Social Equality: A Multidimensional Approach to Justice, Access, and Inclusion in the 21st Century
Social Equality: A Multidimensional Approach to Justice, Access, and Inclusion in the 21st Century
Riya Singhal *1; Varsha Ojha 2
1) Riya Singhal, Deira International School.
2) Varsha Ojha, Consultant OBGYN, Prime Hospital, Dubai.
*Correspondence to: Riya Singhal, Deira International School.
Copyright
© 2025 Riya Singhal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 12 May 2025
Published: 15 May 2025
Abstract
Social equality is a critical cornerstone of modern democratic societies, encompassing the principles of equal access, equal rights, and equitable treatment for all individuals irrespective of their socio-economic status, gender, race, ethnicity, religion, ability, or other identity attributes. This research article presents a comprehensive analysis of the concept of social equality through a multidimensional lens, integrating perspectives from political theory, sociology, economics, education, public health, and international human rights law. By examining the historical evolution of equality movements—from the abolitionist and suffragist eras to contemporary campaigns for racial justice, gender parity, LGBTQ+ rights, and disability inclusion—this study illustrates how the notion of equality has transitioned from formal legal recognition to a deeper focus on substantive and structural change.
The article explores the primary domains where social inequality persists, including income and wealth distribution, educational attainment, healthcare access, gender-based disparities, and racial and ethnic discrimination. It underscores how systemic barriers, often rooted in colonial histories, patriarchal norms, and neoliberal economic systems, continue to perpetuate inequality across generations and geographies. Particular attention is given to intersectionality and the ways in which overlapping forms of discrimination can exacerbate exclusion, especially among marginalized and vulnerable populations.
Using contemporary data, graphs, and case studies, the research evaluates both the progress made and the continuing challenges in realizing a socially equal world. It investigates how new global phenomena—such as digital divides, climate injustice, and post-pandemic recovery—are influencing the terrain of equality and shaping the policy responses needed. The paper also reviews major international and national policy frameworks and legal instruments that have sought to institutionalize social equality, while offering critical insight into their effectiveness and limitations.
Ultimately, this article argues that achieving genuine social equality requires more than legal reforms or policy interventions—it demands a systemic transformation of social values, institutional practices, and economic structures. It calls for an intersectional, inclusive, and participatory approach that centers lived experiences and promotes both equity and empowerment at all levels of society. The findings and recommendations presented herein aim to inform scholars, policymakers, activists, and institutions committed to building fairer and more just communities in the 21st century.
Social Equality: A Multidimensional Approach to Justice, Access, and Inclusion in the 21st Century
1. Introduction
Social equality is one of the foundational pillars of a just and sustainable society. It refers to a condition in which individuals within a society have equal rights, responsibilities, and opportunities, regardless of their socio-economic status, gender, race, ethnicity, religion, sexual orientation, disability, or any other identity marker. More than just the absence of discrimination or bias, social equality embodies the fair distribution of resources, access to public services, and full participation in the political, economic, and cultural life of a community.
The conceptual roots of social equality trace back to classical philosophy and enlightenment ideals. Thinkers such as Rousseau, Locke, and Mill advocated for egalitarian principles, envisioning societies where human dignity was respected and social hierarchies were minimized. In the modern era, philosophers like John Rawls and Amartya Sen have further advanced the discourse, emphasizing not just equal treatment under the law, but equity—where systemic disadvantages are acknowledged and corrected to enable fair outcomes. Rawls’s principle of “fair equality of opportunity” and Sen’s “capabilities approach” have significantly influenced contemporary policies on social justice and human development.
Historically, the pursuit of social equality has been central to major civil rights movements and social revolutions. The abolition of slavery, women's suffrage, labor rights activism, LGBTQ+ movements, and indigenous rights campaigns all exemplify humanity’s enduring struggle to eliminate injustice and expand inclusivity. These movements have reshaped constitutional democracies, led to the formation of international human rights instruments, and compelled the recognition of minority rights in global governance structures.
However, despite these advances, substantive social equality remains far from realized in many parts of the world. Structural inequalities are deeply entrenched through legacies of colonialism, patriarchy, caste hierarchies, racial segregation, and economic exploitation. For instance, women and ethnic minorities continue to face disparities in wages, representation, and personal safety. In low-income countries, millions still lack access to basic education, healthcare, or dignified employment. Even in affluent nations, income polarization, housing inequality, and digital exclusion persist as major barriers to equitable progress.
Moreover, emerging global challenges—such as climate change, forced migration, pandemics, and automation—have exacerbated existing inequalities and created new forms of vulnerability. The COVID-19 crisis, for example, revealed how marginalized populations bore the brunt of health risks, unemployment, and digital disenfranchisement. These trends highlight the urgent need to not only protect rights on paper but to enforce social equality through proactive governance, inclusive policymaking, and intersectional frameworks.
In today's interconnected world, the relevance of social equality extends beyond national borders. Inequality anywhere can have ripple effects everywhere—fuelling social unrest, radicalization, health crises, and economic instability. Thus, social equality is not just a moral imperative but a prerequisite for sustainable development, democratic stability, and global peace. As societies become increasingly diverse and digital, the challenge lies in designing inclusive systems that uphold dignity, foster solidarity, and empower every individual to flourish.
This article explores the multidimensional nature of social equality, its various expressions across economic, educational, gender, racial, and health domains, the current barriers to achieving equality, and the policy frameworks that can pave the way forward. Supported by empirical data, graphs, and comparative analysis, the research advocates for a holistic and intersectional approach to realizing a more just global society.
2. Dimensions of Social Equality
2.1. Economic Equality
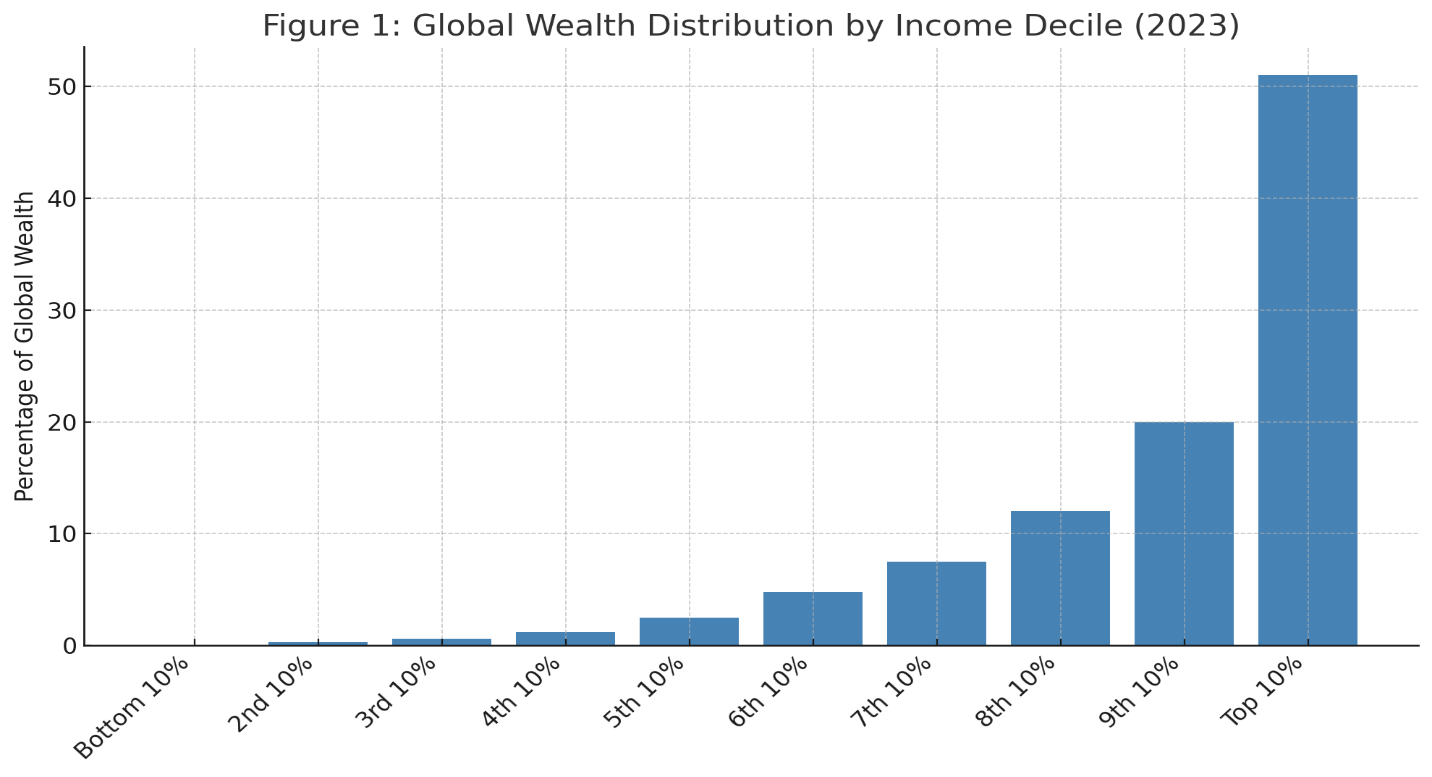
Economic inequality remains a cornerstone of social stratification. Wealth concentration, wage disparities, and intergenerational poverty significantly limit upward mobility. In most societies, the top 10% control over 60% of wealth, creating a power imbalance that impedes equal opportunity.
Policies to promote economic equality include:
- Progressive taxation
- Universal basic income (UBI)
- Minimum wage legislation
- Equal pay for equal work initiatives
Despite these efforts, neoliberal globalization and deregulation have widened income gaps, particularly in developing nations.
2.2. Educational Equality
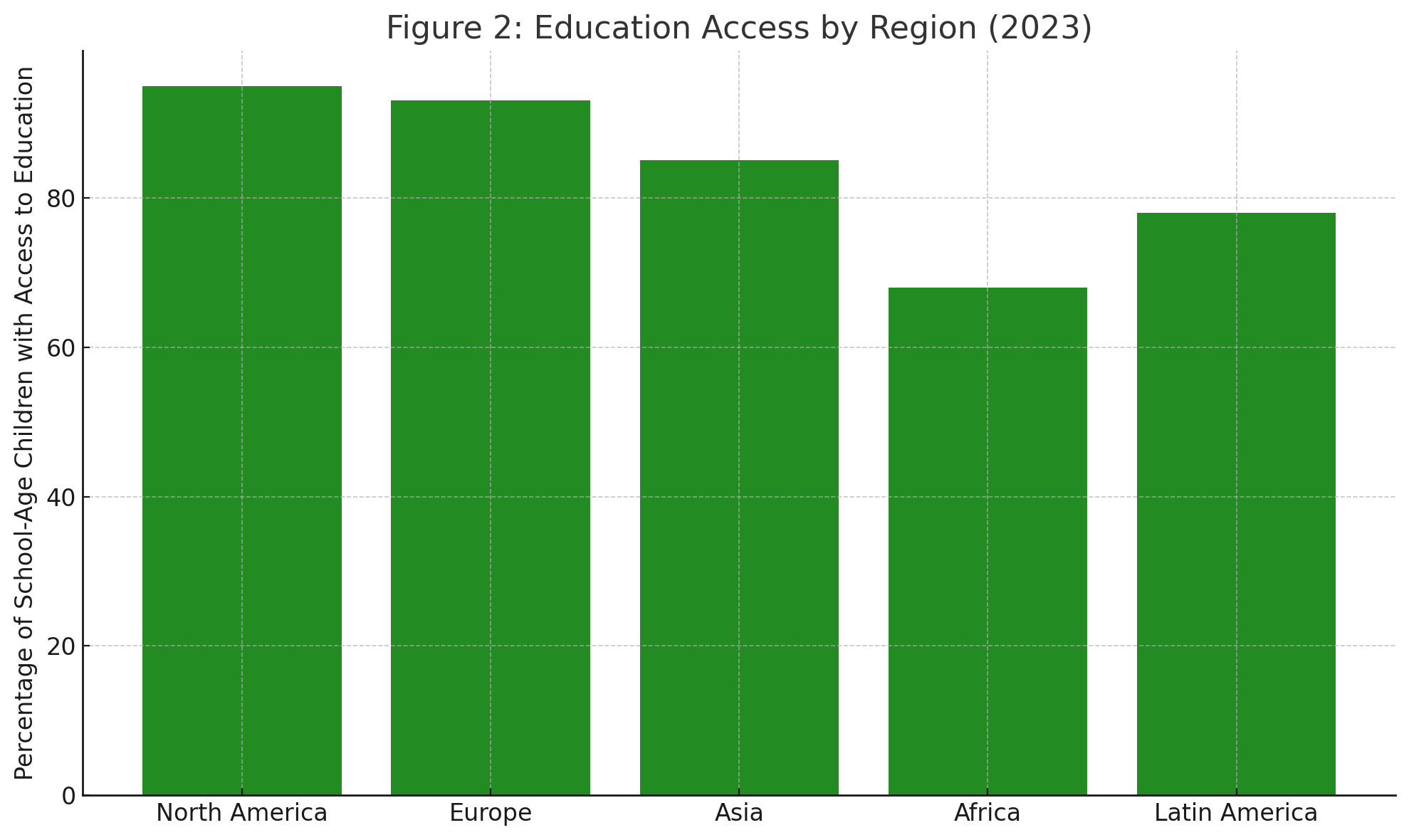
Access to quality education is a pivotal equalizer. Yet disparities persist based on geography, gender, race, and disability. In many regions, children from poor or rural backgrounds lack access to competent teachers, digital resources, or safe school environments.
Strategies for educational equality include:
- Inclusive curricula
- Digital infrastructure in rural areas
- Scholarships for marginalized groups
- Anti-bias teacher training
Empirical studies show that closing the education gap can reduce inequality across generations and lead to more inclusive labor markets.
2.3. Gender Equality
Despite decades of advocacy, gender disparities remain widespread. Women and gender minorities face unequal pay, underrepresentation in leadership, and restricted bodily autonomy. In some countries, harmful practices such as child marriage, gender-based violence, and reproductive control persist.
Key approaches to gender equality:
- Gender mainstreaming in policy
- Legal protections against discrimination
- Support for reproductive health and maternity rights
- Political representation quotas
Global indices such as the Gender Equality Index (GEI) reveal that no country has achieved full gender parity.
2.4. Racial and Ethnic Equality
Ethnic minorities and indigenous peoples often suffer from institutionalized racism, xenophobia, and exclusion from decision-making processes. These inequalities manifest in law enforcement, employment, education, and housing.
Combating racial inequality involves:
- Anti-discrimination laws
- Affirmative action policies
- Cultural competency training
- Historical redress and reparations
The Black Lives Matter movement and anti-caste activism in South Asia are contemporary examples of resistance and reform.
2.5. Health Equality
Health disparities correlate with social determinants such as income, location, education, and race. COVID-19 exposed stark inequities in healthcare access, vaccine distribution, and mortality rates.
Health equality interventions:
- Universal health coverage
- Public health education
- Mental health services
- Free vaccination programs
Countries with strong public healthcare systems report better outcomes for marginalized populations.
3. Contemporary Challenges to Social Equality
3.1. Digital Divide
In the digital age, internet access is a basic need. Yet over 2.6 billion people remain offline—mainly in rural and low-income regions. Digital exclusion limits educational, economic, and political participation.
Bridging the gap:
- Subsidized internet access
- Community tech hubs
- Digital literacy programs
3.2. Intersectionality
Inequality is multifaceted—people may face simultaneous discrimination based on gender, race, and disability. Intersectionality reveals how overlapping identities exacerbate disadvantage.
For instance, a low-income, Black woman with a disability may face compounded exclusion in hiring, healthcare, and civic life.
3.3. Political Polarization and Backlash
In many democracies, progress on social equality is met with populist backlash, hate speech, and regressive legislation. Conservative waves often target gender rights, immigration, and racial justice, threatening the liberal democratic order.
4. Policy and Legal Frameworks Supporting Social Equality
|
Framework / Law |
Region |
Focus Area |
Year Passed |
|---|---|---|---|
|
Civil Rights Act |
United States |
Racial and gender equality |
1964 |
|
Right to Education Act |
India |
Free education for children |
2009 |
|
Equality Act |
United Kingdom |
Anti-discrimination |
2010 |
|
Universal Declaration of Human Rights |
Global (UN) |
All rights and freedoms |
1948 |
|
Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) |
Global (UN) |
Gender equality |
1979 |
5. Graphical Data
Figure 1: Global Wealth Distribution by Income Decile (2023)
Figure 2: Education Access by Region (2023)
6. Conclusion
Social equality remains an unfinished but essential project in the 21st century. While legislative and institutional reforms have made significant strides, deeper structural issues and cultural norms continue to foster exclusion and hierarchy. Achieving substantive equality requires a multidimensional strategy—one that includes legal frameworks, public policy, civic activism, and ethical leadership. In a globally interconnected society, inequality anywhere threatens justice everywhere. Thus, the fight for equality must be relentless, intersectional, and inclusive.
References
1. Rawls, J. (1971). A Theory of Justice. Harvard University Press.
2. Sen, A. (1999). Development as Freedom. Oxford University Press.
3. UNDP. (2024). Human Development Report. https://hdr.undp.org
4. Piketty, T. (2014). Capital in the Twenty-First Century. Harvard University Press.
5. World Economic Forum. (2024). Global Gender Gap Report.
6. WHO. (2023). Global Health Equity Tracker.
7. UNESCO. (2024). Global Education Monitoring Report.
8. Crenshaw, K. (1989). "Demarginalizing the Intersection of Race and Sex." University of Chicago Legal Forum, 1989(1).