Pediatric Soft Tissue Sarcoma in a 7-Year-Old Girl
Pediatric Soft Tissue Sarcoma in a 7-Year-Old Girl
Dr. Vivek Viswanathan *
*Correspondence to: Dr. Vivek Viswanathan, Consultant in Paediatric Urology and Minimal Access Pediatric Surgery, Bhailal Amin General Hospital, Vadodara, Gujarat, India.
Copyright
© 2025: Dr. Vivek Viswanathan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 Apr 2025
Published: 02 May 2025
Abstract
Aims: This case report aims to describe the clinical presentation, histopathological findings, surgical management, and outcome of a rare pediatric soft tissue sarcoma in a 7-year-old girl, focusing on the diagnostic hurdles and treatment strategies employed.
Methods and Results: A 7-year-old female presented with a 6-month history of a painless, progressively enlarging mass in the right thigh. Imaging revealed a 5 cm heterogeneous mass, and a biopsy confirmed a high-grade spindle cell sarcoma with immunohistochemical positivity for vimentin and focal desmin. Surgical resection was done with clear margins confirmed on biopsy, followed by adjuvant chemotherapy. Histopathology showed spindle-shaped cells with high mitotic activity and necrosis, with additional sections revealing dense cellularity and fascicular growth. At 12-month follow-up in March 2025, the patient remained disease-free.
Conclusions: This case highlights the importance of early recognition, histopathological confirmation, and multidisciplinary management in pediatric soft tissue sarcomas, with favorable outcomes possible when treated aggressively.
Keywords: pediatric sarcoma, soft tissue tumor, histopathology, surgical resection, spindle cell sarcoma.
Pediatric Soft Tissue Sarcoma in a 7-Year-Old Girl
Introduction
Soft tissue sarcomas are rare in children, constituting approximately 7% of all pediatric malignancies. These tumors have nonspecific clinical features and histological variability and so present diagnostic challenges. This case report presents the case of a 7-year-old girl with a high-grade spindle cell sarcoma of the right thigh, highlighting the histopathological findings, surgical intervention, and clinical outcome. The work has been reported in accordance with the SCARE criteria [1].
Case Presentation
A 7-year-old female presented to the pediatric outpatient department with a 6-month history of a painless mass in the right thigh. It gradually grew from an incidentally detected small lump to the present size at consultation over the course of 6 months. There was no preceding history of trauma, fever, weight loss, or other constitutional symptoms. Her past medical history was clear, and there was no family history of cancer.
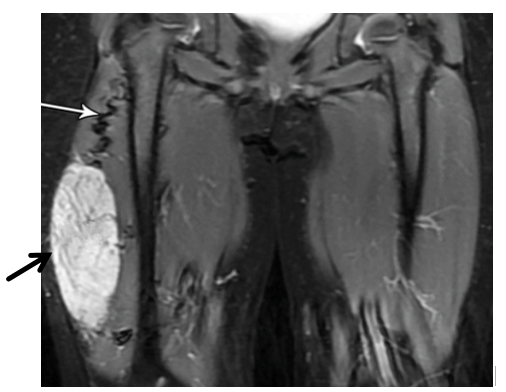
During the exam, we found a firm, non-painful, fixed mass in the front-inner part of her right thigh, measuring roughly 5 x 4 cm. The skin over the mass looked normal, and there were no swollen lymph nodes nearby. Blood tests, including a full blood count and markers of inflammation, came back normal. An MRI scan showed a 5.2 x 4.1 x 3.8 cm mass with uneven borders and mixed characteristics, pointing to a possible cancerous soft tissue tumor.
Figure 1: MRI Scan (T2-weighted MRI (coronal view) of the lower pelvis and thighs)
Description: 5.2 x 4.1 x 3.8 cm mass in the right thigh with an irregular oval shape, showing a mix of bright white (hyperintense) and darker gray (hypointense) areas, suggestive of a malignant soft tissue sarcoma. A black arrow points to the mass, confirming its size matches the measurements. The white arrow highlights a winding, high-flow blood vessel feeding the tumor. The surrounding muscle tissue looks medium gray, while the femur appears dark (low signal). The left thigh, shown for comparison, has normal muscle and bone structure.
An incisional biopsy was performed under general anesthesia. Microscopic examination revealed tightly packed spindle-shaped cells, irregular nuclei, few dividing cells and areas of necrosis, consistent with the diagnosis of a high-grade spindle cell sarcoma. Special staining tests showed strong positivity for vimentin and slight positivity for desmin, but were negative for S100, CD34, and myogenin, supporting a diagnosis of an undifferentiated spindle cell sarcoma.
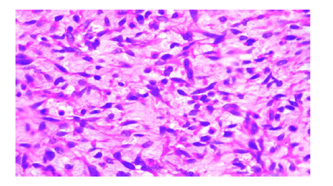
Figure 2: Histopathology Image
Description: This microscope image (H&E stain, 400x magnification) of the biopsy shows a high-grade spindle cell sarcoma. It features a dense cluster of spindle-shaped cells with long, darkly stained nuclei and minimal surrounding material, arranged in bundles. The nuclei vary in size and shape, showing notable irregularity. A few dividing cells are visible, but dead tissue areas aren’t prominent here. The background has the typical pink-purple tones of H&E staining, with some fibrous tissue mixed in.
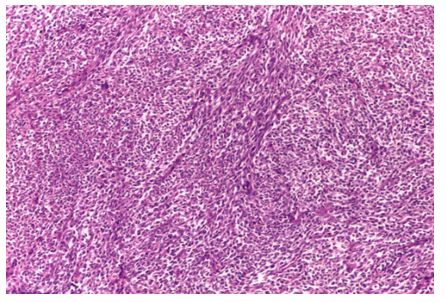
Figure 3: Additional Microscopic View
Description: Another microscope image (H&E stain, 200x magnification) of a different section of the tumor, also showing a high-grade spindle cell sarcoma. This view reveals a highly cellular tumor with spindle-shaped cells in a bundled pattern. The cells have long, darkly stained nuclei with moderate to significant irregularity and little surrounding material. Fibrous tissue is seen in the background, stained in the usual pink-purple H&E colors. Dividing cells and necrotic tissue aren’t obvious in this section, likely due to differences in the sampled area, but the cell structure matches the sarcoma seen in Figure 2.
Informed consent was obtained from the patient’s parents for the publication of this case report, ensuring all data was de-identified to protect privacy.
Surgical Management
Wide local excision was performed on March 15, 2024, under general anesthesia. A longitudinal incision was made over the anteromedial thigh, and the mass was excised with a 2 cm margin of healthy tissue. During the procedure, we confirmed that the mass was limited to the soft tissue, with no spread to the femur or nearby blood vessels and nerves. The surgical site was closed in layers, and the removed tissue was sent for further histopathological analysis.
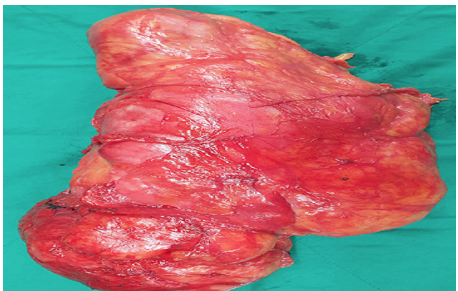
Figure 4: Surgical Photo
Description: This photo shows the removed mass after surgery, a 5 cm soft tissue sarcoma from the right thigh. The tumor looks lobulated and reddish-pink, with a varied surface, measuring about 5 x 4 x 3 cm. The cut surface shows a mix of solid and bloody areas, with some parts looking more fibrous. A thin layer of healthy pink muscle tissue surrounds the mass, matching the 2 cm surgical margin. The specimen is placed on a green sterile drape, typical of an operating room, showing the tumor’s uneven edges and mixed texture.
Further microscopic analysis after surgery confirmed that the edges of the removed tissue were clear of cancer cells (>1 cm margin) and reaffirmed the diagnosis of a high-grade spindle cell sarcoma. The girl recovered well and was discharged 5 days after surgery. She then started chemotherapy with vincristine, doxorubicin, and cyclophosphamide, given the tumor’s aggressive features.
Recovery and Follow-Up
At her 12-month check-up in March 2025, the girl showed no signs of cancer recurrence, based on physical exams and imaging (MRI and chest CT). She was back to her usual activities, though she had slight weakness in her right thigh, likely from the surgery.
Discussion
Soft tissue sarcomas in children are a diverse group, and spindle cell sarcomas are a rare type within this category. The MRI (Figure 1) revealed a mass with uneven borders and mixed signal patterns, which is typical for cancerous soft tissue tumors and helped guide the decision to biopsy and operate. Under the microscope, the tumor showed spindle-shaped cells, frequent cell division, and areas of tissue death, all signs of an aggressive cancer that needed quick action [2]. The microscopic images (Figures 2 and 3) highlight the spindle cell structure, with Figure 2 showing a few dividing cells and Figure 3 emphasizing the dense, bundled cell arrangement. The lack of visible cell division or dead tissue in Figure 3 is likely due to differences in the sampled area, as tumors can vary across sections. The surgical specimen (Figure 4) reveals a tumor with bloody and fibrous areas, matching the aggressive nature of high-grade sarcomas. Special staining was key in ruling out other tumors like rhabdomyosarcoma, which was excluded due to the lack of myogenin staining and only focal desmin positivity, and synovial sarcoma, which was less likely due to the absence of epithelial markers and the overall staining pattern [3]. The positive outcome here highlights the importance of removing the tumor with clear margins and using additional treatments like chemotherapy, as recommended by current guidelines [4].
Advanced tools like digital pathology and whole slide imaging could improve diagnosis in cases like this by enabling remote expert reviews and detailed image studies [5].
Conclusion
This case demonstrates how a rare spindle cell sarcoma in a child can be successfully managed with early detection, accurate histopathological evaluation, and a comprehensive treatment plan. It stresses the need for a team approach and shows how microscopic analysis can guide effective care.
Additional Information
Conflicts of Interest: The author declares no conflicts of interest.
Funding: No funding was received for this study.
Ethical Approval: Ethical approval was not required as this is a case report with de-identified data, in line with institutional guidelines.
Acknowledgments: None.
References
1. Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler A, Orgill DP, et al. The SCARE 2018 Statement: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg. 2018;60:132-6.
2. Samaila MO. Malignant tumours of childhood in Zaria. Afr J Paediatr Surg. 2009;6(1):19-23.
3. Gurcan MN, Boucheron LE, Can A, Madabhushi A, Rajpoot NM, Yener B. Histopathological image analysis: a review. IEEE Rev Biomed Eng. 2009;2:147-71.
4. Nri-Ezedi CA, Ulasi TO, Menkiti FE, Ndukwe CO, Igwenagu CM, Akpuaka FC. Epidemiological trends and treatment abandonment of paediatric solid tumours in a Nigerian tertiary hospital: a seven-year review (2016-2022). BMC Cancer. 2024;24(1):943.
5. Snead DR, Tsang YW, Meskiri A, Kimani PK, Crossman R, Rajpoot NM, et al. Validation of digital pathology imaging for primary histopathological diagnosis. Histopathology. 2016;68(7):1063-72..