A Rare Complication of Targetted Therapy: Pazopanib-Induced Intestinal Lymphangiectasia
A Rare Complication of Targetted Therapy: Pazopanib-Induced Intestinal Lymphangiectasia
Haran Nilesh N *1, Juvekar Shashikant L 2
1. Consultant, Department of Radiology, National Cancer Institute, Nagpur, Maharashtra, India.
2. Head of Department, Department of Radiology, National Cancer Institute, Nagpur, Maharashtra, India.
*Correspondence to: Haran Nilesh N MD, Consultant, Department of Radiology, National Cancer Institute, Nagpur, Maharashtra, India.
Copyright
© 2025 Haran Nilesh N. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 February 2025
Published: 25 February 2025
A Rare Complication of Targetted Therapy: Pazopanib-Induced Intestinal Lymphangiectasia
Introduction
Intestinal lymphangiectasia is thought to be caused by blockage of the lymphatic flow.
Primary is thought to be caused by congenital defects that affect the formation of lymphatic vessels. Secondary is thought to be caused by other underlying conditions that increase the pressure within the lymphatic vessels, such as intra-abdominal infections, tumors, or cirrhosis. However, in the absence of these underlying diseases, even secondary, much of the etiology of intestinal lymphangiectasia is currently unknown. [1] the expression of vascular endothelial growth factor receptor 3 (VEGFR3) and lymphatic vessel endothelial hyaluronan receptor-1 was increased on the intestinal mucosal surface and decreased in the deep mucosal layer in patients with intestinal lymphangiectasia.
The clinical course of our patient indicates that pazopanib plays an important role in the development of intestinal lymphangiectasia [2]. A review of molecularly targeted drugs showed the possible development of intestinal lymphangiectasia in patients taking pazopanib or axitinib.
Pazopanib is a multikinase inhibitor with VEGFR, platelet-derived growth factor receptor, and Kit as its target molecules, and these effects may have caused the development of intestinal lymphangiectasia in the present case.
Discussion
Intestinal lymphangiectasia is a rare disease characterized by dilatation of the intestinal lymphatics and loss of lymph fluid into the gastrointestinal tract, leading to hypoproteinemia, edema, lymphocytopenia, and hypogammaglobulinemia. Endoscopic abnormalities are obvious and include scattered white spots and white swollen villi corresponding to marked dilation of the lymphatics within the intestinal mucosa. [3]
In the present case CT examinations showed characteristic findings, and the patient was diagnosed with intestinal lymphangiectasia. [6]
This rare case highlighted the importance of monitoring patients on tyrosine kinase inhibitors for unusual side effects. Radiologist and oncologists should be aware of the potential risk of in intestinal lymphangiectasia associated with pazopanib and other VEGFR inhibitors. In this case, the discontinuation of pazopanib was necessary to manage intestinal lymphangiectasia.
Case Report
A 27-year-old male with complaints of swelling and pathological fracture involving the right iliac bone and was diagnosed as pleomorphic undifferentiated sarcoma on CT guided biopsy from the soft tissue mass.
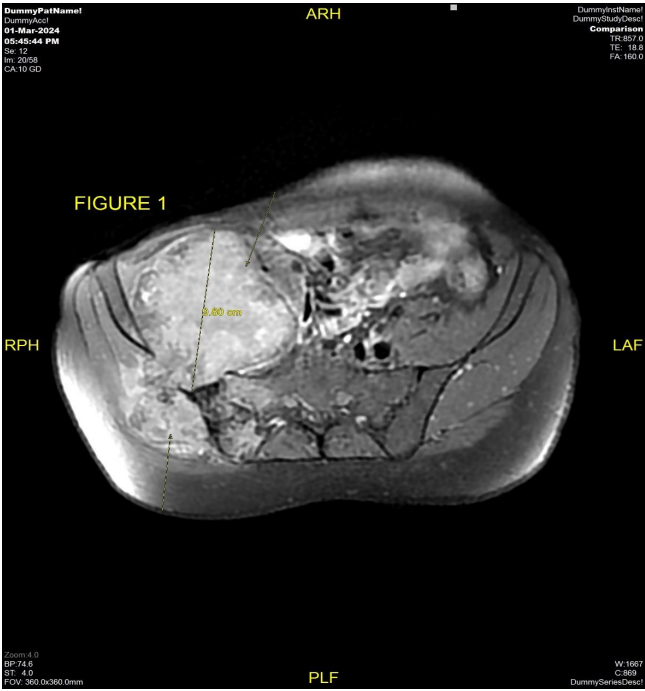
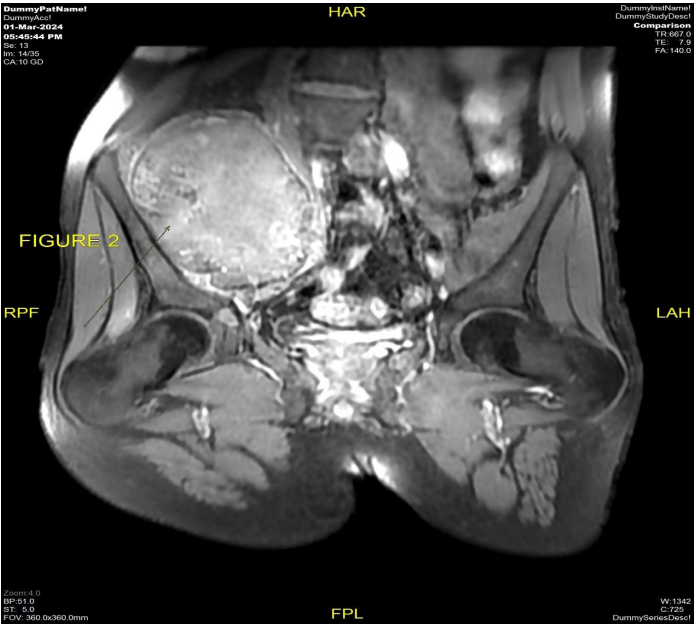
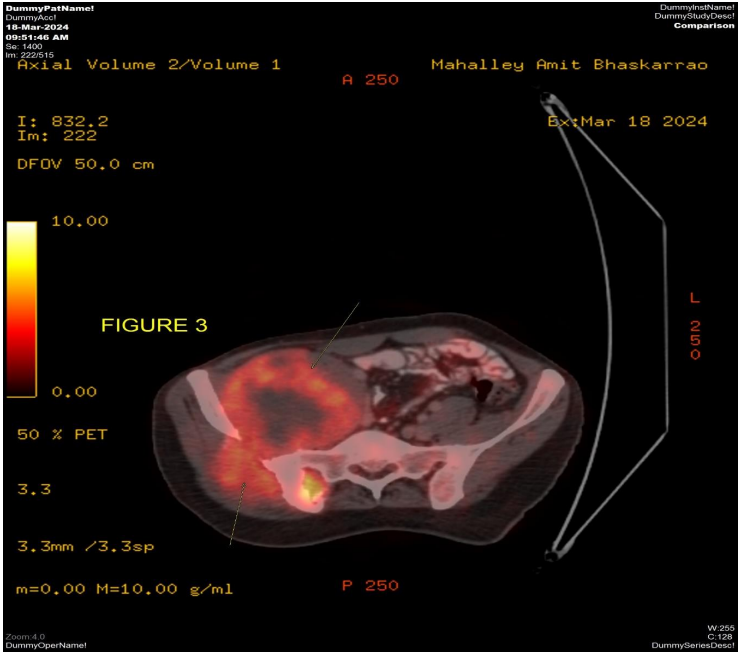
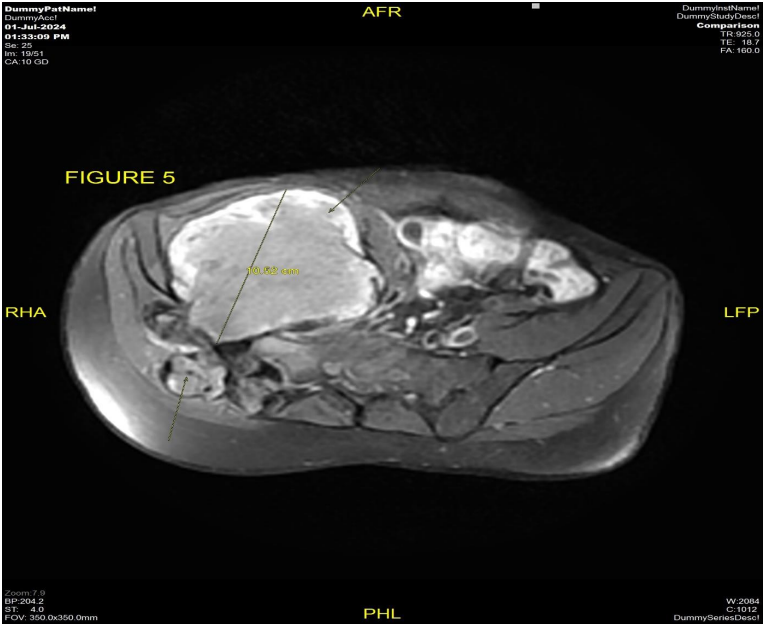
The patient underwent MRI pelvis (Fig 1 & 2) and PETCT (Fig 3 & 4) for initial evaluation (03/2024) at our institute which showed ill-defined large altered signal intensity heterogeneously enhancing mass in the right lumbar region with both intra as well as intrapelvic component by causing erosion of the right iliac bone involving the adjacent iliopsoas and gluteus muscles with central necrosis. On PET-CT scan the lesion showed significant FDG uptake with no other abnormality in the rest of the scan. Text the patient was planned for neoadjuvant chemotherapy and then for surgery. Patient took 2 cycles of neoadjuvant chemotherapy (Holoxan and Adriamycin), but after 2 cycles of chemotherapy response evaluation MRI was done (01/07/2024) (Fig 5) which showed increase in the size of lesion, so patient was planned for targeted therapy ie tyrosine kinase inhibitors, Pazopanib.
Response scan was done on 10/2024 (Fig 6) which showed mild interval decrease in the size and increase in necrosis of the right lumbar region lesion, with no other symptoms, show continued on pazopanib.
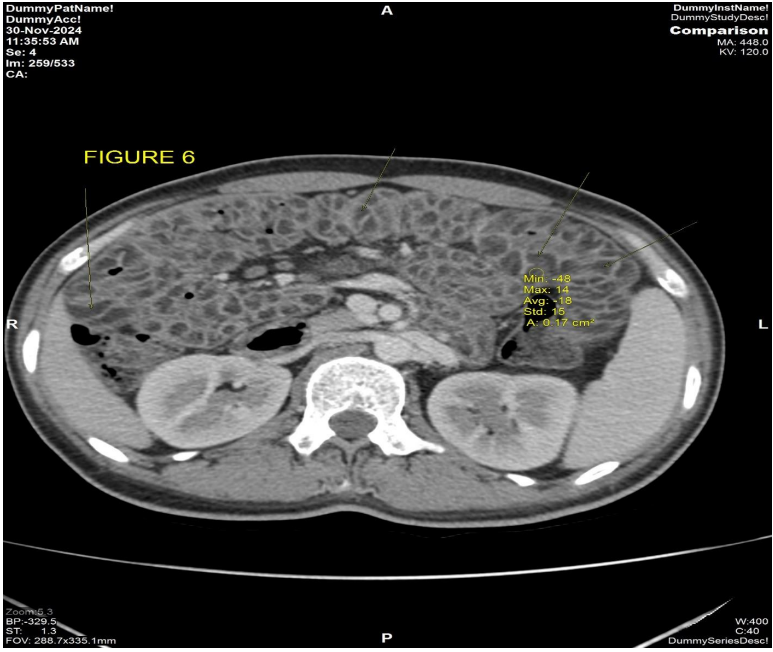
Patient complaint of abdominal pain with diarrhea and weight loss since 1 month, so a CECT thorax abdomen pelvis (Fig 6) was performed on 30/11/2024, which showed no interval change in the size and necrosis of the right lumbar region lesion, however there was new onset significant bowel wall thickening with submucosal fat deposition (-18 HU) mild luminal narrowing involving the entire jejunum with maximum thickness of 15 mm. [4]
The patient was counselled for stopping the Pazopanib therapy and started on Injection Gemcitabine and Docetaxel and was asked to follow up after 3 cycles of treatment.
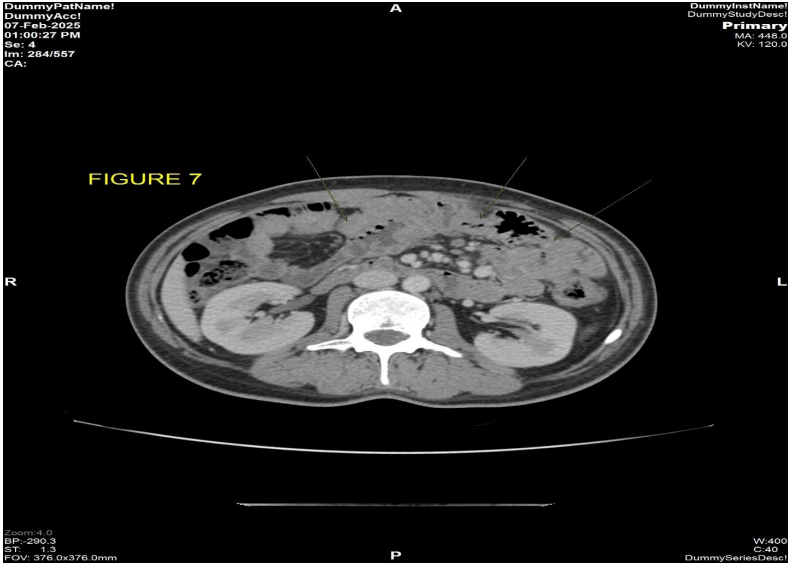
On follow up CECT thorax abdomen pelvis scan (Fig 7) dated 07/02/2025 there is complete resolution of bowel wall thickening and submucosal fat deposition seen involving the jejunal loops with resolution of the symptoms of abdominal pain and diarrhea. [5]
Figure 1 & 2: MRI pelvis dated 03/2024 axial and coronal view T1 post-contrast sequence shows ill-defined heterogeneously enhancing necrotic mass measuring approximately 9.8 cm in AP dimension is seen involving the right lumbar and pelvic region causing erosion of the adjacent right iliac bone and transverse process of S1 and S2 Vertebrae with both intra as well as extrapelvic component.
Figure 3: PETCT scan dated 03/2024 axial pelvic view shows ill-defined heterogeneous significantly FDG avid necrotic mass involving the right lumbar and pelvic region causing erosion of the adjacent right iliac bone and transverse process of S1 and S2 Vertebrae with both intra as well as extrapelvic component.
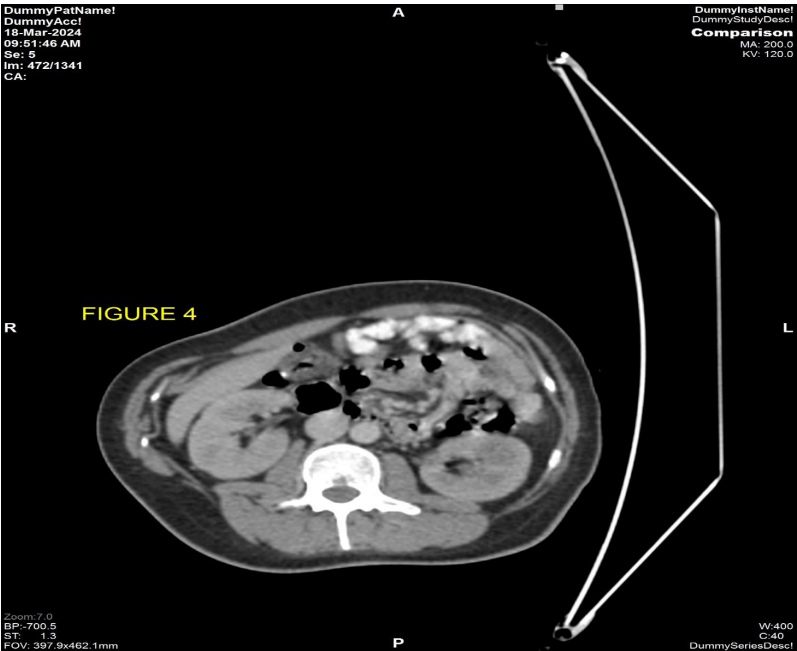
Figure 4: CT component of PETCT scan dated 03/2024 axial abdomen view shows normal small bowel wall with no obvious thickening seen.
Figure 5: MRI pelvis dated 07/2024 axial view T1 post-contrast sequence shows interval increase in the size of ill-defined heterogeneously enhancing necrotic mass measuring approximately 10.5 cm in AP dimension involving the right lumbar and pelvic region causing erosion of the adjacent right iliac bone and transverse process of S1 and S2 Vertebrae with both intra as well as extrapelvic component.
Figure 6: CECT abdomen dated 30/11/2024 axial post contrast view shows diffuse circumferential bowel wall thickening with submucosal fat is seen involving the jejunal wall with HU of -13, consistent with fat.
Figure 7: CECT abdomen dated 07/02/2024 axial post contrast view shows complete resolution of the previously seen diffuse circumferential bowel wall thickening with submucosal fat is seen involving the jejunal loops.
Conclusion
In patients with general malaise, hypoalbuminemia, and anemia despite normal endocrine function, it is necessary to consider the possibility that small intestinal lymphangiectasia may have developed during the treatment with multikinase inhibitors. In addition, radiologists should pay attention to the presence of characteristic thickening of the small intestinal wall on CT images in patients who have been taking multikinase inhibitors for a long time. As the condition is reversible after discontinuation of the drug.
Conflict of Interest; None declared
Funding; None declared
References
1. Kimihiko Masui Et al, A rare case of intestinal lymphangiectasia induced by pazopanib
2. Vardy PA, Lebenthal E, Shwachman H. Intestinal lymphangiectasia: a reappraisal. Pediatrics 1975; 55:842-851
3.Fox U, Lucani G. Disorders of the intestinal mesenteric lymphatic system. Lymphology 1993; 26:61-66
4. Dal Mo Yang and Dong Hae Jung, Localized Intestinal Lymphangiectasia: CT Findings
5. Fakhri A, Fishman EK, Jones B, Kuhajda F, Siegelman SS. Primary intestinal lymphangiectasia: clinical and CT findings. J Comput Assist Tomogr 1985; 9:767-770
6. Puri AS, Aggarwal R, Gupta RK, et al. Intestinal lymphangiectasia: evaluation by CT and scintigraphy. Gastrointest Radiol 1992; 17:119-121.