Double Thyroglossal Duct Cysts; A Case Report
Double Thyroglossal Duct Cysts; A Case Report
Waleed A. Elsayed MD1*, Hussah AlBuainain MD2, Hossam Elshafei MD, FACS3
1. Pediatric Surgery Division, King Fahd Hospital of the University, Alkhobar
2. Imam Abdulrahman Bin Faisal University, Saudi Arabiayu
*Correspondence to: Waleed A. Elsayed, Saudi Arabia.
Copyright
© 2025: Waleed A. Elsayed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 Apr 2025
Published: 02 May 2025
DOI: https://doi.org/10.5281/zenodo.15324425
Abstract
Introduction: Thyroglossal duct cysts ( TGDCs ) are common cause of congenital neck swellings in pediatric patients, embryological cause as the remnant of the tract caused by thyroid gland migration from base of tongue till its normal position in lower neck explaining the possible positions of TGDCs at midline anteriorly in neck, related mainly to hyoid bone which should be included in the dissection during the surgical management to prevent recurrence. Case presentation: TGDCs are commonly single, we reported double TGDCs related to the same duct and infrahyoid in position in a 4-year-old boy, discussing the management with a literature review of this rare condition. Conclusion: It is important to diagnose this condition to prevent complications; mainly recurrence.
Keywords: Thyroglossal duct cyst, neck swelling, double cyst, Sistrunk, Hyoid bone, case report.
Double Thyroglossal Duct Cysts; A Case Report
Introduction
Thyroglossal duct cysts (TGDCs) are the most common congenital neck swellings in pediatric populations, with incidence of 7%, embryologically. Thyroid gland develops at the foramen cecum at the tongue base and descends to the neck leaving a tract called thyroglossal duct which usually involutes at 10th week of gestational age. Failure of involution of this duct causes the TGDCs (1).
TGDCs are usually single, we reported this case of double cysts from the same thyroglossal duct which is a rare presentation with few documented cases in literature.
“This manuscript was prepared following the CARE guidelines (https://www.care-statement.org)”.
Case Presentation
A four-year-old boy presented to our clinic for evaluation of anterior neck swelling, one week prior to the presentation this mass was noticed, as a painful neck mass and physical examination in ED revealed a lower midline neck mass which was erythematous, tender and warm, measuring 2 x 2 cm, diagnosed as infected thyroglossal cyst and antibiotic was started. Antibiotic was given for 7 days.
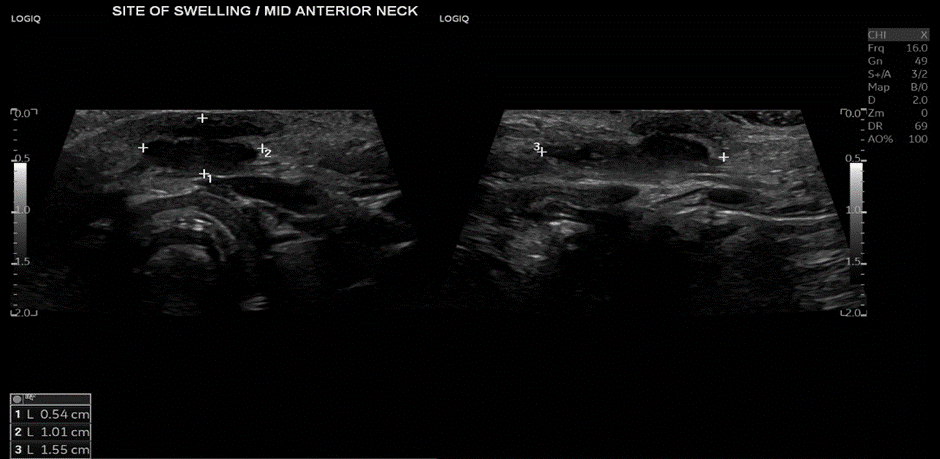
Revaluation of the case one week later in our clinic showed that inflammation subsided, no redness or hotness, no cervical lymph nodes were detected, an ultrasound neck was done and revealed a bilobed hypoechoic lesion located anterior to the hyoid bone, measuring 0.5 x 1 x 1.55 cm, consistent with a thyroglossal cyst, (figure 1).
Figure 1: US neck showing the bilobed swelling
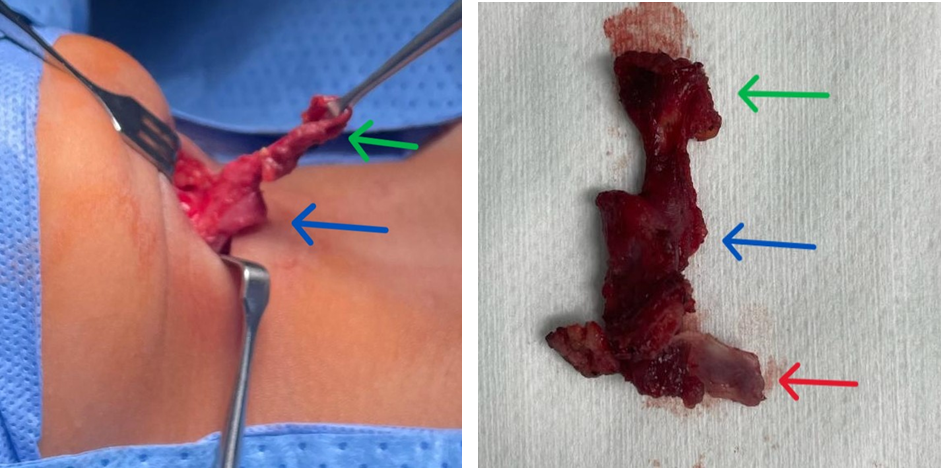
4 weeks later after the inflammation has subsided; patient underwent Sistrunk procedure, the cyst was adherent and fixed to the overlaying skin, so elliptical incision done around the cyst, dissection progressed proximal to it following the tract, before reaching the hyoid bone; another cyst about 2 x 2 cm detected, dissection continued excising middle part of hyoid bone, (figures: 2&3). Surgical pathology result was consistent with thyroglossal duct cyst with no malignancy. Patient was followed up in our clinic and post operative coarse was uneventful.
Figure 2 & 3: Green Arrow; Distal collapsed (ruptured) TGDC, Blue Arrow; Proximal second TGDC, Red Arrow; Central part of Hyoid bone.
Discussion
TGDC is one of the commonest causes of congenital neck swellings, presenting in about 7% of the population (1), and 70% of cases occurs in paediatric age group, with bimodal case distribution with age at diagnosis (0–10 or 40–50 y). (2),
TGDC forms as a result of failure of regression of thyroglossal duct which develops embryologically as thyroid gland travels from base of the tongue to the lower neck passing adherent to the hyoid bone, so the cyst could be anywhere along that course, it usually presents as asymptomatic anterior midline neck swelling that moves up and down with protrusion of tongue and swallowing, however it can be infected causing tenderness, erythema and fever, or even dysphonia and dysphagia (3), Further diagnostic imaging should be obtained to rule out other midline neck masses including dermoid cyst, ectopic thyroid tissue and malignancies, branchial cleft cyst, lymphadenopathy, lymphangioma, lipoma, and teratomas (4), ultrasonography (US) is important to confirm the diagnosis and rule out ectopic thyroid, In this case US was done and showed normal thyroid.
Sistrunk procedure is the gold standard for treatment of TGDC, with lower recurrence rate compared to the simple excision (6.9% vs 29% recurrence, respectively), presumably due to complete removal of the thyroglossal duct remnants (5), the Sistrunk procedure generally started with anterior transverse neck incision along the skin crease or elliptical incision if cyst is adherent to skin as we faced in this case, dissection continued through platysma and strap muscles, cyst is located and dissected cautiously from inferior, dissection continued upwards following the presumed thyroglossal tract till hyoid bone, in this case another cyst about 2x2 cm was detected along with the same tract, strap muscles separated from the central part of hyoid, and the central portion of the hyoid bone is separated medially to the lesser cornua bilaterally, dissection continued superiorly following the tract till the base of tongue, the presumed tract is ligated. The cysts, the presumed thyroglossal tract and the central part of hyoid bone removed en-bloc and sent for pathology.
Histopathology of TGDC consists of either squamous or respiratory pseudostratified epithelium and usually filled with mucus, in contrast to dermoid cysts that contain keratinaceous debris (6).
Double TGDCs that reported in literature showed variation in their sites, in our case both cysts were inferior to hyoid, other sites were reported, collected in table(1).
|
Case reports |
Location of cysts |
|
Walsh et al (2023) (7) |
Inferior to thyroid & inferior to Hyoid |
|
Lee et al. (2017) (8) |
Infrahyoid & tongue base |
|
Yildiz et al. (2014) (4) |
Superior to thyroid isthmus & suprahyoid |
|
Sarmento et al. (2013) (9) |
Superior to geniohyoid & sublingual gland |
|
Yorganc?lar et al. (2011) (10) |
Cervical mass & tongue base with communicating tract |
|
Khadivi and Ardekani (2010) (11) |
Two separate infrahyoid cysts with communicating tract |
|
Guo et al. (2008) (12) |
Suprahyoid & tongue base |
Conclusion
Double thyroglossal duct cysts are rare, imaging and histopathological examinations are important to confirm the diagnosis, Sistrunk procedure is the proper management to avoid complications and recurrence.
Statement: Informed consent was obtained from the parent to publish without showing patient’s face as per request. All authors attest that they meet the current ICMJE criteria for Authorship.
References
1. Thyroglossal duct cyst. [May; 2023]. 2022. https://www.ncbi.nlm.nih.gov/books/NBK519057/.
2. Guo Y, Huang Q, Chen H, et al. Uncommon insidious dumbbell-shaped double thyroglossal duct cyst. J Craniofac Surg 2023;34: e122–e124
3. Thyroglossal cyst: an unusual presentation. Karmakar S, Saha AM, Mukherjee D. Indian J Otolaryngol Head Neck Surg. 2013;65:185–187. [PMC free article] [PubMed] [Google Scholar].
4. A rare form of thyroglossal duct cyst: double thyroglossal cyst and review of the literature. Yildiz T, Ilce HT, Kucuk A, Ilce Z. J Turgut Ozal Med Cent. 2014; 21:148–150. [Google Scholar]
5. Management of suspected thyroglossal duct cysts. Povey HG, Selvachandran H, Peters RT, Jones MO. J Pediatr Surg. 2018;53:281–282. [PubMed] [Google Scholar] [Ref list]
6. Pathology of thyroglossal duct: an institutional experience. Wei S, LiVolsi VA, Baloch ZW. Endocr Pathol. 2015; 26:75–79. [PubMed] [Google Scholar]
7. Walsh J, Clausen S, Degiovanni J, Carr MM. Double Thyroglossal Duct Cyst: A Case Report. Cureus. 2023 Jun 19;15(6): e40660. doi: 10.7759/cureus.40660. PMID: 37485128; PMCID: PMC10356570.
8. Double thyroglossal duct cysts in an adult. Lee DH, Yoon TM, Lee JK, Lim SC. J Craniofac Surg. 2017;28:90–91. [PubMed] [Google Scholar].
9. Double thyroglossal duct cyst involving the floor of the mouth and sublingual gland region. Sarmento DJ, Araújo PP, da Silveira EJ, Germano AR. J Craniofac Surg. 2013;24:116–119. [PubMed] [Google Scholar].
10. Double thyroglossal duct cyst located in the hyoid region and the tongue base: an unusual coexistence. Yorganc?lar E, Y?ld?r?m M, Gün R, Büyükbayram H, Topçu I. Kulak Burun Bogaz Ihtis Derg. 2011; 21:106–109. [PubMed] [Google Scholar].
11. Double thyroglossal duct cyst derived from a single tract: a rare presentation. Khadivi E, Ardekani H. Iran J Otorhinolaryngol. 2010; 22:103–106. [Google Scholar].
12. Uncommon insidious dumbbell-shaped double thyroglossal duct cyst. Guo Y, Huang Q, Chen H, Xu C. J Craniofac Surg. 2023;34:122–124. [PMC free article] [PubMed] [Google Scholar] [Ref list].