophagus. J Clin Oncol 1998; 16: 1826–1834.
23. Zhang X, Shen L, Li J et al. A phase II trial of paclitaxel and cisplatin in patients with advanced squamous-cell carcinoma of the esophagus. Am J Clin Oncol 2008; 31: 29–33.
24. Lee J, Im YH, Cho EY et al. A phase II study of capecitabine and cisplatin (XP) as first-line chemotherapy in patients with advanced esophageal squamous cell carcinoma. Cancer Chemother Pharmacol 2008; 62: 77–84.