Advances in Periodontal Plastic Surgery: The Past, Present and Future Perspectives
Advances in Periodontal Plastic Surgery: The Past, Present and Future Perspectives
Yasmine El Choufi, DDS 1*, Carole Chakar, DDS, MSc, PhD 1,2, Abdel Rahman Kassir, DDS, MSc 1
1) Department of Periodontology, Faculty of Dental Medicine, Saint Joseph University of Beirut, Beirut, Lebanon
2) Cranio-Facial Research Laboratory, Faculty of Dental Medicine, Saint Joseph University of Beirut, Beirut, Lebanon.
*Correspondence to: Yasmine El Choufi, Department of Periodontology, Faculty of Dental Medicine, Saint Joseph University of Beirut, Beirut, Lebanon.
Copyright.
© 2025 Yasmine El Choufi This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 Feb 2025
Published: 12 Feb 2025
DOI: https://doi.org/10.5281/zenodo.14880831
ABSTRACT
This review aims to explore the historical developments, current practices, and future perspectives in soft tissue procedures within periodontal surgery. Mucogingival surgery, introduced by Friedman in 1957, focused on addressing soft tissue deficiencies around teeth. Early techniques, such as the laterally positioned flap, free gingival grafts, and vestibular extension procedures aimed to increase the width of attached gingiva and manage gingival recessions. These methods served as the basis for what later became known as periodontal plastic surgery, a term introduced by Miller in 1993 to include treatments for both functional and aesthetic concerns. Recent advancements, such as coronally advanced flaps, subepithelial connective tissue grafts and tunneling techniques, have significantly improved treatment outcomes for gum recessions. However, challenges like discomfort at donor sites and limitations in complex cases remain. New approaches, including soft tissue substitutes and cell-based therapies, are being developed to overcome these issues and provide better results for patients. This review highlights the progress made in this field and the promising future of periodontal surgery.
Keywords: Cell and tissue based therapy, connective tissue, gingival recessions, graft, periodontal, soft tissue.
Advances in Periodontal Plastic Surgery: The Past, Present and Future Perspectives
Introduction
The consensus report of workgroup 3 of the 2017 World Workshop classifies and defines mucogingival conditions around the natural dentition in the aim of improving consistency in diagnosing and treating these conditions globally. (1) The “normal mucogingival condition” is defined by the absence of pathologies such as gingival recession (GR), gingivitis, or periodontitis within the spectrum of individual anatomical and morphological variations. Deviations from this norm exist even in the absence of apparent pathologies. This definition clarifies the consideration of mucogingival conditions and deformities, such as deficient keratinized tissues (KTs), reduced vestibular depth, and unusual frenum/muscle positioning. These conditions, while not inherently pathogenic, but still differ from conventional oral morphological parameters. (2)
The mucogingival condition with GR involves an apical shift of the gingival margin from its physiological position towards an apical direction at the cemento-enamel junction (CEJ) associated with clinical attachment loss (CAL). Whereas the mucogingival condition without GR can be described through the assessment of gingival phenotype such as gingival thickness and keratinized tissue width (KTW), observed across the entire dentition or specific sites. (1) Recent epidemiological studies have shown that more than 90 % of the population in the USA are affected by mid-buccal GR. (3) In fact, root exposure which is associated with GR lead to major consequences such as impaired esthetics, hypersensitivity, caries, and non-carious cervical lesions (NCCL). (1)
In 1985, Miller classified GR into four classes based on the position of the tooth and its relationship with the periodontium. (4) The most widely used classification, proposed by Cairo et al in 2011, is based on the interdental CAL and is divided into 3 types (RT1, RT2 and RT3). (5) However, the 2017 World Workshop presents a scientific approach for categorizing gingival phenotype, GR, and associated cervical lesions. This classification system is oriented towards treatment planning but has not been widely adopted in practice.(1)
Defined by the American Academy of Periodontology in 2001, mucogingival therapy includes various periodontal treatments that involve surgical procedures to correct defects in the morphology, position, and amount of soft tissue and underlying bone support around teeth and implants. Originally termed “mucogingival surgery” by Friedman in 1957, it describes procedures aiming on preserving gingiva, removing aberrant attachments, and deepening the vestibule. Over time, the term evolved to include a broader range of surgical techniques involving both gingiva and alveolar mucosa. In 1993, Miller introduced the term “periodontal plastic surgery” to reflect the expanded scope, including correction of alveolar ridge deformities and soft tissue esthetics. The American Academy of Periodontology defined it as procedures addressing defects in the gingiva, alveolar mucosa, or bone. In 2014, the 10th European Workshop in Periodontology redefined these procedures as interventions modifying the position of the gingival margin and characteristics of marginal soft tissues. Today, the field has advanced with the introduction of soft tissue engineering, incorporating cell therapy approaches to further enhance periodontal treatment with great promise for the future.(6)
Considering the constant and rapid advancement in periodontal plastic surgery, the aim of this paper is to review and outline the historical foundations that underlie the current concepts and future perspectives in the field of soft tissue procedures.
1. Mucogingival surgery
Defined by Friedman in 1957, the term “mucogingival surgery” refers to surgical interventions that address problems related to the interaction between the gingiva and the alveolar mucosa, with the goal of establishing a functional and sufficient zone of attached gingiva.(7) Different interventions will be systematically elucidated in a chronological sequence facilitating the understanding of the progression.
1.1 Laterally positioned flap
The laterally positioned flap (LPF) introduced in 1956 by Grupe and Warren involved using the adjacent KT to create a pedicle flap shifted horizontally or laterally to cover exposed roots diagnosed with GR. (8)
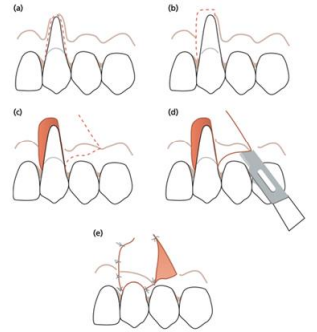
The flap design requires making two vertical oblique incisions starting from the base of the papillae of the tooth adjacent to the recession, extending deep into the alveolar mucosa allowing the pedicle flap to be raised full thickness and then shifted laterally. Excluding marginal soft tissue to minimize donor tooth recession risk as recommended by Grupe (Figure 1). (6)
Figure 1 : (a-e) LPF flap design : The surgical approach involving rotational pedicle grafts to address localized recession defects. (6)
Numerous variations to the original technique were described, excluding marginal soft tissue to minimize donor tooth recession risk was recommended in 1966 by Grupe. Following this, Staffileno (1964), Pfeifer and Heller (1971) advocated for a split-thickness flap to minimize dehiscence at the donor tooth. Using an edentulous area as a donor was proposed by Corn and Robinson (1964). Additionally, Björn (1971) contributed by incorporating a free gingival graft before laterally sliding the flap, enhancing treatment outcomes.
Regardless of the modifications, within the limitations of this flap it is impractical for treating multiple recessions and it presents challenges in enhancing the depth of the vestibule.(8)
A mean root coverage (MRC) of 76.78% was reported using the laterally positioned flap in mucogingival surgeries. (9)
1.2 Gingival augmentation procedure
In the 1960s, vestibular extension procedures aimed on preserving gingival health and preventing CAL by increasing the width of the attached gingiva. Gingival augmentation procedures embrace two main techniques: the denudation technique and the split flap procedure.
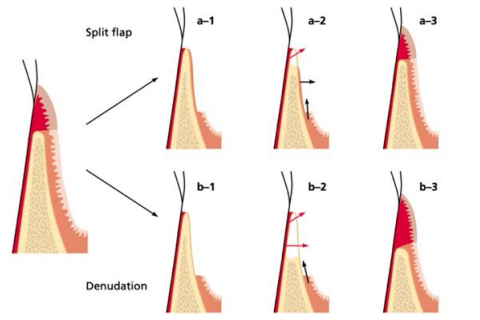
The denudation technique, described by Ochensbein in 1960, suggests a complete elimination of all the soft tissues while keeping the bone exposed. As a result, an increase in the gingival height was observed however the bone exposure led to severe and uncontrolled resorption.
As for the split flap procedure, described by Staffileno et al in 1962, only the superficial soft tissue was removed, and the bone was left covered by the periosteum. The results were similar to the denudation technique, but less resorption was observed (Figure 2). (6)
Figure 2 : Gingival augmentation procedure : (a1-a3) split flap technique, (b1-b3) denudation technique. (6)
1.3Free gingival grafts
Epithelialized free soft tissue graft was firstly introduced by Sullivan and Atkins in 1968. The procedure is a one-step technique where the recipient bed is de-epithelized, extended several millimeters laterally to the recession and the graft is placed at the CEJ after a root planning of the denuded surface. As for the healing, after 2 weeks the persistence of the graft over the exposed root is observed, defined as bridging. After several months a post-operative coronal migration of the free gingival margin was noticed, which is the creeping attachment phenomenon. In fact, a better prognosis is expected when the initial recession is shallow and narrow. (10)
A retrospective study describes the long-term outcomes, spanning 10 to 25 years of free gingival graft procedures performed using the Sullivan and Atkins technique on sites lacking attached gingiva associated with recessions. The results outlined the effectivity of this procedure to increase the amount of KT and to reduce GR over time.(11)
In 1975 Bernimoulin introduced the “two-step procedure”, where the graft is placed 2 mm apical to the recession and 2 months following the first surgery, the keratinized tissue gained are coronally advanced to cover the recession.(12)
Miller in 1982 proposed a one-step procedure where the graft is placed coronal to the CEJ on the prepared recipient bed. The sutures must be anchored in the periosteum and a gingivoplasty is performed after healing for esthetic purposes. This technique incorporates several key steps: starting with scaling and root planning of the exposed root surface then preparing a recipient connective tissue bed apical and lateral to the recession defect, with a width of 3–4 mm. The graft is placed on the prepared site and sutures are maintained for two weeks. After 3 months of healing a gingivoplasty is performed, if required, to improve the esthetic appearance.(6)
1.4 Double flap procedure
This approach consists of making a beveled internal incision on one side and an external beveling on the other. A process outlined by Cohen and Ross (1968). Two oblique incisions are made 1–2 mm coronal to the CEJ. The papillae are detached using a split-thickness incision technique. Subsequently, the two flap sections are aligned and sutured using a single interrupted suture across the midline, ensuring an accurate tissue edge overlap. The flap is further secured using a suspended suture technique to stabilize the wound and promote optimal healing. However, the anchorage area is small, the sutures are over an avascular area and tension is present on root convexities leading to some inherent limitations of the procedure. (6)
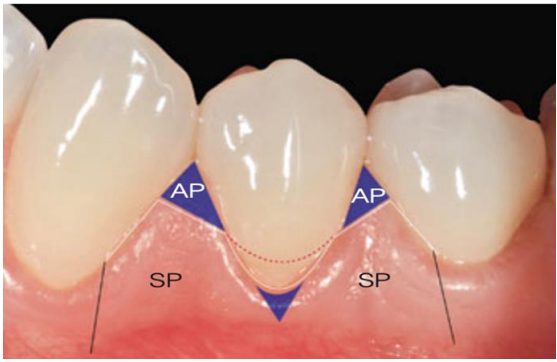
A modified double papillae flap is introduced by Acunzo in 2015, it involves making oblique incisions mesial and distal to the GR, followed by intrasulcular incisions. The flap is then raised using a split-full-split technique. Soft tissues are de-epithelialized, and the root surfaces are planned and scaled. The flaps are sutured with single interrupted and sling sutures for precise adaptation (Figure 3). A mean root coverage of 88.4% and a complete root coverage of 75 % is reported. (13)
Other modifications of the double flap procedure include the adjunction of a connective tissue graft (CTG) to increase root coverage outcome, however current studies lack long term follow-ups and are based on case series. (14)
Figure 3: Modified double papillae flap: oblique incisions define surgical papillae (SP) and preserve anatomical papillae (AP), ensuring precise recession coverage and gingival contour.(13)
1.5 Envelope technique
In 1985, Langer & Langer described the subepithelial connective tissue graft (SCTG) as a donor source for root coverage with a great advantage of avoiding the “keloid” healing that is seen with free gingival grafts. (15)- (16)
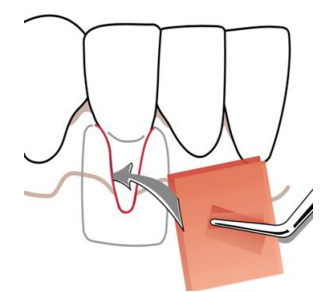
Subsequently, Raetzke developed the "envelope technique" in 1985, which involved employing SCTG to address localized root exposure. It involves creating a "pouch" in the surrounding tissue to hold the SCTG (Figure 4). However, part of the graft remained exposed which had a direct effect on the healing aspect, thus influencing the aesthetic part of the grafted area.
Petsos et al. (2019) evaluated the long-term outcomes of this technique, the study resulted in a MRC of 71.2% and 40% complete root coverage after 10 years. Recession depth decreased from 1.19 mm to 0.63 mm over this period. (17)
Figure 4 : Envelope technique. (6)
1.6 Semilunar coronally positioned flap
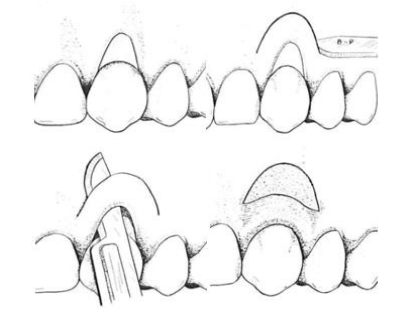
The semilunar flap, as described by Tarnow, involves a semilunar incision made parallel to the gingival margin, positioned at least 3 mm away from the gingival margin into the KT. The flap is elevated with a split thickness manner starting with an intrasulcular incision and extending to the neighboring papillae. This allows the flap to be moved coronally over the exposed root surface.
This flap is stabilized with light manual pressure, eliminating the need for sutures. The semilunar flap technique is advantageous because it requires no sutures, avoids tension on the flap, does not shorten the vestibule, and preserves the existing papillae. Its application is limited to treating shallow recessions that have a wide band of thick marginal KT (Figure 5).(18)
Figure 5: Semilunar coronally positioned flap design : the surgical method to treat shallow, localized recession defects.
1.7 Coronally advanced flap
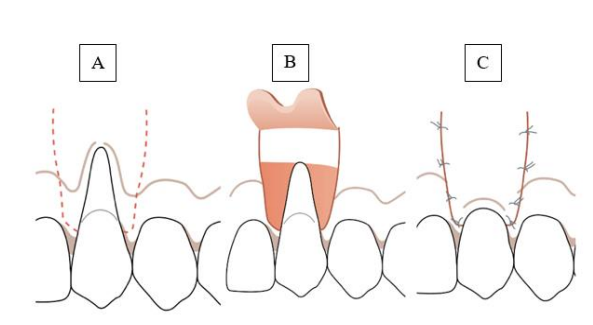
The coronally advanced flap (CAF) was initially introduced by Allen and Miller in 1989. A horizontal intrasulcular incision connects two vertical incisions, which diverge laterally from the tooth at the CEJ and extend into the alveolar mucosa. A split-thickness incision is then made to elevate the flap from the periosteum, allowing it to be positioned coronally over the CEJ. (19)
In 1992, Pini Prato and colleagues modified this approach by incorporating a horizontal marginal incision shaped like a “golf club” to enhance the dimensions of the surgical papillae. Following this, deeper divergent incisions are made into the alveolar mucosa. The purpose of these changes was to increase the flap's size, which would enhance its vascularization and general stability following surgery (Figure 6). (6)
Figure 6 : CAF. (A) Horizontal intrasulcular incision with two vertical incisions diverging at the CEJ, (B) full-thickness flap elevation and split-thickness incision, (C) coronal flap advancement and suturing.(6)
2. Periodontal plastic surgery
The term “Periodontal plastic surgery” was introduced by Miller in 1993 and focuses on the precise correction of alveolar ridge deformities and soft tissue aesthetics. This field has evolved from mucogingival surgery to include regenerative and reconstructive procedures aimed at restoring both function and esthetics. Emphasizing minimally invasive techniques, periodontal plastic surgery makes use of a better understanding of biological principles to improve patient outcomes. This paper reviews the current techniques and relevant literature in periodontal plastic surgery. (20)
2.1 Bilaminar technique
The bilaminar technique consists of using a pedicle flap to cover the graft. It enhances root coverage predictability by providing additional blood supply, while also improving the aesthetic result because it conceals the white scar color of the graft and masks the irregular outline of the mucogingival junction that frequently results after a free gingival graft procedure. (6)
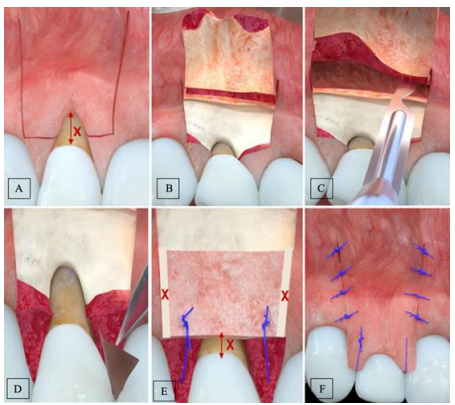
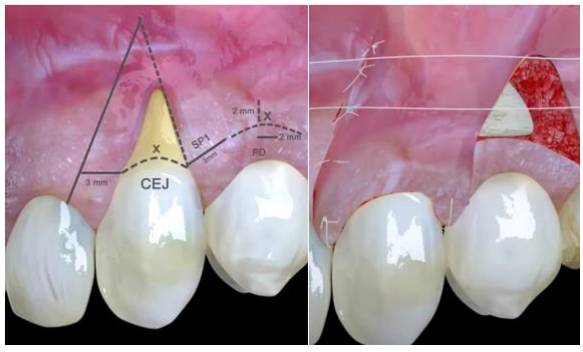
This procedure was introduced in 2003 by Zucchelli where the CTG is positioned slightly apical to the CEJ, thus avoiding any interference with the positioning of the marginal portion of the flap (the latter is positioned coronally to the CEJ). It involves two horizontal incisions (3 mm mesiodistally) at a distance from the anatomical papilla equal to the recession depth and two beveled vertical-releasing incisions extending into the alveolar mucosa. A split-thickness flap is elevated, and muscle insertions are removed for easier coronal displacement. Root surfaces with CAL are thoroughly treated and planned to achieve a clean, smooth surface. The graft dimensions exceed the recession width at the CEJ, with the apicocoronal dimension equal to the bone dehiscence depth, minus the pre-existing KT. Positioned apical to the CEJ, the graft is placed at a distance (x) equal to the height of KT, ensuring coverage. Sutures anchor the graft and stabilize it and sling sutures are used to coronally advance the flap and fully cover the CTG, forming the new gingival margin. This approach requires the presence of at least 1 mm of initial KT (Figure 7). (21)
Figure 7: Bilaminar technique. (A) Two horizontal incisions at a distance equal to recession depth (x) from the anatomical papilla, with two beveled vertical releasing incisions extending into the alveolar mucosa. (B) Full-thickness flap elevation. (C) Split-thickness flap elevation and muscle insertions removal for easier coronal displacement. (D) Papilla de-epithelialization. (E) graft stabilization. (F) flap suture.(34)
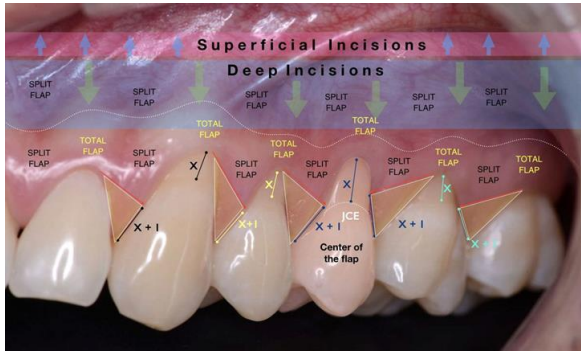
For the treatment of multiple recessions, a horizontal incision is made to create an envelope flap, extending one tooth on each side, choosing one tooth as a center of rotation for an effective coronal repositioning. Oblique submarginal incisions are placed interdentally to avoid loss of interdental KT. These incisions alter the positioning of the surgical papilla: those mesial to the flap’s midline rotate in a mesial-coronal direction, while those distal rotate in a distal-coronal direction (Figure 8). The flap is raised using a split-full-split approach to allow mobility. When the flap is advanced coronally, the papilla rotate toward the flap's edges, with the final position centered interproximally. (22)
Figure 8 : Bilaminar technique for multiple recessions. (34)
The bilaminar technique has shown 97.8 % of MRC for isolated RT1 and 97 % of MRC for multiple recessions.(23) In a 2009, Zucchelli et al. compared two CAF techniques: one with vertical releasing incisions and one without. Both approaches significantly reduced GR depth, achieving high patient satisfaction with aesthetic outcomes. However, the envelope-type CAF (without vertical incisions) led to a more substantial increase in the height of buccal KT, indicating a potential advantage for tissue stability and “keratinization”. (24)
2.2 Laterally moved coronally advanced flap
In 2004, Zucchelli et al. introduced the Laterally Moved Coronally Advanced Flap (LMCAF) technique as an improved procedure to the LPF. A triangular recipient area is de-epithelialized and prepared using three distinct incisions: a 3mm horizontal incision at the CEJ, a vertical beveled incision in the alveolar mucosa, and an intrasulcular incision along the recession's margin. The flap, which includes SP1 and SP2 (surgical papillae), is crafted to preserve at least 1mm of KT around the donor site. After lateral movement, the flap is anchored in place, ensuring it covers the recession area while maintaining stability (Figure 9). (25) MRC achieved in LMCAF was reported to be around 96%. (9)
Figure 9: LMCAF: a triangular flap is prepared with three incisions, preserving ≥1mm keratinized tissue, laterally moved, and secured to cover the recession. (34)
A study comparing the LMCAF and the bilaminar technique for treating single GR on molars found that both techniques were effective in recession coverage at first molar sites. However, the bilaminar technique was significantly related to higher rates of complete root coverage (CRC), while LMCAF was associated with a more comfortable post-operative experience. (26)
2.3 Tunnel
The tunneling (TUN) technique is a surgical approach deriving from the envelope technique. In 1994, Allen et al. expanded this approach to treat multiple recessions by creating a muco-gingival tunnel using a supra-periosteal flap with intrasulcular incisions, keeping papillae intact. The SCTG is then placed in the tunnel, partially covering the recessions, and secured. However, graft exposure sometimes led to necrosis and/or altered aesthetics, which was a limitation of this method.(6)
In 2010, Aroca et al. developed this technique to prevent graft exposure by coronally advancing the supra-periosteal flap, carefully detaching the interdental papillae and modifying the suturing technique (Figure 10). (27)
Figure 10: Tunnel : muco-gingival tunnel keeping papillae intact, CTG is placed in the tunnel and the flap is advanced coronally. (34)
Please click here to view all figures
The TUN technique preserves papilla height for better aesthetics and promotes healing with improved blood flow due to the lack of vertical incisions and the coronal flap position. It achieves both aesthetic and root coverage goals but requires advanced skills from the practitioner. A systematic review and meta-analysis evaluated the effectiveness of the TUN technique for treating localized and multiple GR, comparing it to the CAF. The findings indicated that TUN achieved a MRC of 82.75% for localized and 87.87% for multiple recessions, with better results observed in maxillary and Miller Class I/II defects. However, CAF was associated with a higher percentage of CRC when the same grafts (connective tissue or acellular dermal matrix) were used.(28) Another multi-center clinical paper revealed no significant difference in root coverage between the two techniques. However, TUN was associated with greater KT gain, shorter surgery time, and reduced postoperative discomfort, stating the procedure as a “less invasive alternative”. (29)
2.4 Free soft tissue
In 2013, De Santis and Zuchelli developed a free gingival graft concept using a two-step surgical procedure. First, the recipient bed is prepared at the base of the recession with the graft designed to match the height of the KT on adjacent teeth and the width to cover the recession and interdental papillae. This first procedure will increase the keratinized tissue apical to the recession and liberate the coronal muscle and fiber insertion. After three months, a second surgery is performed where a CAF is executed to cover the recession with the newly keratinized tissue gained. This technique is particularly beneficial for lower anterior cases where the recession extends to the base of the vestibule, or for cases with a shallow vestibule and insufficient KT for a LMCAF. (6) The findings indicate a MRC of 94 %. (9)
2.5 Soft tissue substitutes
Soft tissue substitutes have been explored as alternatives to autologous grafts for treating GRs. Highlighting the most documented: (1) acellular dermal matrix (ADM), used with CAF or the TUN technique, showed short-term MRC of 71% and long-term MRC of 68%. (2) Xenogeneic porcine-derived collagen matrix demonstrated 88% MRC at 12 months and 77% at 5 years. While porcine-derived acellular dermal matrix (PADM) yielded inferior results as compared to SCTG when using the CAF technique.(6)
In 2018 a systematic review reported that CAF, with or without CTGs or biomaterials, is effective for treating single or multiple GRs. Modified CAF and TUN techniques produced the highest CRC percentages, while evidence for soft tissue substitutes, like ADM grafts, was weak. The review called for RCTs to better understand the factors affecting prognosis.(23) A more recent systematic review and network meta-analysis (in 2022) concluded that SCTG combined with CAF remains the gold standard for treating single GR defects, offering the best outcomes in MRC, CRC, and KTW.(30)
3. Future perspectives
The aforementioned surgical techniques are effective for covering GR but are associated with some inherent drawbacks like increased morbidity, potential donor-site complications and some limitations in treating multiple advanced recessions. This has led to recent and growing interest in safer substitutes, including tissue engineering and cell therapy, which aims at generating tissues using cells, growth factors, and specific scaffolds. This method supports the regeneration, substitution and restoration of lost tissues, applying engineering principles for controlled soft and hard tissue regeneration.(31) So far, human gingival fibroblasts and autologous blood products are the main area of interest in relation to periodontal plastic surgery.
3.1 Gingival fibroblasts
Human gingival fibroblasts (hGFs) are considered the most suitable cell source for gingival tissue regeneration due to easy harvesting and strong healing capacity. Effective 3D scaffolds mimic the extracellular matrix (ECM) and support cell growth. Fibrin gel, a biocompatible, naturally derived scaffold with a soft tissue-like structure, is widely used as it enables nutrient transport and waste removal. When sourced from the patient’s blood, fibrin gel offers a biocompatible 3D scaffold with minimal inflammatory response. Autologous fibroblast culture on a collagen matrix with CAF is effective for GR, promoting healing, reducing surgery time, and lowering patient morbidity. However more studies are needed to evaluate the mean root coverage as well as the long term outcome.(32)
3.2 Autologous blood products (ABPs)
Autologous blood products (ABPs), derived from a patient's own blood through centrifugation, provide biomaterials rich in growth factors and cytokines essential for wound healing. ABPs include first-generation platelet-rich plasma and second-generation leukocyte and platelet-rich fibrin (L-PRF), which act as biological scaffolds for stabilizing and gradually releasing healing agents like platelet-derived growth factor and vascular endothelial growth factor. While ABPs can enhance root coverage and improve soft tissue characteristics, techniques like CAF combined with SCTG, ADM, or xenograft collagen matrix generally yield, till date, more predictable results than CAF with ABPs alone. There is still lacking evidence on the use of ABPs with mucogingival surgeries and controversies exist on whether the adjunction of ABPs results into a better surgical outcome. (33)
Conclusion
Over the past 30 years, significant advancements have reshaped the field of periodontal surgery, and the future holds even greater promise. Mucogingival surgery laid the foundation, periodontal plastic surgery now offers effective treatment, and cell therapy is an evolving concept with an immense and interesting potential. As we look ahead, continued innovation in these areas promises to enhance patient outcomes, offering hope for a more effective, easier and reproductible regenerative therapies in the years to come.
References
1. Jepsen S, Caton JG, Albandar JM, Bissada NF, Bouchard P, Cortellini P, et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018 Jun;45 Suppl 20:S219–29.
2. Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J Clin Periodontol. 2018 Jun;45 Suppl 20:S190–8.
3. Romandini M, Soldini MC, Montero E, Sanz M. Epidemiology of mid-buccal gingival recessions in NHANES according to the 2018 World Workshop Classification System. J Clin Periodontol. 2020 Oct;47(10):1180–90.
4. Miller PD. A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985;5(2):8–13.
5. Cairo F, Nieri M, Cincinelli S, Mervelt J, Pagliaro U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol. 2011 Jul;38(7):661–6.
6. Berglundh T, Giannobile WV, Lang NP, Sanz M, editors. Lindhe’s clinical periodontology and implant dentistry. Seventh edition. Hoboken: John Wiley & Sons, Inc; 2022.
7. FRIEDMAN N, LEVINE HL. Mucogingival Surgery. Dent Clin North Am. 1964 Mar 1;8(1):63–77.
8. Prato GP. Advances in mucogingival surgery. J Int Acad Periodontol. 2000 Jan;2(1):24–7.
9. Amine K, El Kholti W, Kissa J. Surgical Procedures. In: Periodontal Root Coverage [Internet]. Cham: Springer International Publishing; 2019 [cited 2024 Nov 9]. p. 47–72. Available from: http://link.springer.com/10.1007/978-3-030-20091-6_8
10. Matter J. Free gingival grafts for the treatment of gingival recession. A review of some techniques. J Clin Periodontol. 1982 Mar;9(2):103–14.
11. Agudio G, Nieri M, Rotundo R, Cortellini P, Pini Prato G. Free Gingival Grafts to Increase Keratinized Tissue: A Retrospective Long?Term Evaluation (10 to 25 years) of Outcomes. J Periodontol. 2008 Apr;79(4):587–94.
12. Bernimoulin J ?P., Lüscher B, Mühlemann HR. Coronally repositioned periodontal flap.: Clinical evaluation after one year. J Clin Periodontol. 1975 Mar;2(1):1–13.
13. Acunzo R, Pagni G, Fessi S, Rasperini G. Modified double papillae flap technique: a new surgical approach for the treatment of isolated gingival recession defects. A case series. Int J Esthet Dent. 2015;10(2):258–68.
14. Amine K, El Kholti W, Kissa J. Periodontal root coverage: an evidence-based guide to prognosis and treatment. Cham: Springer; 2019.
15. Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol. 1985 Dec;56(12):715–20.
16. Bruno JF. Connective tissue graft technique assuring wide root coverage. Int J Periodontics Restorative Dent. 1994 Apr;14(2):126–37.
17. Petsos H, Eickholz P, Raetzke P, Nickles K, Dannewitz B, Hansmeier U. Clinical and patient?centred long?term results of root coverage using the envelope technique in a private practice setting: 10?year results—A case series. J Clin Periodontol. 2020 Mar;47(3):372–81.
18. Tarnow DP. Semilunar coronally repositioned flap. J Clin Periodontol. 1986 Mar;13(3):182–5.
19. Allen EP, Miller PD. Coronal positioning of existing gingiva: short term results in the treatment of shallow marginal tissue recession. J Periodontol. 1989 Jun;60(6):316–9.
20. Miller PD. Periodontal plastic surgery. Curr Opin Periodontol. 1993;136–43.
21. Zucchelli G, Amore C, Sforza NM, Montebugnoli L, De Sanctis M. Bilaminar techniques for the treatment of recession?type defects. A comparative clinical study. J Clin Periodontol. 2003 Oct;30(10):862–70.
22. Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol. 2000 Sep;71(9):1506–14.
23. Chambrone L, Salinas Ortega MA, Sukekava F, Rotundo R, Kalemaj Z, Buti J, et al. Root coverage procedures for treating localised and multiple recession-type defects. Cochrane Oral Health Group, editor. Cochrane Database Syst Rev [Internet]. 2018 Oct 2 [cited 2024 Nov 9];2018(10). Available from: http://doi.wiley.com/10.1002/14651858.CD007161.pub3
24. Zucchelli G, Mele M, Mazzotti C, Marzadori M, Montebugnoli L, De Sanctis M. Coronally advanced flap with and without vertical releasing incisions for the treatment of multiple gingival recessions: a comparative controlled randomized clinical trial. J Periodontol. 2009 Jul;80(7):1083–94.
25. Zucchelli G, Cesari C, Amore C, Montebugnoli L, De Sanctis M. Laterally moved, coronally advanced flap: a modified surgical approach for isolated recession-type defects. J Periodontol. 2004 Dec;75(12):1734–41.
26. Zucchelli G, Marzadori M, Mele M, Stefanini M, Montebugnoli L. Root coverage in molar teeth: a comparative controlled randomized clinical trial. J Clin Periodontol. 2012 Nov;39(11):1082–8.
27. Aroca S, Keglevich T, Nikolidakis D, Gera I, Nagy K, Azzi R, et al. Treatment of class III multiple gingival recessions: a randomized-clinical trial. J Clin Periodontol. 2010 Jan;37(1):88–97.
28. Tavelli L, Barootchi S, Nguyen TVN, Tattan M, Ravidà A, Wang HL. Efficacy of tunnel technique in the treatment of localized and multiple gingival recessions: A systematic review and meta-analysis. J Periodontol. 2018 Sep;89(9):1075–90.
29. González-Febles J, Romandini M, Laciar-Oudshoorn F, Noguerol F, Marruganti C, Bujaldón-Daza A, et al. Tunnel vs. coronally advanced flap in combination with a connective tissue graft for the treatment of multiple gingival recessions: a multi-center randomized clinical trial. Clin Oral Investig. 2023 Jul;27(7):3627–38.
30. Chambrone L, Botelho J, Machado V, Mascarenhas P, Mendes JJ, Avila-Ortiz G. Does the subepithelial connective tissue graft in conjunction with a coronally advanced flap remain as the gold standard therapy for the treatment of single gingival recession defects? A systematic review and network meta-analysis. J Periodontol. 2022 Sep;93(9):1336–52.
31. Milinkovic I, Aleksic Z, Jankovic S, Popovic O, Bajic M, Cakic S, et al. Clinical application of autologous fibroblast cell culture in gingival recession treatment. J Periodontal Res. 2015 Jun;50(3):363–70.
32. Meenakshi RP, Kiruba R, Arun KV, Sivaram G, Arumuganainar D, Kaveri K. Cell-based therapy in the management of Class III Miller’s recession - A case report with 45-month follow-up. J Indian Soc Periodontol. 2023;27(4):437–42.
33. Geisinger ML, Kaur M, Abou Arraj RV, Basma H, Geurs NC. Clinical applications of mucogingival therapies utilizing adjunctive autologous blood products. Clin Adv Periodontics. 2022 Dec;12(4):233–40.
34. PerioPixels - Educational Surgery Videos [Internet]. YouTube; [cited 2025]. Available from: https://www.youtube.com/@PerioPixels.